



Background/Objective: To examine the roles of anxiety sensitivity and attentional bias in the development of anxiety and depression symptoms among adolescents. Method: 214 grade 7 to grade 10 Hong Kong Chinese students completed a package of psychometric inventories to measure levels of anxiety sensitivity, selective attentional processing, and anxiety and depressive symptoms in 2016 and then again in 2017. Results: Girls, when compared with boys, exhibited more anxiety symptoms and anxiety sensitivity in 2016. They also reported a significant increase in mean depression level from 2016 to 2017. Regression analyses revealed that the physical-concerns dimension of anxiety sensitivity, positive attentional bias, and to a lesser extent negative attentional bias were related to the development of both anxiety and depression symptoms one year later. Fear of mental incapacity could predict depression one year later but not anxiety symptoms. Conclusions: Intervention through anxiety sensitivity training to reduce somatic concerns and attentional bias modification to increase habitual attention to positive stimuli and to disengage from negative stimuli can reduce anxiety and depression symptoms among high school students.
Antecedentes/Objetivo: Examinar el rol de la sensibilidad a la ansiedad y del sesgo atencional en el desarrollo de los síntomas ansiosos y depresivos en adolescentes. Método: Doscientos quatorce estudiantes que cursaban entre séptimo y décimo Grado completaron pruebas para medir niveles de sensibilidad a la ansiedad, procesamiento selectivo atencional y síntomas de ansiedad y depresivos en 2016 y 2017. Resultados: Las chicas mostraron más síntomas de ansiedad y de sensibilidad a la ansiedad en 2016, en comparación con los chicos, así como un aumento significativo en el nivel promedio de depresión entre 2016 y 2017. Los análisis de regresión revelaron que la dimensión relacionada con las preocupaciones físicas de la sensibilidad a la ansiedad, el sesgo atencional positivo y, en menor medida, el sesgo atencional negativo se asociaban al desarrollo de síntomas ansiosos y depresivos después de un año. El temor a la incapacidad mental predecía la depresión después de un año, pero no los síntomas de ansiedad. Conclusiones: El entrenamiento de la sensibilidad a la ansiedad para reducir problemas somáticos y la modificación del sesgo atencional para aumentar la atención habitual a estímulos positivos y desasirse de los negativos puede reducir la ansiedad y síntomas depresivos en estudiantes de Secundaria.
Anxiety and depression are common mental health issues across the globe. In a systematic review of 87 prevalence studies of anxiety disorders from 44 countries published between 1980 and 2009, Baxter, Scott, Vos, and Whiteford (2013) reported that the global prevalence of any anxiety disorders was 7.3% (95% CI: 4.8–10.9%), ranging from 0.9% in China to 28.3% in Afghanistan. In particular, depression escalated from 0.1% below the age of 12 to 4% between the ages of 12 and 17 years (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015). Understanding the factors related to later development of both anxiety and depression symptoms is necessary to enable early interventions to alleviate these problems. This prospective study investigates two cognitive factors, anxiety sensitivity and attentional bias, in the development of both anxiety and depression symptoms one year later. A review of the literature on both anxiety sensitivity and attentional bias and anxiety sensitivity is provided first.
Attentional bias is the generalized habitual cognitive processing style to selectively attend to either negative or positive information (Noguchi, Gohm, & Dalsky, 2006). Generally, methods to research attentional bias fall into two categories: experimental paradigms and psychometric inventories. Regarding psychometric inventories, which are more relevant to this study, the Attention to Positive and Negative Information Scale (APNIS) developed by Noguchi et al. (2006) is most commonly used. It consists of two dimensions: the Attention to Positive Information (API) and the Attention to Negative Information (ANI) scales. They are differentially related to affect: API is related to positive affect, ANI to negative affect (Noguchi et al., 2006). Self-report of attentional bias has been demonstrated to be related to many psychological outcomes among adolescents (Yeung, Ho, & Mak, 2015) and other populations such as cancer survivors (Garland et al., 2016).
