







A national report has indicated that a high percentage of youths in the USA (aged 6 to 17 years) was prescribed to wear eyeglasses/contact lenses (Rueben, 2021). Interestingly, the prevalence was higher among girls than boys. In boys, the prevalence was 20.0 % among those aged 6–11 years and 35.3 % among those aged 12–17 years, whereas these rates were 26.4 % (6–11 years) and 48.2 % (12–17 years) among girls (Rueben, 2021). Such high prevalence of prescribed eyeglass/contact lenses was also observed in other countries or regions. For example, a large-scale study with school-aged children in the United Kingdom pointed towards an increased prevalence of prescribed eyeglasses for myopia from 2009 (24 %) to 2017 (32 %) (Wong & Dahlmann-Noor, 2020). Besides, nearly 53 % of Chinese school-aged children who were diagnosed with refractive errors were prescribed to wear corrective lenses or glasses (Chen et al., 2021). Consequently, the widespread need for prescribed glasses or contact lenses has emerged as a global public health concern.
Notably, children and adolescents with prescribed eyeglasses/contact lenses were more likely to experience negative emotions and report poorer adaptive skills as compared to normal sighted peers, a relationship that was observed in various countries (e.g., China and United States) (Alimovic, 2013; Koenes & Karshmer, 2000; Mohamed et al., 2019; Runjić et al., 2015; Xu et al., 2020) . Collectively, the health issues of children prescribed with eyeglasses/contact lenses can be categorized into internalizing and externalizing problems (Brown & Prinstein, 2011). Specifically, children prescribed with eyeglasses/contact lenses often encountered more or less difficulties in self-perception and negative judgments from their peers (Holguin et al., 2006; Jellesma, 2013; Yabumoto et al., 2009), which may in turn result in higher levels of internalizing problems (depressive symptoms) (Abolfotouh & Telmesani, 1993) and increased level of anxiety (Augestad, 2017). Additionally, previous studies indicated that children prescribed with eyeglasses/contact lenses, as compared to their normal sighted peers, exhibited higher levels of behavioral problems (e.g., irritability and noncompliance) (Aghai et al., 2016; Kara et al., 2023), which might be attributable to the fact that they have fewer opportunities to develop their social skills in comparison to their peers without visual correction (Lifshitz et al., 2007). Thus, these unfavorable consequences could overshadow the benefits derived from improved vision (Guan et al., 2018).
A growing body of research has identified modifiable factors that might help to improve mental health problems and maladaptive behaviors among persons with visual problems (e.g., myopia and visual impairment) (Hou et al., 2023; Zhao et al., 2023). Notably, this research has advocated the beneficial effects of maintaining health behaviors (e.g., 24-Hour Movement Behavior [24-HMB] guidelines) on health outcomes, including the above-mentioned aspects of internalizing and externalizing problems (Tremblay et al., 2016). The 24-HMB guidelines are composed of different components including physical activity (PA), sedentary behavior (typically referring to screen time [ST]), and sleep duration (SL) within the 24-hour diurnal cycle. More specifically, 24-HMB guidelines have recommended that children and adolescents should aim for at least 60 min of moderate-to-vigorous-intensity PA (MVPA) per day, limit recreational ST to no more than 2 h per day, and ensure getting 9 to 11 h of sleep per night if they are aged 5 to 13 years, or 8 to 10 h if they are aged 14 to 17 years (Tremblay et al., 2016).
Previous studies have examined associations of meeting 24-HMB guidelines with some aspects of internationalizing and/or externalizing problems among different age groups (e.g., preschoolers, youths, and emerging college students) with healthy or clinical condition (Bu et al., 2021; Hou et al., 2023; Ohta et al., 2023; Patte et al., 2020; Sampasa-Kanyinga et al., 2021; Zhu et al., 2023). For instance, a cross-sectional study indicated that meeting all three components of 24-HMB guidelines was linked to fewer internalizing and externalizing problems among preschoolers aged 3–6 years (Zhu et al., 2023). Additionally, baseline data of the Adolescent Brain and Cognitive Development study indicated that meeting ST+SL guidelines was linked to a lower risk of developing internalizing and externalizing problems among 11,875 children aged 9–11 years (Sampasa-Kanyinga et al., 2021). Further, study findings indicated that meeting 2 or 3 integrated components of 24-HMB guidelines was more strongly linked to the above-presented measures in relation to meeting one single guideline or not meeting any of the 24-HMB guidelines (Sampasa-Kanyinga et al., 2021). Notably, a recent study in visually impaired children and adolescents indicated associations between meeting integrated components of the 24-HMB guidelines with emotional (e.g., anxiety and depression) and social functioning (e.g., difficulty making friends and bullying others) (Hou et al., 2023). Thus, based on previous findings, it seems reasonable to suggest that the health benefits from maintaining healthy movement behaviors could be applied to children and adolescents of prescribed with eyeglasses/contact lenses.
