




The VACTERL (V: vertebral defects, A: anal atresia, C: cardiac defects, TE: tracheoesophageal fistula, R: renal anomalies, L: limb abnormalities) association is defined by the presence of at least three of the above-mentioned malformations. The incidence of VACTERL is low in the general population. Its aetiology is unknown, but it is attributed to the interaction between multiple genetic and environmental factors.1
The incidence of inflammatory bowel disease (IBD) in children is low, but it is characterised by a more aggressive pattern of presentation and progression compared to adults.2 The aim of this scientific letter is to report the simultaneous presentation of Crohn's disease (CD) and the VACTERL association.
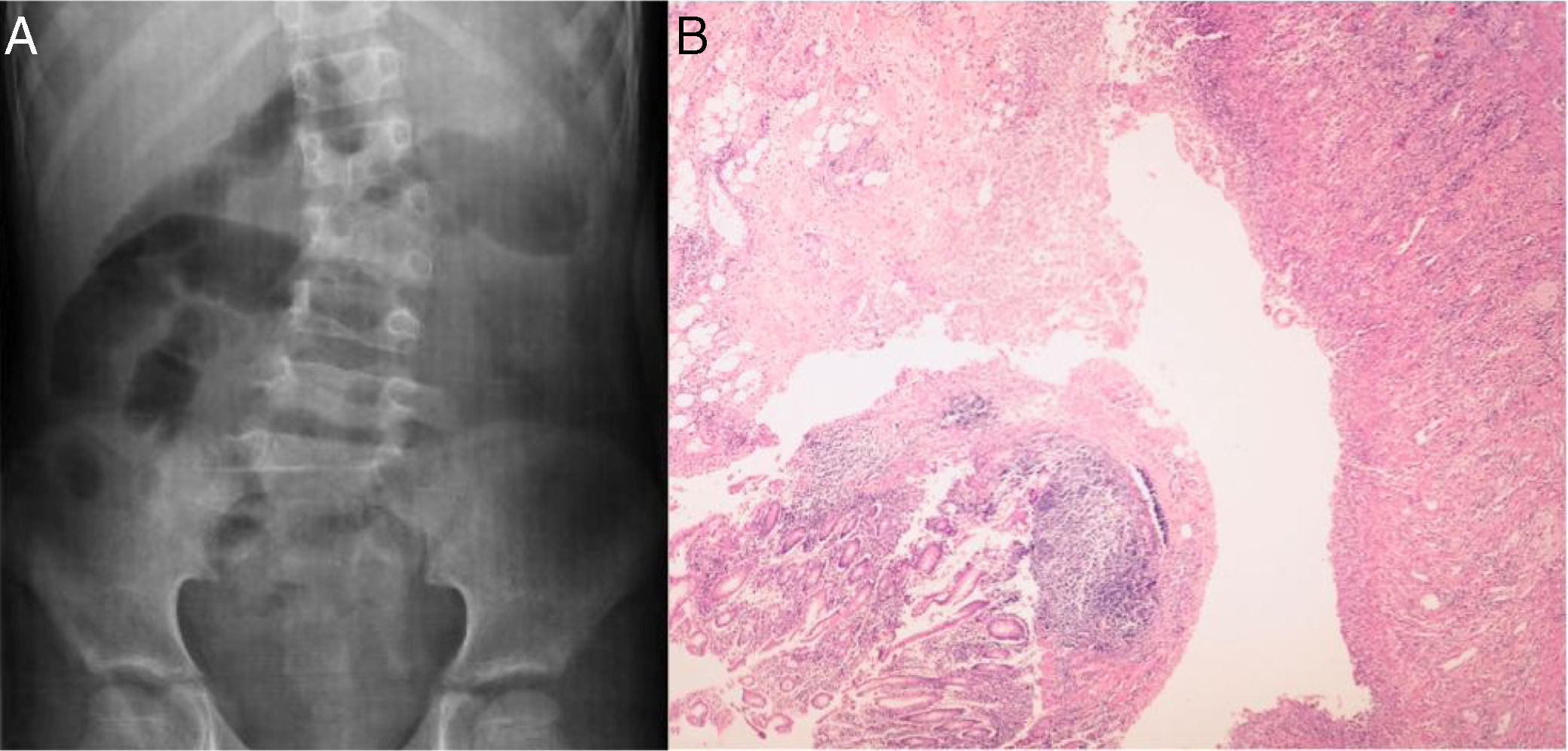
This was a six-year-old girl with a history of VACTERL association, characterised by vertebral malformations (Fig. 1A), anal atresia, cardiac defects and renal anomalies. She was brought to Accident and Emergency with rectovaginal bleeding, pain and abdominal distension. She reported asthenia and weight loss over the previous month. On physical examination, the patient was found to be malnourished and had signs of acute abdomen, for which she underwent an exploratory laparotomy. During surgery, a right hemicolectomy was performed due to multiple intestinal perforations, fistulas and severe bleeding. The colon histopathology report indicated the presence of epithelial ulceration, chronic inflammation with lymphoid aggregates and muscle hyperplasia, as well as extensive areas of fibrosis and necrosis (Fig. 1B) and CD was diagnosed, Paris classification3: A1a, L3, B3 and G0.
 Vertebral defects: scoliosis caused by hemivertebra and ankylosis of L4–L5. (B) Histopathology of the colon: ulcerated epithelium, chronic inflammation with lymphoid aggregates and muscle hyperplasia with areas of fibrosis and necrosis.")
The patient was started on treatment with mesalazine (50mg/kg/day), prednisone (1mg/kg/day) and infliximab (5mg/kg/dose, induction at weeks 0-2-6 and 2 intensification doses every 4 weeks). However, she continued to have rectovaginal bleeding and bleeding from the stoma, so the treatment was changed to azathioprine (2mg/kg/day) with adalimumab (induction dose: 80mg at 2 weeks: 40mg and weekly maintenance dose: 20mg), with significant reduction in the bleeding. Calprotectin levels were within normal limits (16μg/g [reference value: <50μg/g]). The patient is now only on adalimumab every ten days. After two years of follow-up, the bleeding has subsided, the patient has recovered her nutritional status and she has not had any adverse events from the use of the monoclonal antibody.
