


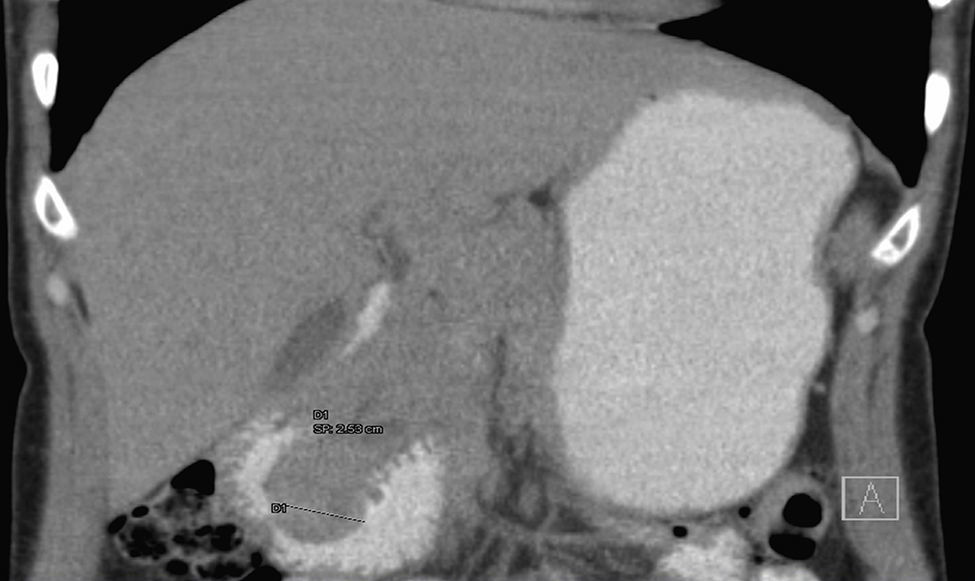
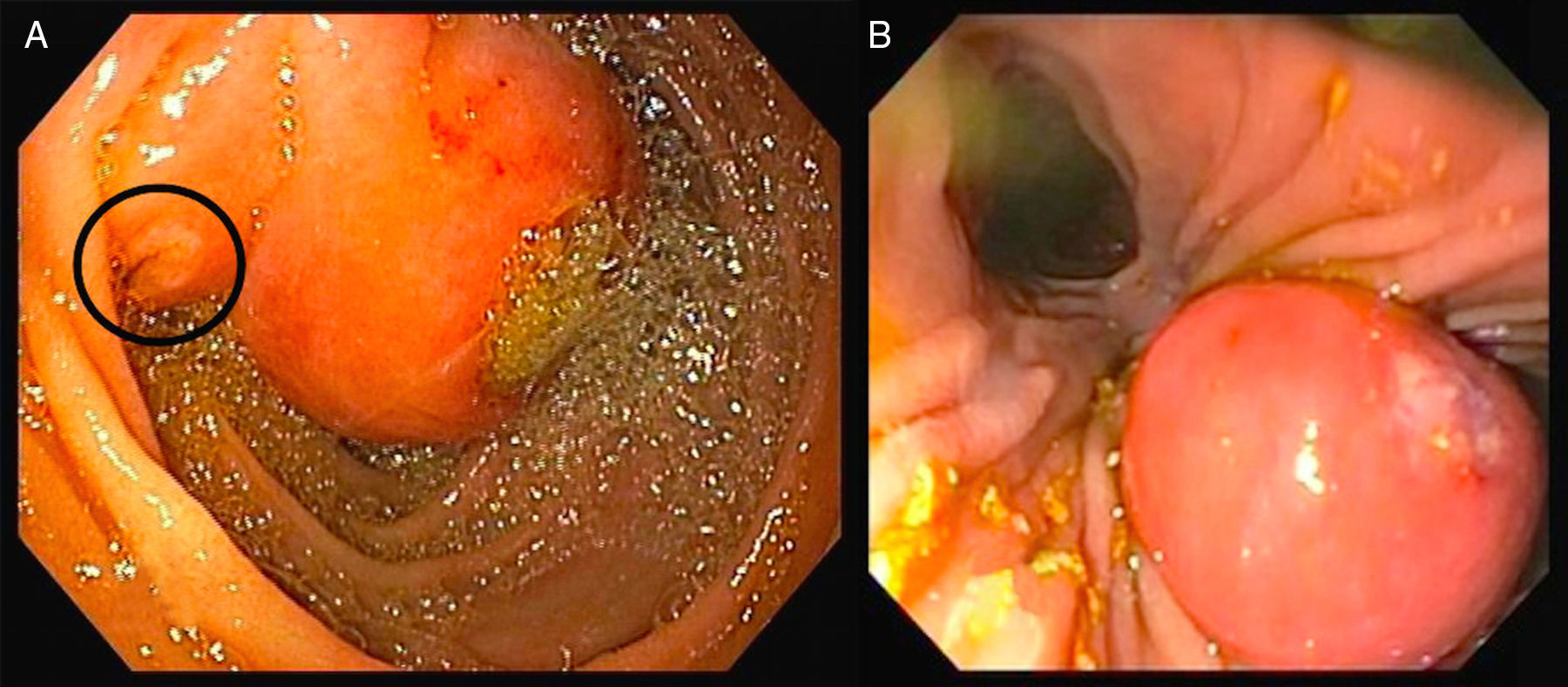
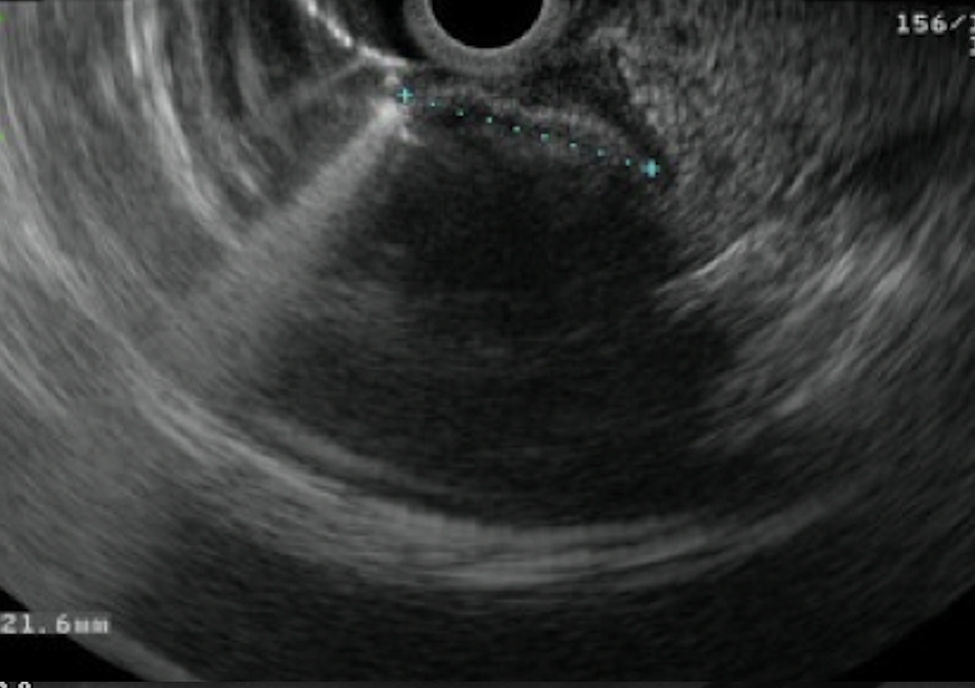