We hypothesized that in children and adolescents prescribed with eyeglasses/contact lenses, (i) the prevalence of meeting 24-HMB guidelines, especially meeting the integrated guidelines, is relatively low, (ii) meeting both independent and integrated components of the 24-HMB guidelines are beneficially linked to aspects of internalizing and externalizing problems, and (iii) meeting two or three components of the 24-HMB guidelines is more strongly linked to the above-presented outcomes relative to meeting one single component or none of 24-HMB guidelines. The results of this study will offer valuable insights and have the potential to contribute to evidence-based recommendations for children and adolescents prescribed with eyeglasses/contact lenses both in educational settings and healthcare environments.
MethodsData resourceData were obtained from the nationally cross-sectional dataset of the 2021 National Survey of Children's Health (NSCH). This national survey employs a structured, multistage sampling procedure to reflect the demographic composition of noninstitutionalized children and youth aged 0–17 years in each state. Detailed information on the survey design and ethical approval is available in Supplementary material. Caregivers provided relevant information about the participants' movement behaviors and the variables of interest through questionnaires. This study specifically targets (i) individuals aged 6 to 17 and (ii) those who were being prescribed eyeglasses/contact lenses (Has an eye doctor prescribed eyeglasses/contact lenses in the past 2 years?). Notably, the responses were categorized into three options: (i) An eye doctor has prescribed eyeglasses/contact lenses; (ii) The child/adolescent saw an eye doctor, but did not receive a prescription; (iii) The child/adolescent did not see an eye doctor. Children and adolescents who fell into category 1 were included in this study.
Exposure variables: 24-Hour movement behaviorsAs previously mentioned, 24-HMB guidelines comprise three components (PA, ST, and SL). Single-item questions were used to determine if a child/adolescent met the 24-HMB guidelines: (i) To assess PA, parents were asked: “Over the past week, how many days did your child engage in exercise, sports, or physical activity for at least 60 min?” Four response options were offered: 0 days, 1–3 days, 4–6 days, and every day. (ii) To assess ST, parents were asked: “On most weekdays, how much time does your child typically spend watching TV, using electronic devices, or engaging in online activities not related to school?” Five response options were offered: Less than 1 h per day, 1 h per day, 2 h per day, 3 h per day, and 4 or more hours per day. (iii) To assess SL, parents were asked: “During the past week, how many hours of sleep did your child usually get on weeknights?” Seven response options were offered: Less than 6 h, 6 h, 7 h, 8 h, 9 h, 10 h, and 11 h or more. Notably, the SL guideline varied slightly across age groups: (i) 5 to 7 for 5-to 13-year-old children; (ii) 4 to 6 for 14-to-17-year-old adolescents. Participants who met all three 24-HMB guidelines were coded as 1, whereas those who did not met the 24-HMB guidelines were coded as 0. Such coding procedures were used in previous studies (Hou et al., 2023; Kong et al., 2023; Taylor et al., 2023; Zhao et al., 2023). Both categorical (PA, ST, SL, PA+ST, PA+SL, ST+SL, PA+ST+SL) and continuous (e.g., 0–3) number of 24-HMB guidelines were used in this study.
