





The stomach is an unusual site for metastasis, with a reported incidence in clinical and autopsy series between 0.2 and 5.4%.1–4 With improvements in prognosis of cancer, gastric metastasis are encountered more frequently. A rare cause of gastric metastasis is presented here.
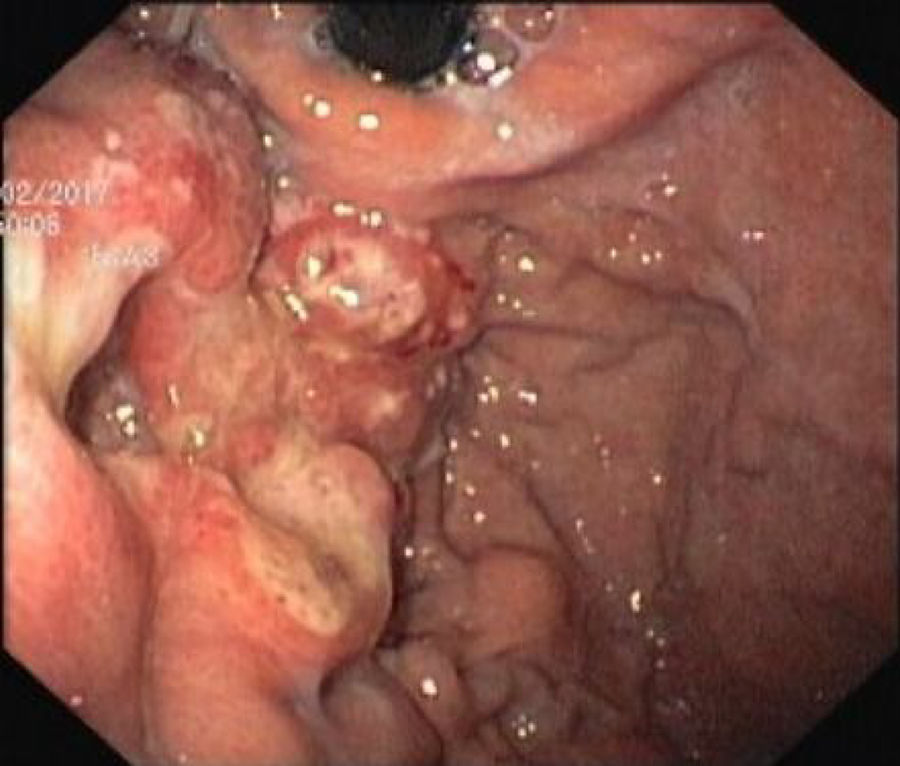
A 43-year-old female patient was hospitalized for weight loss (10kg in 2 months), asthenia and anorexia. Three years before she had been diagnosed with invasive cervical squamous cell carcinoma (high-grade intraepithelial squamous cell carcinoma) and submitted to adjuvant chemotherapy and radiotherapy. Laboratory test showed iron-deficiency anemia (Hb 8.4g/dL) and hepatic cytolysis and cholestasis (ALT 32IU/L, AST 43IU/L, GGT 301IU/L). On the second day of hospitalization she developed melena and worsening anemia (Hb 6.8g/dL). The patient underwent upper digestive endoscopy which showed on the gastric side of the cardia, an irregular, friable and ulcerated vegetative lesion occupying one-third of the circumference of the lumen. Biopsies demonstrated neoplastic cells immunoreactive for cytokeratin 14, p40 and p16, allowing the diagnosis of metastasis of carcinoma of the cervix. In addition, a thoraco-abdomino-pelvic CT scan showed liver enlargement with several solid lesions in both lobes, with a necrotic aspect, the largest with at least 16cm of the largest axis, with a cystic component; spleen with numerous solid lesions; and thickened and irregular gastric fundus wall. The diagnosis of metastatic cervical carcinoma was confirmed and, in a multidisciplinary meeting, it was decided to perform palliative chemotherapy after clinical and analytical stabilization. The patient died on the 19th day of hospitalization due to clinical worsening (Figs. 1–2).


Gastric cancer is the one of the most common malignancies in Portugal. The incidence of gastric metastasis (GM) is increasing along with the increased survival of cancer patients. The distinction between primary and secondary neoplasms of the stomach may be difficult because of its nonspecific symptoms and indistinguishable radiological and endoscopic features.
Gastric metastasis may originate from various organs, but arise predominantly from malignant melanoma (23%), breast (15%) and lung (9%) cancers.2,3 GM secondary to gynecological cancers, particularly from cervical carcinoma, are extremely rare with only a 6 cases reported in literature.1–7
The clinical presentation of GM is nonspecific and may be modified by the primary disease and the effects of treatment. Anemia and upper gastrointestinal bleeding are the most common presenting symptoms.
Given that endoscopic findings are nonspecific of metastatic disease, histologic diagnosis is mandatory.
Considering the limited number of reported cases in literature, there is not a recommended treatment for this patients. Since majority presents with concomitant metastases to other organs, this condition is often associated to a poor prognosis.
This report should increase physicians awareness to the possible existence of metastatic gastric cancer from other malignancies of solid organs.
Author's contributionEach author's contribution to the following criteria for authorship: 1, conception and drafting of the article; 2, critical revision of the article.
