





Ulcerative proctitis (UP) presents distinctive clinical characteristics, outcomes and therapeutic approaches as compared to left-sided and extensive ulcerative colitis (UC).
AimTo describe the current therapeutic requirements and clinical outcomes in patients with active UP.
MethodsRetrospective observational study conducted in a referral IBD centre. Patients with UP in follow-up between 1989 and 2014 were included. The clinical characteristics, as well as the different treatments and drug formulations administered to treat flares, were recorded.
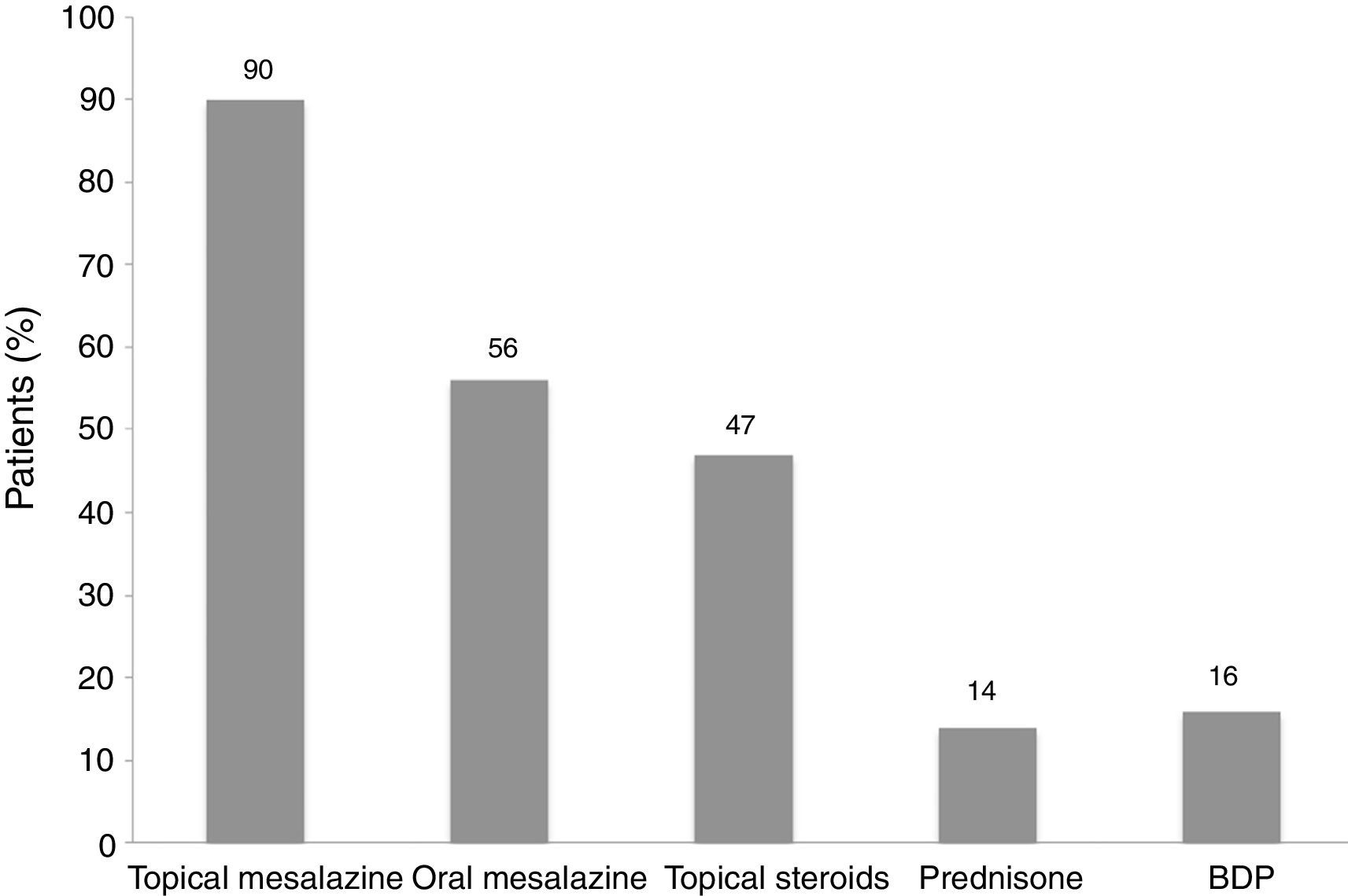
ResultsOut of 687 UC patients, 101 patients (15%) with UP were included. Median follow-up was 8 years (IQR 3–14) and 49% of patients presented disease activity during the study period. Topical mesalazine monotherapy (90%) was the most commonly administered treatment for disease activity (mostly as suppositories), followed by topical steroids (47%) and oral mesalazine (56%) in monotherapy or combination therapy. Only 14% and 16% of patients required oral prednisone and beclomethasone, respectively.
