




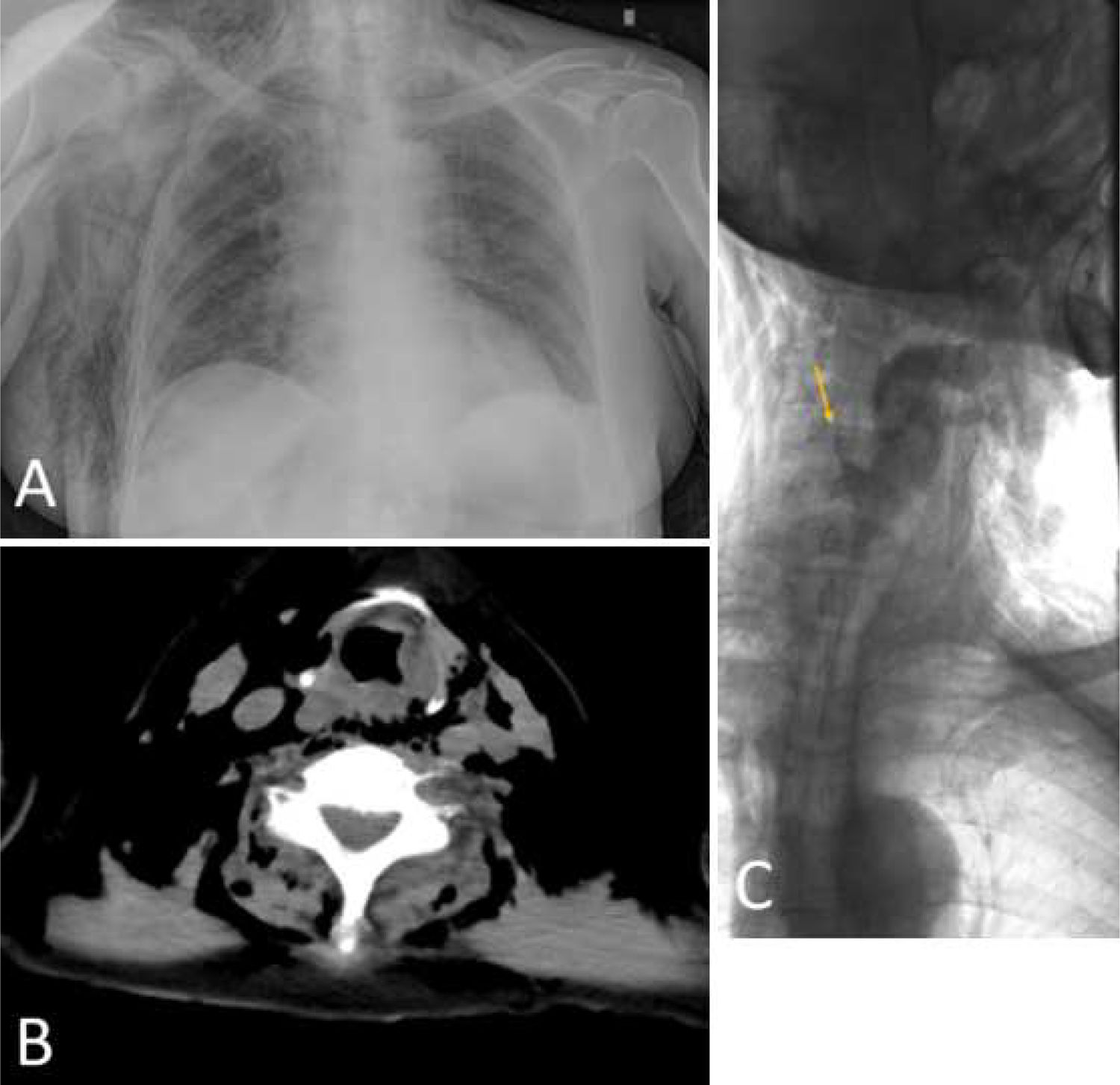
A 78-year-old female underwent endoscopic retrograde cholangiopancreatography (ERCP) for bile leakage at day 2 after laparoscopic cholecystectomy (post hoc-histology myofibroblastic tumor). After initial minimal resistance during duodenoscope introduction, ERCP confirmed cystic duct leakage. Therefore, a minimal-incision papillotomy with 10-Fr double pigtail stenting was performed. Immediately following the procedure, a cervical and right thoracic emphysema was noted, which was replicated on X-ray studies, however without evidence of free abdominal and/or retroperitoneal air. (Fig. 1A) Urgent computed tomography confirmed these findings and suggested hypopharynx perforation underlying the exuberant emphysema. (Fig. 1B) A limited contrast swallow using water-soluble gastrografin unequivocally proved a small pyriform sinus perforation. (Fig. 1C, arrow) The patient underwent a cautious CO2-insufflated EGD for guidewire placement for gently positioning a nasogastric tube. The patient was successfully treated conservatively with broad-spectrum antibiotics, initial enteral feeding and soft meals for 7 days. Duodenoscope insertion during repeat ERCP 6 weeks later was likewise performed over an endoscopically placed guidewire.
 Chest X-ray demonstrating exuberant thoraco-abdominal and neck emphysema. Note lack of free abdominal and/or retroperitoneal air. (B) CT scans likewise illustrating diffuse neck emphysema suggestive of hypopharyngeal perforation. (C) Limited contrast swallow using water-soluble gastrografin confirmative of a small pyriform sinus perforation.")
(A) Chest X-ray demonstrating exuberant thoraco-abdominal and neck emphysema. Note lack of free abdominal and/or retroperitoneal air. (B) CT scans likewise illustrating diffuse neck emphysema suggestive of hypopharyngeal perforation. (C) Limited contrast swallow using water-soluble gastrografin confirmative of a small pyriform sinus perforation.
ERCP-related perforation traditionally centers around duodenal and/or periampullary/intraductal localizations as reflected by e.g. the widely embraced Stapfer classification.1 By contrast, perforation along the duodenoscope insertion route is more uncommon, and may particularly involve the esophagus and/or hypopharyngeal structures.2 For the latter close interdisciplinary cooperation with ear-nose-throat (ENT) specialists is crucial to decide on the best individual treatment with small sinus pyriformis perforations often amenable to conservative treatment.3
Conflict of interestNothing to declare.
