




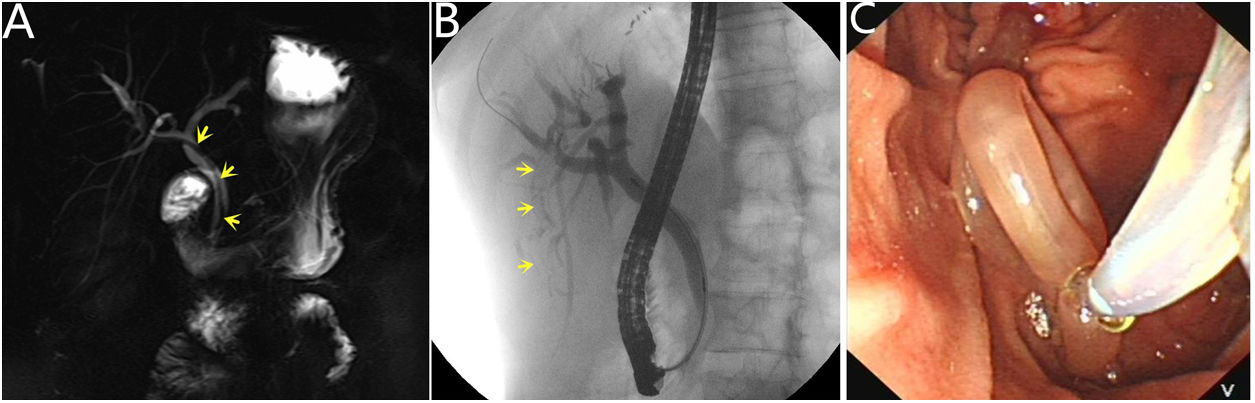
A 42-year-old female presented with a 3-day history of severe abdominal pain radiating to back, nausea and vomiting, without chills and fever. Physical examination revealed right epigastric tenderness without guarding. Laboratory test results showed total bilirubin and conjugated bilirubin level increased. Magnetic resonance cholangiopancreatography (MRCP) showed a hypo intense strip in the common and right intrahepatic bile ducts (Fig. 1A, yellow arrow). Endoscopic retrograde cholangiography (ERCP) found the ascaris had completely gone into right posterior intrahepatic bile duct (Fig. 1B, yellow arrow). We extracted the ascaris using a wire-guided basket without sphinterotomy (Fig. 1C, Video 1). The lady's pain was gone after the ascaris extraction and she was discharged two days later.
 Magnetic resonance cholangiography showed a hypo intense strip in the common and right intrahepatic bile ducts. (B) ERCP revealed a long strip filling defect in the right posterior intrahepatic bile duct. (C) The ascaris was extracted by a wire-guided basket.")
Biliary ascariasis is one of the most serious complications of gastrointestinal ascariasis. It could cause cholecystitis, cholangitis and acute pancreatitis.1 The patients may present with unbearable abdominal pain due to the onset of biliary ascriasis. The pain will relieve when the ascaris enters or exits the biliary tract completely.2 The ascaris in bile duct should be extracted and endoscopic intervention is an effective choice.3 ERCP is the main treatment for the ascaris in bile ducts. If the endoscopic treatment fails, the surgery is considered.
Financial disclosureAll authors have no financial relationships relevant to this article to disclose.
Conflict of interestAll authors have no conflicts of interest to disclose.
The following are the supplementary data to this article:
Video 1: ERCP revealed a long strip filling defect in the right posterior intrahepatic bile duct and the ascaris was extracted by a wire-guided basket without sphincterotomy.
Video text: Endoscopic extraction of intrahepatic biliary ascaris
A 42-year-old female presented with a 3-day history of severe abdominal pain. The bilirubin level increased slightly. MRCP showed a hypo intense strip in the common and right intrahepatic bile ducts. The ascaris was not visible at the duodenal papilla in duodenoscopy. After biliary intubation, cholangiography showed that no filling defect in the common bile duct. A filling defect was visible in right intrahepatic bile duct after injecting of contrast agent continuously. The guide wire was inserted into right bile duct. The basket failed to catch the filling defect. After injection of contrast agent again, a long strip filling defect appeared in the right posterior intrahepatic bile duct. The guide wire was inserted into the bile duct. The wire-guided basket was inserted into the posterior intrahepatic bile duct. The ascaris was caught and pulled out of the papilla successfully.
