




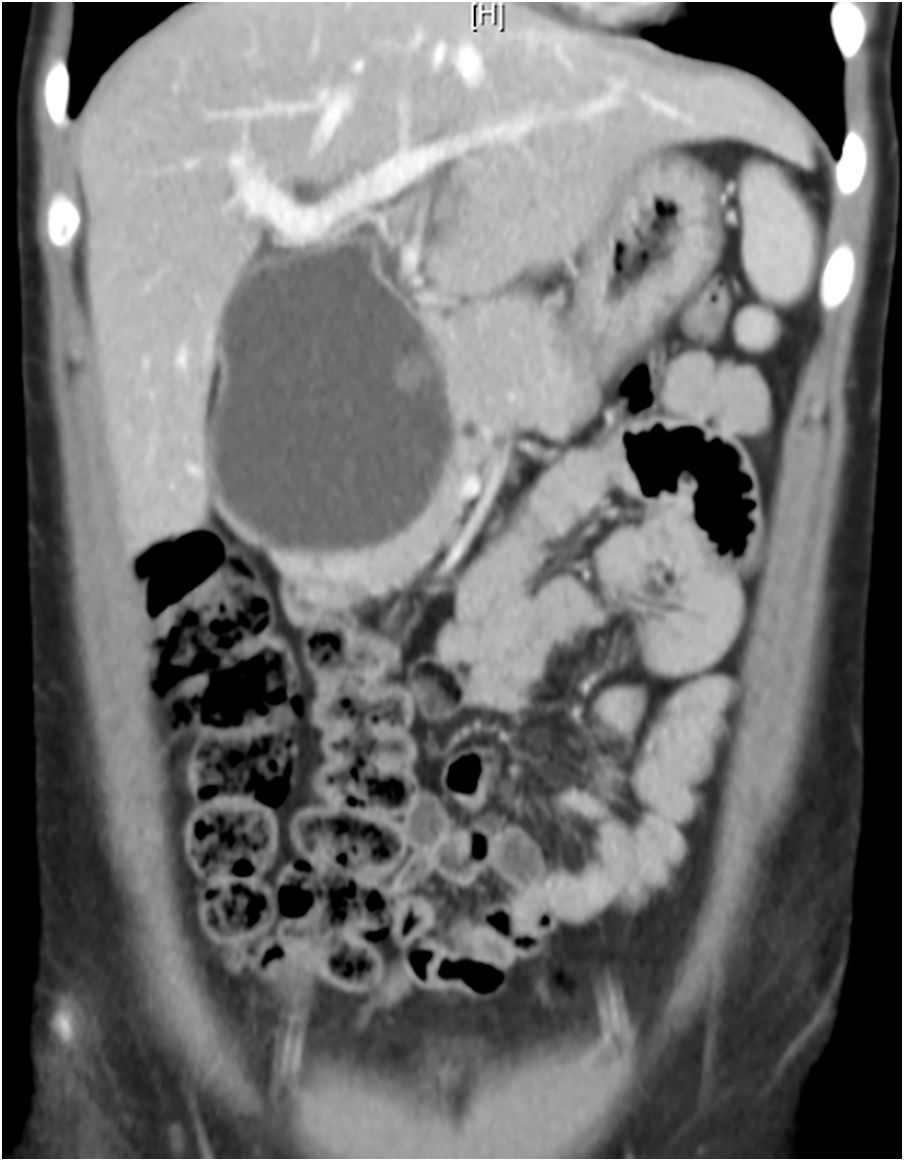

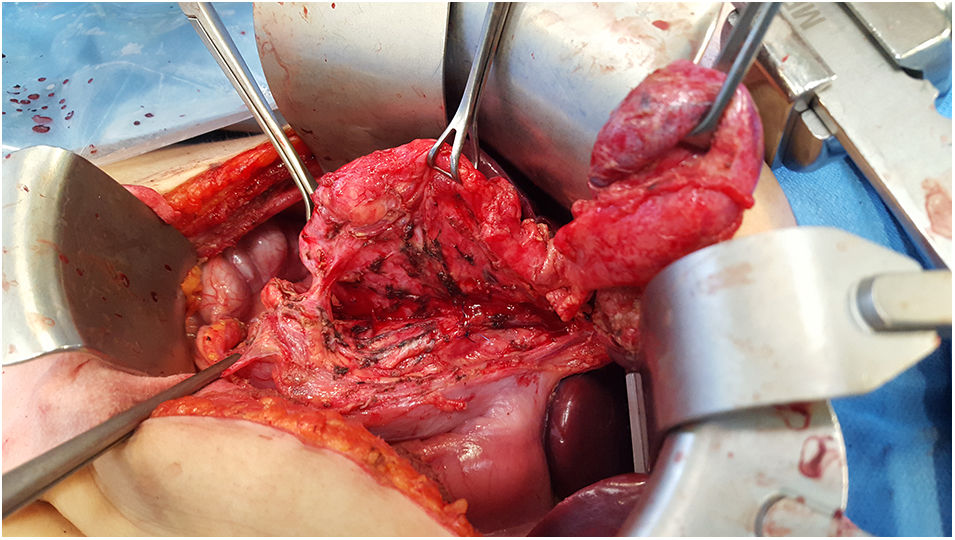
We present the case of a 20-year-old woman, with no prior history, who attended the Emergency Department due to a two-month history of abdominal pain in the right hypochondrium, which intensified in the 48 h prior, together with jaundice of the skin and mucous membranes. Blood tests were requested, which revealed total bilirubin of 20 mg/dl, as well as a CT scan that showed a bile duct tumour measuring 9.4 × 7 × 5 cm (Fig. 1). This was confirmed by bile duct MRI (Fig. 2), which revealed a type IVA choledochal cyst as per the Todani classification, with focal dilations of the intrahepatic bile duct but no involvement of the pancreatic-duodenal junction. Preoperative drainage of the bile duct was performed by transparietal transhepatic cholangiography to reduce bilirubin levels and the risk of associated cholangitis. Subsequently, the cyst was resected (Fig. 3) by Roux-en-Y hepaticojejunostomy. The histological study confirmed the presence of a choledochal cyst with fibrosis and signs of chronic inflammation with polynuclear neutrophilic and eosinophilic infiltrate, as well as intestinal metaplasia, with no signs of malignancy.

.")

Choledochal cysts are a congenital defect of the bile duct first described by Vater in 1723.1 In 80% of cases, they occur in nursing infants and small children, predominantly girls,2,3 and are rare in adults. Their incidence in Western countries ranges from one in 13,000–15,000 live births.1 Associated complications include gallstones, bile duct stenosis, cholangitis, cholangiocarcinoma, pancreatitis and biliary cirrhosis secondary to spontaneous cyst rupture. The most serious complication is the malignant degeneration of the cyst, which occurs in up to 30% of adults,4 and is most common in the extrahepatic bile duct.1,4 Given the risk of malignancy, the treatment of choice is surgical resection and reconstruction of the bile duct, either by open or laparoscopic surgery.
To date, it has yet to be presented at any congress.
Conflict of interestsThere are no conflicts of interest.
Please cite this article as: Soto-Darias IC, García-Romera Á, Rodríguez-Castellano D, Bravo-Felipe A, Alarcó-Hernández A. Quiste de colédoco gigante. Una causa inusual de ictericia obstructiva en el adulto. Gastroenterol Hepatol. 2019;42:562–563.s