Our case is of special interest, as it is the first report of a patient with the aforementioned characteristics. The presentation of CD has not been linked to the VACTERL association. However, both conditions can be the result of exposure to a disease modifier in a genetically predisposed patient.
The aetiology of the VACTERL association seems to be heterogeneous; there are some genetic alterations, but they are described in a small number of patients. The environmental factors which have been associated with anorectal malformations are: maternal diabetes; infertility treatment; and exposure in the uterus to oestrogen or compounds that contain progesterone, statins or lead.1 Our patient had no history of any of these circumstances.
Some aspects of the VACTERL association have similarities with manifestations caused by mitochondrial dysfunction,4 and there are reports of cases which present both conditions. Mitochondrial function is crucial for the maintenance of the intestinal epithelium. Currently, there is no evidence of a causal association between mitochondrial dysfunction and IBD. However, some studies have demonstrated alterations in mitochondrial function within the intestinal epithelium of patients with IBD.5 This suggests that mitochondrial dysfunction in the intestinal epithelium is an integral component of the inflammatory process, through effects on epithelial permeability, interactions with the microbiota and effects on the signalling processes.5 Thus, hypothetically, the link between the VACTERL association and CD may be mitochondrial dysfunction.
This case also reveals the need for the application of current and future molecular technology in the study of patients with complex diseases, to determine the role of the genetic alterations that these diseases may present.
Please cite this article as: Peña-Vélez R, Almanza-Miranda E, Zaragoza-Arévalo GR. Enfermedad de Crohn en una niña con asociación VACTERL: ¿puede coexistir disfunción mitocondrial? Gastroenterol Hepatol. 2019;42:435–436.