Outcome variables: internalizing and externalizing problemsTwo separate single-item questions (Does your child currently have depression or anxiety problem?) were used to measure depression and anxiety as key components of internalizing problems. Three response options are used as follows: (i) No current condition; (ii) Previously informed, but not currently affected; (iii) Currently affected. Six aspects of externalizing problems were measured via single-item questions, including behavioral problems, arguments, defiant behavior, social difficulty, care difficulty, and bullying behaviors. Behavioral problems were assessed with the following question: “Does your child currently have behavior problems?” Responses options were: (i) Does not have the problem, (ii) Ever told, but no currently affected, and iii) Currently affected. Arguments were assessed with the following question: “How often does your child argue too much?” Four response options were given: (i) Always, (ii) Usually, (iii) Sometimes, and (iv) Never. The score on response frequency was a reverse code, with higher scores indicating greater frequency of arguments. Defiant behavior, described as actions that bother the caregiver, was assessed with the following question: “During the past month, how often have you felt that your child does things that really bother you a lot?”. Response options were: (i) Never, (ii) Rarely, (iii) Sometimes, and (iv) Usually/always. Social difficulties, difficulty of making friends was measured via the following question: “Compared to other children of the same age, how much difficulty does your child have making or keeping friends? Three response options existed: (i) No difficulty,(ii)A little difficulty, and (iii) A lot of difficulty. Care difficulty was assessed with the following question: “During the past month, how often have you felt: That this child is much harder to care for than most children their age?” Responses were selected from four options: (i) Never, (ii) Rarely, (iii) Sometimes, and (iv) Usually/always. Finally, bullying behavior was evaluated with the following question (“During the past 12 months, how often did this child bully others, pick on them, or exclude them?” Five response options were presented: (i) Never, (ii) 1, 2 times in the past 12 months, (iii) 1, 2 times per month, (iv) 1, 2 times per week, and (v) Nearly every day.
CovariatesThe selection of covariates was informed by previous research (Williamson et al., 2021), including age, sex, ethnicity, premature birth (born ≥3 weeks before due date), overweight (yes vs. no), household federal poverty level (FPL), mental well-being of both parents (1 = excellent or very good, 2 = good, and 3 = fair or poor), and educational background of primary caregivers (1 =less than high school education, 2 = high school or General Educational Development(GED), 3 = some college or technical school, 4 = college degree or higher). In line with previous research (Hou et al., 2023; Kong et al., 2023; Zhao et al., 2023), FPL was categorized into 2 levels, which in turn generated two categories: (i) 0 = 0 %–99 %; (ii) 1 = 100 % and more.
Statistical analysesStatistical analyses were conducted using Stata 17 (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC). To ensure the accuracy of the findings, we applied sampling weights to the survey data. This weighting was based on stratification, considering the state of residence and households with children and adolescents. We further stratified by assigning a unique household identifier, creating a new variable called "STRATACROSS." For the presentation of our data, we provided descriptive statistics for all variables. Continuous data were summarized as mean and standard deviation (SD) and categorical data included unweighted sample counts and weighted percentages for each category. Multi-variable logistic regression analyses were used to examine and assess the association between meeting 24-HMB guidelines and outcomes of interest (internalizing and externalizing problems), with odds ratios (OR) reported at a 99.5 % confidence interval (CI). The present study aimed to determine whether meeting 24-HMB guidelines in both continuous and categorical manners were linked to lower risk of developing (internalizing and externalizing problems as dependent variables. Additionally, age, sex, ethnicity, household income, premature, the highest educational level of caregivers, and the mental health status of both the mother and father were factored in as covariates within the logistic regressions. Individuals with missing data were excluded for data analyses, followed by sensitivity analyses for inclusion of missing data (generating similar results, which are not presented in this study). To determine statistical significance with more conservative cutoff, p ≤ 0.005 for all analyses was used as the Bonferroni adjustment (0.05 divided by 8 dependent variables = 0.00625) can address the issue of multiple comparisons.
ResultsParticipant characteristicsInitially, 9315 participants were identified with prescribed eyeglasses/contact lenses. Participants who did not answer the questions for the 24-HMB guidelines and/or the selected outcome measures were removed, resulting in 6030 participants with prescribed eyeglasses/contact lenses (n = 2799 girls), with a mean age of 12.79 ± 3.1 years. The weighted population size was 8942,196. Regarding ethnicity, 4053 participants were categorized as White (weighted percentage: 53.5 %). The number of children and adolescents with premature birth was 697 (weighted percentage: 11.7 %), whereas 617 children and adolescents (weighted percentage: 12.4 %) were classified as overweight or obese. A total of 537 participants (weighted percentage: 14.1 %) had a FPL of 0 %–99 %. An overview and more detailed information about the characteristics of the present sample can be found in Table 1.
