




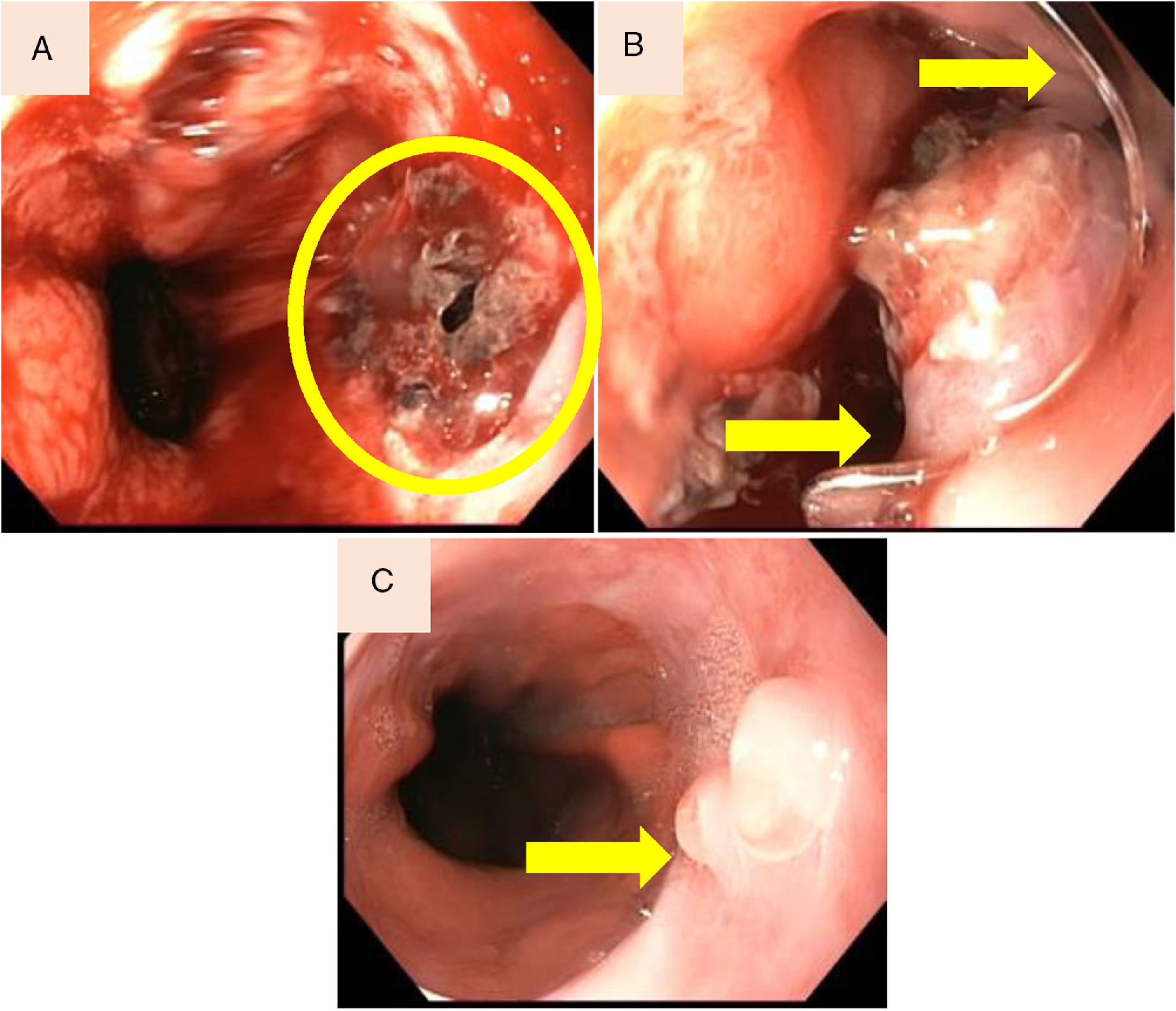
A 63-year-old man was admitted in Emergency Services 12h after vomiting and hematemesis. He was on regular treatment with antihypertensive and anti-inflammatory. Haematocrit decreased from 43% to 30%. The patient had not got any sign of sepsis with a normal chest X-ray. Urgent gastroscopy demonstrated active haemorrhage due to a 10mm oesophageal disruption located at the oesophagogastric junction (Fig. 1A). The procedure was performed at endoscopy room under deep sedation. The disruption was resolved with placement of over-the-scope clip (OTSC) (Fig. 1B). After that, the computer tomography discarded contrast leakage. The patient remained hemodynamically stable without haemorrhagic recurrence and without fever during hospitalization. He was discharged home after 72h. After 4 months of follow-up the patient remains asymptomatic. Endoscopic control demonstrated no clip at oesophageal mucosa (Fig. 1C).
 Laceration of the oesophagogastric junction. (B) Disruption resolved with placement of over-the-scope clip (OTSC). (C) Endoscopic control demonstrated no clip and granulation formation at the laceration site.")
Spontaneous oesophagus perforation (Boerhaave's syndrome) is a spontaneous disruption of the distal oesophagus associated with high mortality. Surgery repair during the first 24h from perforation is the best option.1 Surgery is associated with a high rate of mortality and morbidity. In the last years, endoscopic techniques have appeared2–4 to resolve gastrointestinal perforation. OTSC could be used for gastrointestinal perforation equal or under 10mm.
Conflict of interestThe authors declare no conflict of interest.