ConclusionsIn clinical practice, active UP presents mostly favourable outcomes. Mesalazine suppositories are by far the most used treatment for these patients.
La proctitis ulcerosa (PU) presenta unas características clínicas, evolutivas y terapéuticas distintas con respecto a la colitis ulcerosa izquierda o extensa.
ObjetivoDescribir los requerimientos terapéuticos y la evolución clínica en pacientes con PU activa.
MétodosEstudio observacional retrospectivo realizado en un centro de referencia en EII, en el que se incluyeron pacientes en seguimiento entre 1989 y 2014 con PU. Se registraron las características clínicas, así como los diferentes tratamientos y galénicas utilizados para tratar el brote de actividad.
ResultadosDe un total de 687 pacientes con colitis ulcerosa se incluyeron 101 (15%) con PU. La mediana de seguimiento fue de 8 años (RIC 3-14). El 49% de los pacientes presentó actividad de la enfermedad durante el período a estudio. La monoterapia con mesalazina tópica (90%) fue el tratamiento más utilizado para la actividad de la enfermedad (predominantemente en forma de supositorios), seguida de los esteroides tópicos (47%) y la mesalazina oral (56%) en monoterapia o en terapia combinada. Solo el 14 y el 16% de los pacientes requirieron prednisona oral y beclometasona, respectivamente.
ConclusionesEn la práctica clínica, los supositorios de mesalazina son el tratamiento más utilizado en pacientes con PU activa, presentando la mayoría de ellos una evolución clínica favorable.
Ulcerative colitis (UC) is a chronic, inflammatory, relapsing-remitting disease. The rectum and colon are continuously involved proximally from the anal verge. UC is classified, according to the extent of inflammation, into ulcerative proctitis (UP) when the inflammation is limited to the rectum, left-sided colitis (when it reaches up to splenic flexure), and extensive colitis (when inflammation extends beyond the splenic flexure of the colon).1 The reason for this classification relies on that disease extent determines a different disease course and prognosis. Moreover, distal forms of UC can be managed with only rectal therapies. Finally, UP has not an increased risk for colorectal cancer, allowing a less intensive disease monitoring.2
In population-based studies, UP accounts for more than a quarter of UC patients.3,4 UP usually runs a milder course as compared to more extensive disease (in terms of requirement for hospitalization, intravenous therapy, and colectomy),5 and that is the reason why medical literature has paid less attention to this minor form of UC. However, symptoms in UP (particularly, tenesmus, urgency, and incontinence) impact deeply on the patients’ health-related quality of life.
Rectal formulations, particularly mesalazine suppositories, are the first line therapy in UP since they achieve higher concentrations of active drug into the rectum and act directly to the inflamed mucosa providing better results as compared to oral formulations.6–8 Moreover, rectal formulations show a better safety profile as compared to oral treatments. However, rectal therapies are often inconvenient for the patients because of limited tolerance (particularly when the rectal mucosa is severely inflamed), or even because of the impossibility to be self-administered. These drawbacks may be relevant in some circumstances such as in elderly patients (with less anal continence and physical agility) or in patients living alone.
Although there are evidence-based arguments supporting the superiority of rectal mesalazine over rectal steroids for inducing symptomatic improvement and remission in distal UC,9 there is the belief among patients and even some physicians that steroids are more powerful (and efficient) than mesalazine.10
In addition, topical mesalazine was available later than topical steroids. In Spain, the availability of different galenical formulations and dosages for topical mesalazine (suppositories, foams, and enemas) has considerably increased within the last decade, offering a wide variety of treatment options, while topical steroids are limited to two presentations, in foam and enema.
Although the combination therapy of oral and topical mesalazine is more effective than any of them alone, there are few data reporting the efficacy of topical mesalazine and topical steroids to treat active UP.
Despite the above-mentioned literature, studies performed in real-life clinical practice and specifically in patients with UP are scarce. Therefore, the aim of the present study was to assess the different treatment options and galenical formulations used in daily clinical practice for our cohort of UP patients with active disease. As a secondary aim, the use of clinical resources and disease course were also evaluated.