A 39-year-old female with no significant past medical history presented with intense epigastric, colic pain for the three previous days. Laboratory studies showed mild and isolated C-reactive protein (CRP) elevation (1.9mg/dL); liver function tests and pancreatic enzymes were within normal range. An abdominal computed tomography (CT) was performed and revealed a duodenal (D2/D3) endophytic polypoid, high density, heterogeneous lesion, with 26mm; biliary tree and pancreas were normal (Fig. 1). Upper endoscopy (Fig. 2A) and duodenoscopy (Fig. 2B) identified a 25mm large subepithelial lesion, distal to the duodenal papilla (black circle in Fig. 2A), with ulcerated top, suggestive of gastrointestinal stromal tumor (GIST). Endoscopic ultrasound (EUS) examination confirmed a peripapillary subepithelial lesion with 22mm and massively calcified, with posterior acoustic shadowing (transition zone undefined) (Fig. 3); the common bile duct was normal.
 endophytic polypoid, high density, heterogeneous lesion, with 26mm.")
 Upper endoscopy; (B) duodenoscopy: 25mm large subepithelial lesion, distal to the duodenal papilla (black circle in A), with ulcerated top.")

In this patient, EUS findings raised the diagnostic suspicion of a gallstone impacted in the duodenal wall through a peripapillary bilioenteric fistula. Therefore, duodenoscopy was repeated at day 6 but, instead of the lesion previously seen, there was now a large peripappilary orifice, suggestive of a bilioenteric fistula (40mm large after contrast injection and guide-wire exploration) (Fig. 4). There was spontaneous and complete abdominal pain remission in less than a week after admission.
.")
The case presented was particularly challenging as the endoscopic and imagiologic appearance mimicked that of a calcified subepithelial lesion with ulcerated top, such as GIST. Most common subepithelial lesions found in the duodenum are GIST, leyomiomas, lipomas and carcinoids and EUS plays a major role in the differential diagnosis. These lesions may occasionally show calcification, usually focal or punctate.1 However, massive calcification is extremely rare (it has been described in few cases of GIST)1 and may point to an alternative diagnosis such as an impacted gallstone into the duodenal wall, particularly if found in D2. There are only three published case reports of parapapillary fistula with impaction of a gallstone into the duodenal wall.2,3
Conflicts of interestThe authors have no conflicts of interest to declare.
DisclosuresAll authors have approved the manuscript and agree with its submission to GE – Portuguese Journal of Gastroenterology. All authors have nothing to disclose.
Author contributionsSusana Marques did the writing of the manuscript. Pedro Pinto-Marques and David Serra were responsible for the revision of its contents.
