




We report the case of a 60-year-old man presenting with weight loss (15kg in the last month), lack of energy, abdominal pain and discomfort and lymphedema of the legs. He had a previous medical history of gout, systemic arterial hypertension (diseases which had been diagnosed 10 years earlier and had been medicated and controlled), and benign prostatic hyperplasia. He had prostate biopsy and appendectomy in the past. He did not smoke cigarettes and occasionally drinks alcohol. His medical family history were unremarkable. Initial investigations revealed with leukopenia, white blood cell count, 3.37/mm3 with 55.5% neutrophils, 30/mm3 eosinophils and 28.5% lymphocytes. Other blood investigations, including creatinine, electrolytes, liver function, and random and fasting blood sugar levels, were normal. Also, tumor markers such as CA19-9, CEA and AFP were in the normal range.
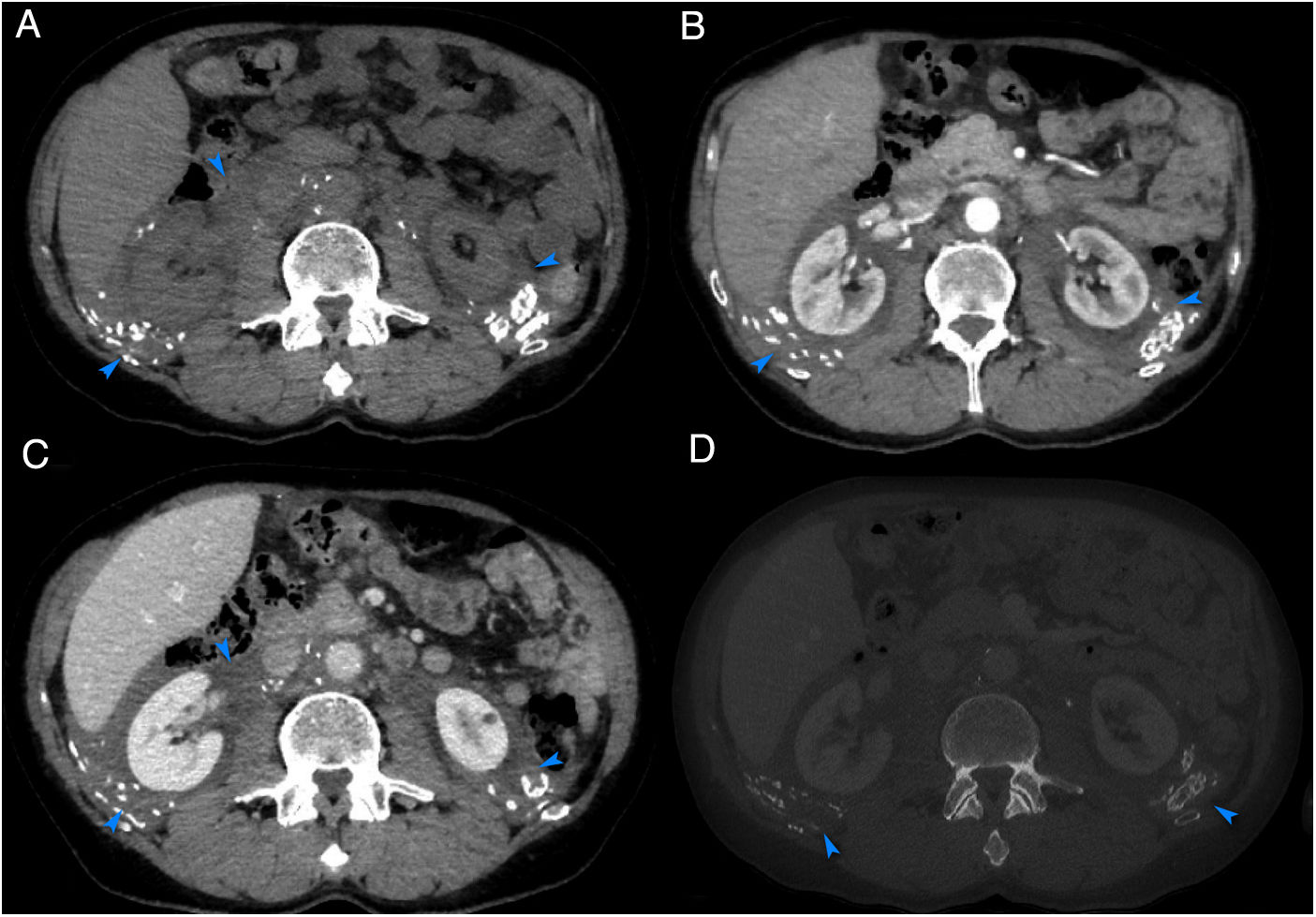
Computed tomography of the abdomen revealed massive thickening of the retroperitoneum with calcifications that encased the abdominal vessels and kidneys, but without compressing them (Fig. 1) and also, pelvic lymphadenopathy.
 showing irregular massive thickening with calcification in the retroperitoneum (arrows).")
Extensive laboratory examinations (serum and urinary protein electrophoresis) were performed, showing a monoclonal spike in the gamma region, which indicated IgG and Bence–Jones protein lambda light chains and therefore the possibility of amyloidosis was considered. Serum-free kappa and lambda chains were 36.85 and 42.90, respectively. The analysis of a biopsy of pelvic lymphadenopathy showed deposits of amorphous eosinophilic material, hyalinization and clusters of small lymphocytes. Congo red staining demonstrated amyloid deposition. Consequently, the diagnosis of lambda light chain retroperitoneal amyloidosis was confirmed by immunohistochemistry. The patient was subsequently investigated for the underlying diseases, but there was no evidence of systemic amyloidosis, plasmacytoma, or multiple myeloma. Our patient was referred to our department of haematology and subsequently started on chemotherapy with seven cycles of bortezomib 0.7mg/m2 and neofordex 40mg, and his condition improved with good drug tolerance. Currently, the patient is stable and the disease has stagnated.
Amyloidosis represents a group of diseases that occurs as a consequence of an extracellular deposition of amyloid protein in organs and/or tissues.1 Historically, it can be classified as primary and secondary or systemic.1,2 Primary amyloidosis, also known as AL amyloidosis, is a rare entity that is difficult to diagnose.1 Retroperitoneal involvement is one of the rarest forms of presentation, being a challenge, a clinical and imaging dilemma.2,3 Once the diagnosis of amyloidosis is suspected, it must be confirmed by biopsy on the affected organ, with histopathological assessment using the Congo red staining.1 Treatment is largely based on steroids and with autologous stem cell transplantation in a select group of non-responsive patients.1 Early diagnosis and treatment are essential in stabilizing the disease, thereby improving the outcome and the prognosis.1,3
AcknowledgementThe authors of this paper like to thank Cyril Faure from the Groupe Hospitalier de la Haute-Saône, Hospital of Haute Saone, Vesoul, France, Internal Medicine Department, for his contribution to the diagnosis of this case.
Conflict of interestNone.