Material and methodsThis was a retrospective, observational study performed at the Gastroenterology Department of the University Hospital Germans Trias i Pujol (Badalona, Catalonia). We included adult patients with UC ever limited to the rectum included in our local ENEIDA database (Estudio Nacional en Enfermedad Inflamatoria intestinal sobre Determinantes genéticos y Ambientales, a Nationwide database by the Spanish Working Group in IBD – GETECCU) who were visited in our centre from May 1989 to October 2014 with a minimum period of 3 months of follow-up.
Clinical information including baseline patient characteristics, number of disease flares, clinical outcome, and treatments provided for each episode specifying galenical formulations used, were recorded. Active UP was defined as rectal bleeding with or without other symptoms including urgency, abdominal pain, tenesmus or an increased number of bowel movements. A severe flare was defined as the requirement of intravenous steroids or colectomy to treat disease activity. Patients who presented proximal progression of the disease (to left-sided or extensive colitis) during the follow-up, were excluded.
Ethical considerationsThe Ethics Committee of our centre approved the ENEIDA Registry in December the 22th of 2006. All patients signed a written informed consent for participation.
Statistical analysisStatistical descriptive analysis was performed using the SPSS version 20.0 statistical package (SPSS Inc., Chicago, IL). Descriptive statistics were calculated as percentages for discrete data and medians with interquartile ranges (IQR) for continuous data. P-values were considered significant when smaller than 0.05. Chi square and Mann–Whitney U-tests were used for calculating discrete and continuous data respectively.
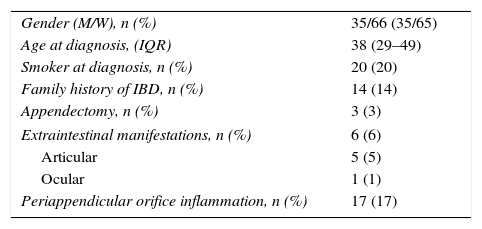
ResultsDuring the study period, 101 (15%) out of 687 UC patients registered in our local ENEIDA database were identified to have UP with no further evidence of proximal progression. Median age at diagnosis was 38 years (IQR 29–49) and 65% of patients were women. Median time of follow up in our centre was 8 years (IQR 3–14). Baseline characteristics of patients are summarized in Table 1. Among them, 49 patients presented active UP at any time during the follow-up period (median of 1 flare per patient with a maximum of 6 flares). Median time in clinical remission was 48 months (IQR 22–118). None of the baseline characteristics was associated with UP flare (data non-shown).
Baseline characteristics of the patients (n=101).
| Gender (M/W), n (%) | 35/66 (35/65) |
| Age at diagnosis, (IQR) | 38 (29–49) |
| Smoker at diagnosis, n (%) | 20 (20) |
| Family history of IBD, n (%) | 14 (14) |
| Appendectomy, n (%) | 3 (3) |
| Extraintestinal manifestations, n (%) | 6 (6) |
| Articular | 5 (5) |
| Ocular | 1 (1) |
| Periappendicular orifice inflammation, n (%) | 17 (17) |
For UP flares, rectal mesalazine in monotherapy was the most common first line treatment (90% of patients). Suppositories were the most frequent topical formulation for mesalazine (used in 96% of these patients in at least one flare). Foams and enemas of mesalazine were used in 14 and 8% of cases, respectively. Oral mesalazine (alone or in combination with topical treatment) was prescribed in 27 patients (56%), in at least one flare. Age at diagnosis and gender were not associated with the use of any specific type of these galenical formulations.
Topical steroids (budesonide or triamcinolone) were used in 23 (47%) patients (foams 83% and enemas 17%). Oral prednisone and beclomethasone were required in 7 (14%) and 8 (16%) patients, respectively. Combination with any of these drugs and their galenical formulations, was prescribed in 23 patients (47%), in most of cases after failure of topical mesalazine. The most commonly combination therapy used was topical mesalazine together with topical steroids (32%). None of the patients required intravenous steroids or anti-TNF. No cases of severe flare or colectomy were recorded. Details about different treatment options are collected in Figs. 1 and 2.


Three patients treated with mesalazine suppositories and 2 patients with topical steroids presented gastrointestinal intolerance, requiring change of the galenical formulation. None other secondary effects were recorded.
Median C-reactive protein and haemoglobin levels were within the normal ranges during active UP. Six per cent of patients attended to Emergency and only 4% required hospital admission due to UP activity.
DiscussionAlthough in population-based studies,3,4 UP represents at least a quarter of the cases of UC, in our cohort its prevalence was lower (15%) probably due to the fact that our centre is a referral tertiary hospital with the intrinsic bias of having a selected population including a higher proportion of extensive and complicated UC patients. This study analyses the disease course and treatment requirements of 49 patients (out of 101 UP patients) with active disease during a median of 8 years follow-up period.