Anxiety sensitivity (AS) is the extent to which fear of anxiety-related sensation is interpreted as having negative physiological, psychological, and social consequences (S. Taylor, 1995). Evidence has shown that AS is best constructed as having one higher-order factor (anxiety sensitivity) and three lower-order factors, including physical concerns (fear toward somatic symptoms), mental concerns (fears of mental incapacity), and social concerns (fear of social evaluation) (Brown et al., 2014). AS is a long-established cognitive vulnerability factor for anxiety symptoms (S. Taylor, 1995). Prospective studies of adolescents indicated that AS predicted future occurrence of anxiety symptoms (Hayward, Killen, Kraemer, & Taylor, 2000). Regarding depression, Weems, Hammond-Laurence, Silverman, and Ferguson (1997) provided preliminary evidence for the positive relation between AS and depression in a sample of clinic-referred children and adolescents aged 6–17 years, and the correlation remained significant even after controlling for levels of manifest anxiety (i. e. physiological anxiety, worry, and concentration). Empirical work has provided further evidence that the lower-order AS dimensions are differentially related to certain anxiety and depression disorders (Naragon-Gainey, 2010).
AS has been conceived as a form of attentional bias because individuals high in AS selectively attend to or focus on anxiety-related sensations, which are interpreted as having negative consequences. Schoth, Golding, Johnson, and Liossi (2016) used a pictorial visual-dot probe task, featuring pain-related, health-threat, and general-threat images, to measure attentional bias. Regression analyses revealed that AS and attentional bias showed similar associations toward pain-related images. These results suggest that in children and adolescents, AS is at least associated with attentional bias toward negative information of personal relevance.
Recent theoretical work has tended to examine the relations between cognitive vulnerabilities. However, to date, not many studies have explored the relations among multiple cognitive vulnerabilities and depression and anxiety in adolescents. Building on previous research, in this study we extend this line of investigation by including AS and attentional bias, which are known robust risk factors for anxiety and depression, and examining independent and universal associations between these cognitive constructs and later anxiety and depressive symptoms. It is hypothesized that early (Time 1) AS and attentional bias are important factors to predict later (Time 2) development of anxiety and depression symptoms in a community sample of high school students.
MethodParticipants and procedureEthics approval was obtained from the Human Subjects Ethics Sub-Committee of the City University of Hong Kong (Reference number: 3-15-201502). In March 2016, a total of 216 grade 7 to grade 10 students with a mean age of 14.02 years (SD = 1.19, range = 12.25-17.71) from a high school in Hong Kong were recruited to complete a package of psychological inventories. These students were again approached to complete the same set of questionnaires in March 2017. A letter outlining the purposes and procedures of the study was sent to parents via the school about 3 weeks before the assessment sessions in both 2016 and 2017. Students with written informed consent from their parents participated in the study in a classroom with a group size of about 20, conducted by research assistants with psychology backgrounds.
MeasuresChinese Version of the Childhood Anxiety Sensitivity Index (CASI; Zhao, Shi, & Zhang, 2013). Derived from the original version (Silverman, Ginsburg, & Goedhart, 1999), the CASI is a self-report questionnaire containing 18 items describing reactions to physical symptoms. For each item, participants indicated either 1 (none), 2 (some), or 3 (a lot) for the extent to which they believed the experience of anxiety would result in negative consequences. Higher scores reflected higher levels of AS. Various factor structures of the CASI have been proposed, among which the model with three factors consisting of Physical concerns (PC, 12 items), Social concerns (SC, 3 items), and Mental concerns (MC, 3 items) is used most frequently (Brown, Meiser-Stedman, Woods, & Lester, 2016). Using the software Amos (Version 23.0) (Arbuckle, 2014), the 2016 data from this study were analyzed by confirmatory factor analysis (CFA) to examine if the first-order CFA model consisting of the three above-mentioned factors could achieve a good fit for the present sample. The fit statistics were satisfactory: GFI = .91, CFI = .89, RMSEA = .06, AGFI = .89. Cronbach's alphas of the three subscales for 2016 and 2017 were calculated as follows: 2016 PC = .81, 2016 MC = .65, 2016 SC = .52; 2017 PC = .84, 2017 MC = .69, 2017 SC = .56. The SC subscale was excluded from this study due to its low internal consistency in both years. The two subscale scores were computed by summing each corresponding item score: PC representing sensitivity toward physical symptoms related to anxiety and MC representing sensitivity toward mental incapacitation related to anxiety.
Chinese Attention to Positive and Negative Information Scale (CAPNIS) (Chan, Ho, Tedeschi, & Leung, 2011). The original 40-item English version of APNIS (Noguchi et al., 2006) measures individual differences in the tendency to attend to, think about, and focus on positive or negative information with respect to self and others, and past and future events. It includes two subscales: Attention to Negative Information (ANI, 18 items) and Attention to Positive Information (API, 22 items), which measure negative attentional bias and positive attentional bias, respectively. The Chinese version of the scale (CAPNIS) used by Chan and colleagues (Chan et al., 2011) was used in this study. Participants were asked to rate to what extent each statement was true of them along a 5-point Likert scale (from 1 = very untrue of me to 5 = very true of me). Cronbach's alphas of the two subscales according to the 2016 and 2017 data were calculated as follows: 2016 ANI = .83 and 2016 API = .87; 2017 ANI = .80 and 2017 API = .83.
