




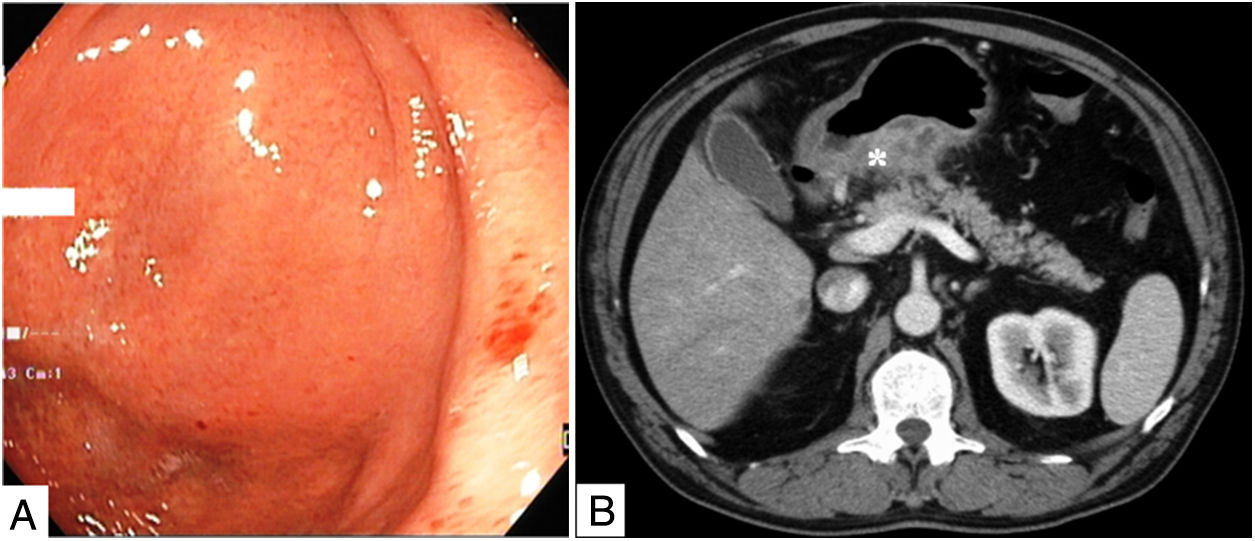
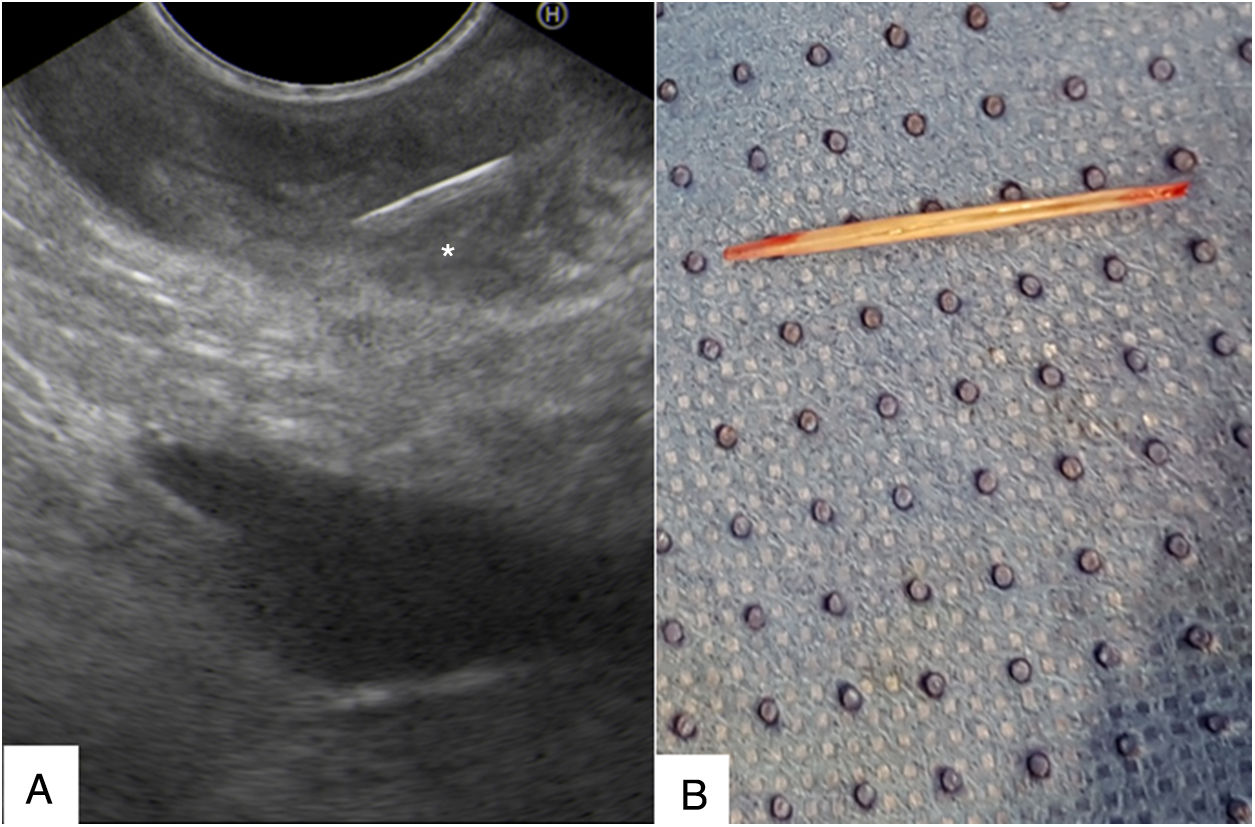
A 64-year-old man was submitted to an endoscopic ultrasound (EUS) for the evaluation of a suspected gastric neoplasia. The differential diagnosis of gastric MALT lymphoma and diffuse gastric cancer was raised after performing an upper endoscopy that revealed a subepithelial bulge of the posterior wall of the gastric antrum with erythematous mucosa (Fig. 1A) and no abnormal histopathological findings, corresponding to a diffuse gastric wall thickening with necrotic areas on abdominal CT (Fig. 1B). EUS revealed hypoechoic thickening (14mm) and loss of stratification of the posterior wall of the antrum, as well as rupture of the serosal layer with permeation to the adjacent peritoneal fat. A EUS-guided fine needle aspiration was scheduled 7 days later, but EUS findings at revaluation were markedly different: gastric wall thickening was less pronounced (up to 10mm) and circumscribed to a small area involving a linear hyperechoic image, probably corresponding to a foreign body of 20-mm length (Fig. 2A). These findings were compatible with an inflammatory reaction to a foreign body that became more circumscribed over time. An exploratory laparotomy was performed with removal of a fish bone located in the posterior wall of the gastric antrum (Fig. 2B), without any complications.
 Slight subepithelial bulge of the gastric antrum with erythematous mucosa. (B) Abdominal CT showing diffuse thickening of the posterior gastric wall with necrotic areas (*).")
 Gastric wall thickening circumscribing a linear echogenic foreign body (*). (B) Fish bone extracted from the gastric wall.")
Gastric complications following accidental foreign body ingestion are rare. Fish bones embedded in the gastric wall leading to gastric bulging and mimicking a subepithelial lesion are extremely rare, with few cases described in literature.1