UP has a less aggressive course as compared to more extensive forms of the disease, with lower rates of moderate-to-severe flares, systemic steroid requirement, colectomy, hospitalization or colorectal cancer risk.11,12 In our cohort no colectomy was recorded and only 4% of patients required hospitalization. The assessment of disease severity in UP patients is particularly difficult since most of patients do not present increased motions nor abdominal pain but rectal bleeding and rectal symptoms (tenesmus, incontinence). However, no specific activity index for UP is still available. Moreover, acute phase reactants usually remain within the normal range in patients with active UP. Of note, none of the flares in our cohort had raised plasmatic biomarkers (C-reactive protein and haemoglobin). Faecal calprotectin has demonstrated to be a more accurate biomarker than C-reactive protein for endoscopic activity in UC patients (and particularly in UP),13 but it was not measured in our patients.
Topical mesalazine, and particularly suppositories, are considered the first line treatment for active UP14,15 since they have demonstrated superiority against placebo for the induction of remission, as shown in several placebo-controlled trials16–20 and also confirmed in systematic reviews and meta-analysis.9,21,22 In this line, in our population, mesalazine suppositories were by far the most common first-line treatment (in 96% of patients). In a Cochrane database systematic review it was shown that, for patients receiving mesalazine suppositories, the pooled odds ratio to induce symptomatic, endoscopic and histological remission was 8.3 (95% CI 4.28–16.12), 5.3, and 6.3, respectively.9 Regarding the optimal dose of topical mesalazine, both ECCO and GETTECU guidelines recommend a dose of 1g per day, since no clear benefit with higher doses has been demonstrated.14,23 Despite that the mainstay treatment for active UP is mesalazine suppositories, in patients with poor tolerability, other rectal formulations such as foams or enemas could also be an option.24 In our cohort, only 14 and 8% of patients used mesalazine foams and enemas, respectively.
Topical steroids and oral mesalazine14,15,23 have been proposed as a second line treatment for distal UC. Second-generation topical steroids such as budesonide in rectal formulations (foams and enemas) have demonstrated also to be effective for active distal UC and UP to induce remission.24–27 Budesonide has a high topical anti-inflammatory effect and presents an important first-pass metabolism, leading to a lower incidence of systemic effects as compared to conventional steroids. In Spain, only budesonide, triamcinolone diacetate and methil-prednisolone (magistral preparation) are available. Among them, triamcinolone diacetate is one of the most commonly used as shown in our cohort. However, there is scarce data about its efficacy in UP.
Oral mesalazine (in monotherapy or in addition with topical mesalazine or steroids) could also be a second line therapy for patients intolerant to rectal therapy. Combination therapy with topical and oral mesalazine has demonstrated to be more efficient than any of these treatments alone in active UC, although no specific data for UP is available. In our population, 27 patients (56%) required oral mesalazine (alone or in combination therapy) to induce remission. In summary, topical steroids and oral mesalazine are considered a second line therapy since topical steroids have not demonstrated superiority than topical mesalazine and oral mesalazine is clearly less effective than topical mesalazine.7,28,29 In refractory patients, systemic steroids or anti-TNF could be used, but data in UP population is also scarce.30
Despite being the first line treatment for active UP, some authors suggest that topical mesalazine is underused in clinical practice, what increases the risk of clinical relapse.31 Poor adherence to treatment has been described as one of the main reasons for refractory UP; therefore physicians should always think of it in case of refractory disease and try to improve adherence in these patients. Providing with specific information on the optimal rectal administration could improve the adherence rate. This information could be given by the nurse or doctor but also by explanatory leaflets or open-access videos (e.g. GETTECU's channel on Youtube) which could be even more educational for the patients. Increasing frequency or reintroduction of previous medication could be also effective.32 Due to the retrospective design of our study and the fact of the follow-up started in 1998, we were not able to assess the real adherence, although patients seemed to have a good acceptance to topical treatment due to the high proportion of them under topical mesalazine. Moreover, some data such as the specific grade of clinical activity (mild or moderate) according to a clinical index was not possible to calculate.
Finally, this study was performed in a single tertiary centre, which might not reflect the daily clinical practice among smaller centres. Further prospective multicentre studies (including also non-tertiary) could overcome this limitation.
In conclusion, topical mesalazine (mainly suppositories) was the first line treatment in our cohort of UP patients, and oral mesalazine, topical steroids or the combination therapy remained as a second line therapy. In addition, disease course was mild with a low rate of health resources consumption and no requirement of systemic steroids or anti-TNF treatment.
Conflict of interestsThe authors have no conflict of interests.
