




Taeniasis in humans can be related to two main species for which are the beef tapeworm, Taenia saginata, or the pork tapeworm, Taenia solium. Infected people excrete the eggs in the feces into the environment, from where those are ingested by an intermediate host (e.g. cattle). Individuals become infected by eating raw or undercooked meat containing cysticerci, leading to the sexual reproduction of the adult tapeworm in the human small bowel.1
T. solium is endemic in regions of Central and South America, sub-Saharan Africa, India and Asia, and prevalence is higher in non-urbanized areas where pigs are raised and sanitary conditions are suboptimal.2T. saginata affects 60–70 million individuals, and is considered the most prevalent zoonotic tapeworm, affecting developing and industrialized countries where consumption of undercooked beef is usual.3 A recent systematic review showed that the prevalence of T. saginata in Europe based on meat inspection was generally low (below 6.2% in 95% records) and varied between and within countries.3
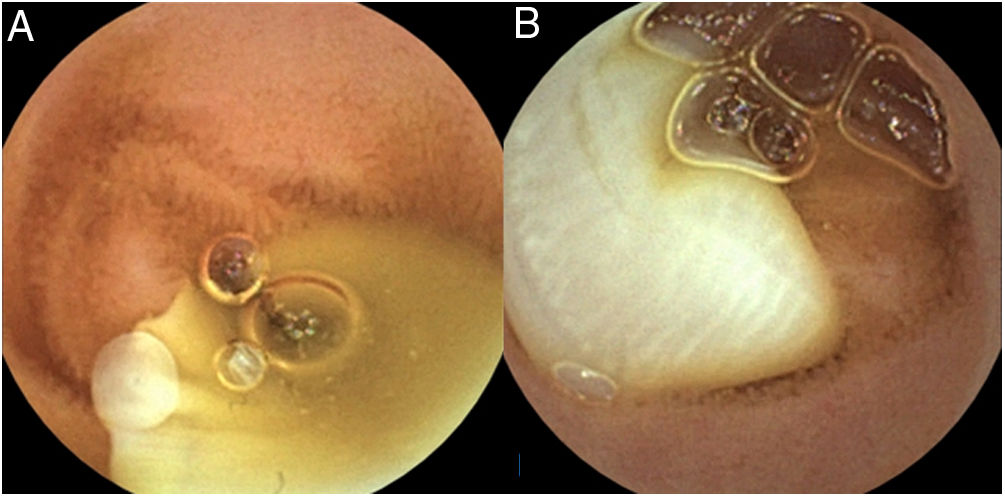
The authors present a case of a 68 year-old caucasian male with no relevant medical history, who was admitted to our hospital due to a severe microcytic and hypochromic iron-deficiency anemia (+/−6g/dL) since 1 year ago. The patient denied visible gastrointestinal bleeding or other gastrointestinal symptoms. Upper endoscopy and colonoscopy were unremarkable. A capsule endoscopy was then attempted, showing from the distal jejunum to the terminal ileum, a long, white living tapeworm, compatible of a Taeniaspp infestation (video), suggestive of T. saginata given the genital pores and the numerous (>12) uterine branches in the proglottids (Fig. 1). He admitted to eat raw or undercooked beef. The patient performed a single dose of praziquantel, resulting in resolution of anemia after therapy.
 and numerous (>12) uterine branches (B) in the proglottids, in relation to a Taenia saginata infection.")
It is important to distinguish between the two main Taeniaspecies (spp), given the risk of neurocysticercosis related with T. solium. Taenia spp has a scolex which is the head of the tapeworm, and produces proglottids. When proglottids mature, they become gravid and detach from the tapeworm to pass into stool, releasing the eggs. The scolex and the number of uterine branches on each proglottid are morphologically distinguishable between the two species. T. saginata has a scolex with no hooks and proglottids have more than 12 primary uterine branches. On the other hand, T. solium has a scolex with hooks and proglottids have less than 10 primary uterine branches.4
Patients with taeniasis may be asymptomatic or may present with nonspecific symptoms, namely abdominal pain, nausea, vomiting and weight loss. Iron deficiency anemia is rarely recognized as a manifestation of tapeworm infection (taeniasis, diphyllobothriasis, and hymenolepiasis), and only few reports of anemia have been related to taeniasis itself.5
The standard stool microscopy may not be accurate enough to detect mature Taenia proglottids and its eggs given the intermittent shedding. Moreover, other methods, as the ELISA detection of fecal Taenia coproantigens, are not universally available and may not be able to differentiate from other parasites (e.g. Ascaris and Trichuris). Although, capsule endoscopy is not the gold-standard to diagnose tapeworm infection, this method has been important for the detection and differentiation among the two species, as occurred with our patient.4
