


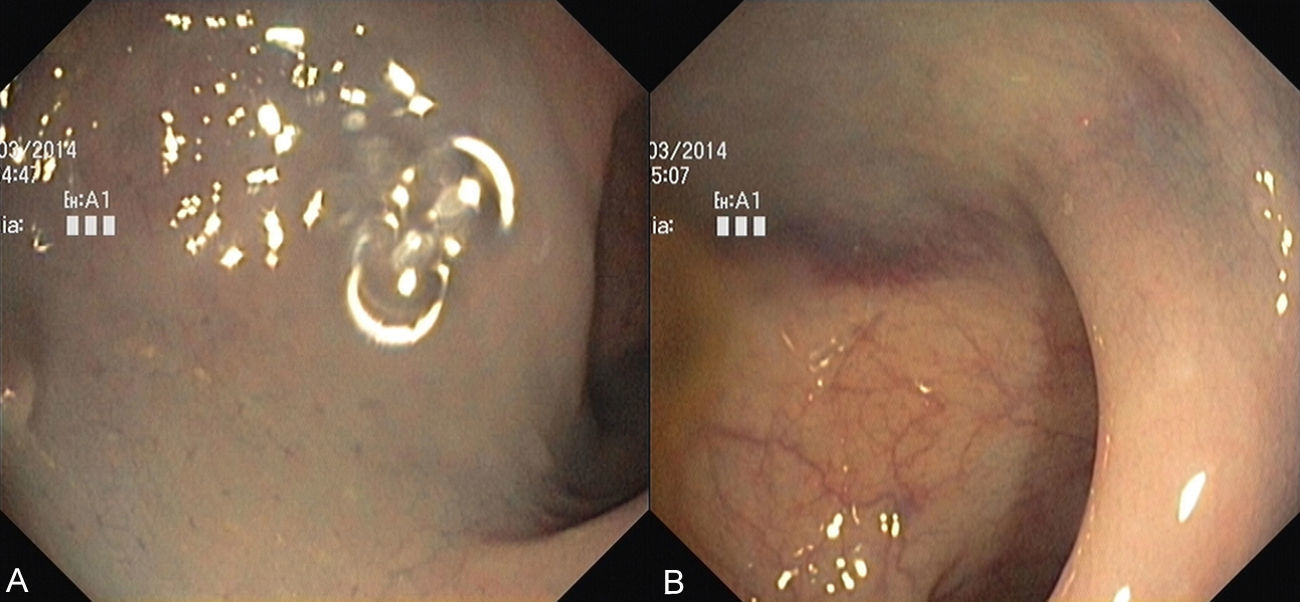

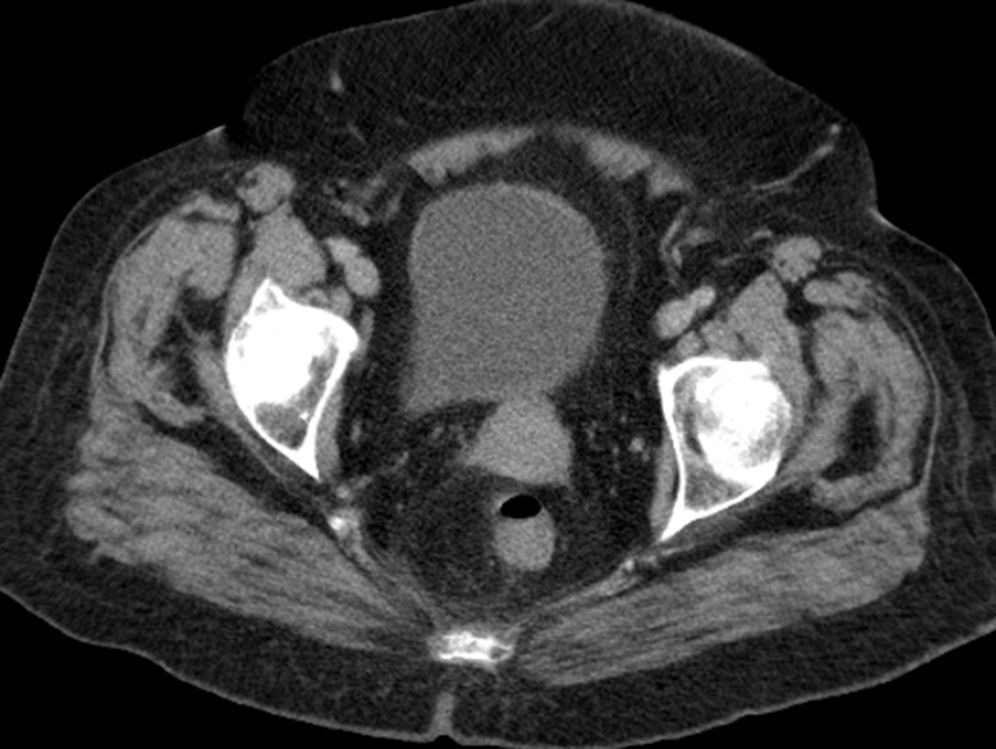
An 84-year-old woman presented with a 2-day history of rectal bleeding. Physical examination revealed no signs of peritoneal irritation and digital rectal examination revealed no palpable masses although there was blood on the glove. Laboratory tests showed a haemoglobin level of 10.9g/dL, a platelet count of 182,000/uL and an international normalised ratio of 1.11. Sigmoidoscopy revealed congestive internal haemorrhoids and a large haematoma on the right rectal wall extending 10cm from the anal verge, with no signs of active bleeding into the lumen (Fig. 1A and B). Computed tomography (CT) revealed perirectal air and densification of adjacent fat, mainly in the right side of the rectum, suggesting perforation (Figs. 2 and 3). Upon anamnesis review, the patient recalled development of perianal pain a few hours after administration of the cleansing enema by a trained nurse in left lateral decubitus and denied history of recent trauma before admission, antiplatelet or anticoagulant therapy. Complete resolution of symptoms and CT findings occurred after eight days of conservative management with intravenous antibiotics and intestinal rest, after which oral nutrition was started. The patient received two more days of ciprofloxacin and metronidazole and was discharged on the eleventh day.
, extending 10cm from the anal verge (B), with no signs of active bleeding.")


Intramural hematomas may occur throughout the gastrointestinal tract, but rarely affect the rectum. Most rectal intramural hematomas are secondary to blunt trauma. Non-traumatic spontaneous hematomas may result from anticoagulant therapy and hematologic diseases.1
Rectal perforation after administration of cleansing enemas has rarely been reported.2 Enema tips have different size, format and material, but all may induce severe injury. Unless the infusate is irritating, pain do not occur immediately after rectal perforation, which may delay the diagnosis.3,4 Administration of rectal cleansing enemas should be performed with gentle insertion and adequate lubrification.2,4 Furthermore, the patient should be in the left lateral decubitus position while the enema tip is inserted.2,5 As our patient had no risk factors to develop rectal haematoma and the symptoms occurred after the administration of the cleansing enema, the perforated rectal haematoma was assumed to be iatrogenic.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Grant supportGrant Support was not provided for this article.
Conflict of interestThe authors have nothing to disclose.