Participants characteristics (N = 6030).
Note: N represents unweighted sample counts and% is weighted sample sizes; GED = General Educational Development; FPL = federal poverty level.
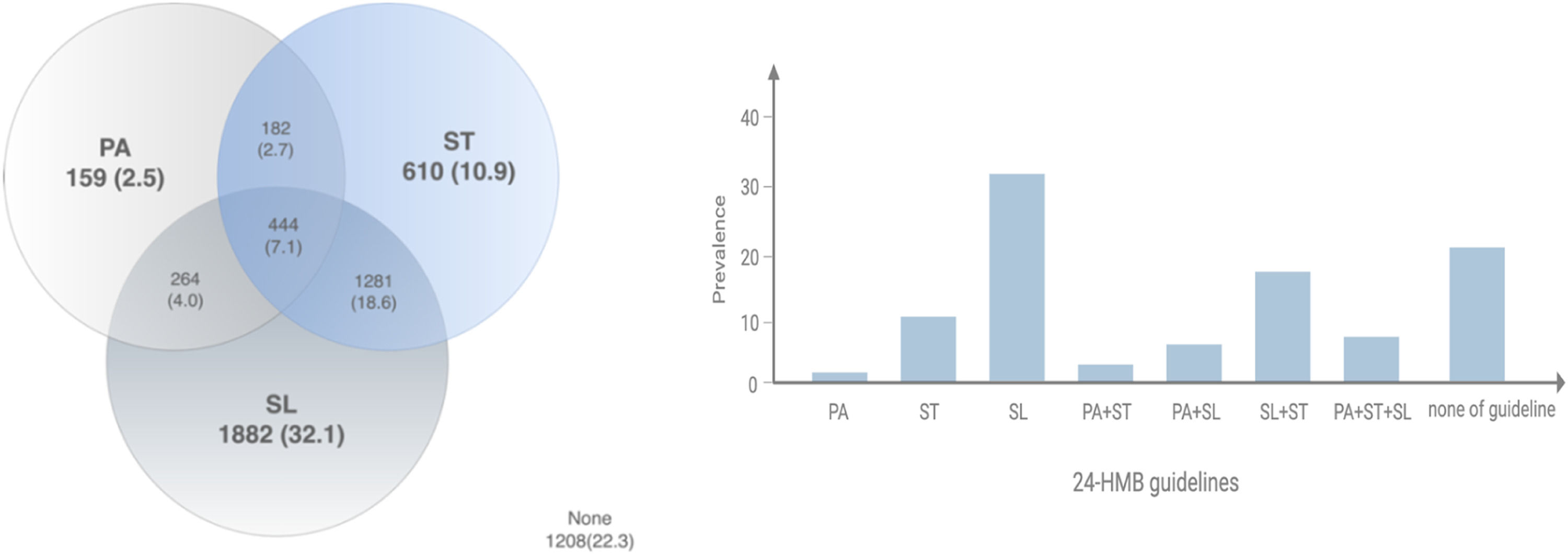
In total, 22.3 % of the participants did not meet any of three 24-HMB guidelines whereas 45.5 % participants met a single guideline (PA = 2.5 %, ST = 10.9 %, and SL = 32.1 %) (Fig. 1). Additionally, participants who met two and three integrated guidelines have reached 32.4 % (PA + ST = 2.7 %, PA + SL = 4.0 %, and SL + ST = 18.6 %, PA + ST + SL = 7.1 %). Information on weighted percentage and frequency are detailed in Supplementary Table A2.
Internalizing problems of meeting 24-Hour movement behavior guidelines (N = 6030): PA = physical activity, SL = sleep, duration, ST = screen time. None = meet none of guidelines, ALL = meet PA + ST + SL guidelines.")
Meeting at least one of 24-HMB guidelines was significantly linked to lower odds of depression (OR=0.6, 99.5 % CI [0.4–0.8]). As shown in Fig. 2, compared to meeting none of 24-HMB guidelines, meeting at least two (PA + ST: OR=0.1, 99.5 % CI [0–0.6]; PA + SL: OR=0.2, 99.5 % CI [0.1–0.8]; ST + SL: OR=0.4, 99.5 % CI [0.2–0.8]) or all three of 24-HMB guidelines (OR=0.2, 99.5 % CI [0.1–0.4]) was significantly linked to lower odds of depression as reported by the caregiver.

Associations of meeting 24-HMB guidelines with internalizing and externalizing problems among children and adolescents with prescribed eyeglasses/contact lenses. "-" indicates statistical non-significance. The specific numbers represent odds ratios and 99.5 % confidence intervals, indicating a negative correlation between meeting 24-HMB guidelines with aspects of internalizing and externalizing problems. Running figure = physical activity; TV = screen time; Moon = sleep duration.
Similarly, the number of children and adolescents meeting at least one of 24-HMB guidelines was significantly linked to lower odds of anxiety (OR=0.7, 99.5 % CI [0.6–0.9]). As highlighted in Fig. 2, compared to meeting none of 24-HMB guidelines, meeting integrated guidelines (ST + SL: OR=0.4, 99.5 % CI [0.3–0.7]; PA + ST + SL: OR=0.4, 99.5 % CI [0.2–0.9]) was significantly linked to lower odds of anxiety.
Externalizing problemsNo significant associations were found between meeting 24-HMB and behavioral problems (see Fig. 2). Nevertheless, meeting 24-HMB guidelines was significantly linked to lower odds of arguments (OR=0.8, 99.5 % CI [0.7–0.9]) and defiant behaviors (OR=0.8, 99.5 % CI [0.7–1.0]). As shown in Fig. 2, as compared to meet none of 24-HMB guidelines, meeting PA + ST guidelines was significantly linked to lower odds of defiant behaviors (OR=0.4, 99.5 % CI: [0.2–0.9]) and arguments (OR=0.4, 99.5 % CI: [0.2–0.9]). Additionally, meeting PA + ST + SL guidelines was significantly linked to lower odds of arguments (OR=0.5, 99.5 % CI [0.3–0.9]). Meeting at least one of 24-HMB guidelines was also significantly linked to lower odds of experiencing difficulties in making friends (OR=0.33, 99.5 % CI [0.5–0.7]). As shown in Fig. 2, compared to meeting none of 24-HMB guidelines, meeting independent (ST: OR=0.5, 99.5 % CI [0.3–0.8]) and integrated guidelines (PA + ST : OR=0.2, 99.5 % CI [0–0.5]; PA + SL: OR=0.3, 99.5 % CI [0.2–0.6]; ST + SL :OR=0.5, 99.5 % CI [0.3–0.7]; PA + ST + SL: OR=0.2, 99.5 % CI [0.1–0.4]) were significantly linked to lower odds of difficulties in making friends. Finally, meeting 24-HMB guidelines was significantly linked to lower odds of care difficulty (OR=0.8, 99.5 % CI: [0.7–0.9]). As compared to meet none of 24-HMB guidelines, meeting integrated guidelines (ST + SL: OR=0.3, 99.5 % CI [0.4–1.0]; PA + ST + SL: OR=0.5, 99.5 % CI [0.3–1.0]) were significantly linked to lower odds of care difficulty.
Results presented in Fig. 2 correspond to unadjusted odds rations. Adjustment for covariates did not change the pattern of the relationships. Adjusted odds ratios provided as Supplementary Online Material (Tables A2 and A3).
DiscussionFindings from this large-scale cross-sectional study indicated that the prevalence of children and adolescents with prescribed eyeglasses/contact lenses who meet PA + ST + SL guidelines was relatively low (7.1 %), which is similar to our previous study (6.1 %) on the same age group with visual impairment (Hou et al., 2023). Notably, meeting PA guideline alone appears to be particularly challenging for those with prescribed eyeglasses/contact lenses or with visual impairment (Haegele & Porretta, 2015), which may be partially attributed to the fear of injury that are linked to reduced opportunities for PA engagement (Stuart et al., 2006). Further, meeting independent and integrated components of 24-HMB guidelines were selectively linked to aspects of internalizing and externalizing problems. Main findings will be discussed below, while results for covariates are presented within the Supplementary Online Material.
Association between meeting 24-HMB guidelines and internalizing problemsIn general, internalizing problems encompass experiences of depression and anxiety (Wilkinson, 2009). Meeting 24-HMB guidelines with both categorical (SL + ST and PA + ST + SL)and continuous metrics were beneficially linked to reduced depression and anxiety of those prescribed eyeglasses/contact lenses. Such findings are supported by previous studies on different age groups (e.g., preschoolers, youths, and college students, workers) (Kitano et al., 2020; Ohta et al., 2023; Sampasa-Kanyinga et al., 2021; Zhu et al., 2023) with different health status (e.g., visual impairment and neurodevelopmental disorders) (Brown et al., 2021; Hou et al., 2023). For instance, a cross-sectional study indicated that meeting any combination of 24-HMB guidelines was linked to a lower risk of internalizing behaviors among 11,875 youths. Closer examination of health status, another study on children and adolescents with visual impairment indicated that meeting an integrated (ST + SL) guidelines was linked to reduced levels of depression and anxiety (Hou et al., 2023).
The above-presented findings may be partly attributed to negative social comparisons made on social networking sites which may lead to higher levels of depression and anxiety (Seabrook et al., 2016), which could be exacerbated by prolonged screen-based sitting (Teychenne et al., 2015). In addition, higher ST was linked to internalizing behaviors including depression and anxiety, in turn, may potentially result in Sleep problems (Demirci et al., 2015; Yang et al., 2020). On the other hand, persons who experience high levels of depression and anxiety may be more inclined to utilize devices as a way to “switch off”, which could delay Sleep onset latency and even cause Sleep disorder (Teychenne et al., 2011) - it becomes a vicious cycle. Notably the role of engaging in PA on brain health (e.g., depression and anxiety) has been well-documented (Zou et al., 2023). For instance, a seminal review indicated that PA or exercise effectively alleviated depressive levels through different levels of biological mechanisms (e.g., neurotrophins, cellular signaling pathway, or structural level) (Kandola et al., 2019). Moreover, the benefits of PA could manifest at the psychosocial mechanisms level, social support/positive peer influences positive self-perception (self-esteem or self-efficacy), or resilience may potentially protect against the progression of depressive symptoms (Iannotti et al., 2009; Kandola et al., 2019; Zhang et al., 2022). Collectively, meeting integrated guidelines could maximize the psychological benefits.
Association between meeting 24-HMB guidelines and externalizing problemsExternalizing problems among children and adolescents typically manifest as persistent behavioral problems, and irritability and noncompliance (Tarver et al., 2021) are identified risk factors for social exclusion (Caspi et al., 2014; Sharp, 2002), particularly among persons with visual problems (Beteinaki, 2019). The results of this study indicated that meeting at least two components of 24-HMB guidelines was beneficially linked to arguments, defiant behaviors, care difficulty, and/or difficulties in making friends within the framework of externalizing behaviors. Such findings are supported by previous studies on healthy and clinical participants (e.g., visual impairment, autism spectrum disorder, and attention deficit hyperactivity disorder) across various age groups (e.g., preschooler and youth) (Carson et al., 2019; Hou et al., 2023; Kong et al., 2023; Sampasa-Kanyinga et al., 2021; Taylor et al., 2023). For instance, a youth study indicated that meeting at least 2 guidelines showed stronger and more beneficial association with externalizing behaviors than meeting one or none guideline (Sampasa-Kanyinga et al., 2021). Closer examination of health status, another study on children/adolescent with visual impairment indicated meeting integrated (PA + ST and PA + SL) guidelines were linked to lower odds of social difficulty (Hou et al., 2023).
The above-presented findings may be partially explained by the social learning theory (Bandura & Walters, 1977). Specifically, youth who spent a great amount of time on screen-based activities are more likely to be exposed to inappropriate content (e.g., aggression and violence) (Funk et al., 2004; Tomopoulos et al., 2007). Such long-term engagement may result in desensitization and subsequent maladjustment behaviors (Funk et al., 2004; Huesmann, 2007), and have a negative impact on social functioning in children and adolescents (Domingues‐Montanari, 2017), which potentially limited opportunities for interaction with peers. Additionally, increased time spent on screen-based activities may reduce time spent on other movement behaviors (e.g., SL duration and/or PA) accordingly. As a result, insufficient SL duration could disrupt functions of reward-related brain areas (e.g., decreased response to reward in the striatum and increased response in the dorsomedial prefrontal cortex) or compromise alertness and neurobehavioral functioning, which is closely linked to increased vulnerability for developing externalizing problems (Yue et al., 2022). Furthermore, reduced time in PA engagement or exclusion of PA engagement was linked to frustration, resulting in higher levels of acting out behaviors (Kjønniksen et al., 2009). Conversely, previous meta-analytical studies indicated that the PA intervention programs (e.g., physical exercise, PA and mind-body interventions, and martial arts) effectively improved externalizing behaviors (e.g., aggression, delinquency, hostility, anger, and other maladaptive or disruptive behaviors) in both minors (children and adolescents) and adults (Harwood et al., 2017; Spruit et al., 2016; van der Sluys et al., 2022). Thus, meeting at least two components of 24-HMB guidelines could optimize its associations with externalizing behaviors among our target population.
LimitationsWhile this large-scale study has yielded valuable new insights into associations of meeting 24-HMB guidelines (especially integrated guidelines) with internalizing and externalizing problems among children and adolescents those prescribed eyeglasses/contact lenses, some limitations need to be acknowledged. First, results from this cross-sectional study cannot imply causation. Thus, more longitudinal studies should be conducted to further explore the above-presented relationships so that more nuanced and evidence-based recommendation can be provided for health professionals and policy makers. Second, the use of caregiver proxy-reports during the NSCH survey to assess outcomes of interest (internalizing and externalizing behaviors) might have recall bias and social desirability bias, which is usually linked to an overestimation or underestimation of specific measures (e.g., PA, ST or SL levels) by the parent(s) or legal guardian (Rescorla et al., 2013). Third, the measure of depression and anxiety as indicators of internalizing behaviors are crude and are therefore a limitation of the study. Thus, use of scales and reliable/valid measures should be used in future studies. Fourth, the single-item questionnaire in this study to assess ST cannot identify type of screen-based activities as cognitively active and cognitively passive activities are differentially linked to specific aspects (e.g., depression and anxiety) of brain health (Hallgren et al., 2020). Further, dose-response relationships existed across different type of screen-based activities, for instance, moderate duration of playing video games was linked to better high-order cognition (e.g., executive function) that play a significant role in emotional regulation, social function, and behavioral problems (West et al., 2017). Collectively, more specific measures for screen type in combination with digital device-based approaches should be considered in future studies.
ConclusionsThe current study highlights that a considerable portion of children and adolescents prescribed eyeglasses/contact lenses did not meet 24-HMB guidelines. Moreover, within our sample, the proportion of individuals meeting PA guideline alone (2.5 %) was notably lower compared to those meeting SL guideline alone (32.1 %) and ST guideline (10.9 %) separately. Furthermore, findings indicated associations of meeting integrated guidelines with more favorable outcomes among our target group. This underscores the urgent necessity to customize PA courses at school and home for youth with prescribed eyeglass/contact lenses so that they are more likely to engage in indoor and outdoor activities and in turn lead to increased level of PA. In addition, approaches to limit screen time and ensure sleep duration should be considered, for example, parents should not allow youth to take electronic devices into their bedrooms while cellphone is prohibited at school. Especially, screen time before bed potentially disrupt the sleep-wake cycle, which in turn resulted in poor sleep quality and insufficient sleep. Of note, further longitudinal studies are essential to further validate these associations presented above.
Funding statementThis study (MJ and LYZ) was supported by Shenzhen Education Science Foundation for the 14th Five-Year Plan(zdzb22014), the Ministry of Education for Social Science Foundation (23YJA880093), Shenzhen Science and Technology Innovation Commission (202307313000096), and China Postdoctoral Science Foundation (2022M711174).. MT is supported by a National Health and Medical Research Council Emerging Leadership Fellowship (APP1195335). AOW is supported by the São Paulo Research Foundation (FAPESP) with a PhD scholarship (FAPESP process: 2019/24124-7). The contents of the published material are solely the responsibility of the individual authors and do not reflect the views of the funding bodies.