Chinese Version of the Revised Child Anxiety and Depression Scale (RCADS). The RCADS (Chorpita, Yim, Moffitt, & Umemoto, 2000) consists of 47 items that assess symptoms of anxiety and depression in children aged 8 to 18. The RCADS can better account for the comorbidity between anxiety and depression than other scales designed to measure either one of the two disorders (Cummings, Caporino, & Kendall, 2014). The Chinese version was obtained from the website of the scale (http://www.childfirst.ucla.edu/Resources.html). Participants were required to answer along a 4-point Likert scale (from 1 = never to 4 = always); a higher score indicated greater severity of symptoms. The RCADS-Depression score was computed by summing the 10 items on the Major Depressive Disorder subscale, whereas the RCADS-Anxiety score was obtained by summing the remaining 37 items, which are all related to anxiety. An RCADS-Total score was computed by summing all items of the scale. Cronbach's alphas of the participants’ RCADS-Depression scores and RCADS-Anxiety scores of the 2016 and 2017 data were as follows: 2016 RCADS-Total = .95, 2016 RCADS-Depression = .84, 2016 RCADS-Anxiety = .94; 2017 RCADS-Total = .95, 2017 RCADS-Depression = .85, 2017 RCADS-Anxiety = .94.
Demographic questionnaire. A demographic questionnaire designed for this study was used to obtain personal information including age, gender, place of birth, ethnicity, and first language.
ResultsAmong the 216 students who had completed the questionnaires in 2016, one grade 7 girl and another grade 9 boy failed to promote to a higher grade in 2017. Thus, they were excluded from the analyses. A total of 214 students were therefore included. There were 117 girls (54.7%) and 97 boys (45.3%), with a mean age of 14.68 years in 2017 (SD = 1.22 years, range = 13–18 years). All participants were Chinese, with a majority (96.3%) reporting Cantonese as their first verbal language. The grade distribution in 2017 was as follows: 75 students (35.0%) from grade 8, 49 (22.9%) from grade 9, 55 (25.7%) from grade 10, and 35 (16.4%) from grade 11. There were no significant differences in gender distribution across grades, χ2(3) = 1.92, p = .59.
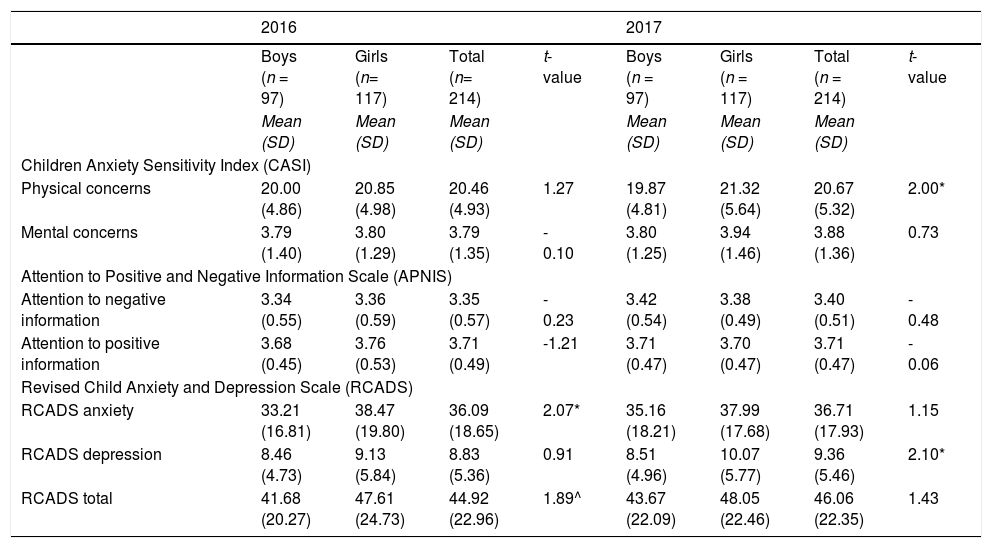
The means and standard deviations of psychological variables are shown in Table 1. Girls, when compared with boys, reported more anxiety symptoms in 2016 (t(212) = 2.07, p < .05, Cohen's d = .29) and more depression symptoms in 2017 (t(212) = 2.10, p < .05, Cohen's d = .29). They also exhibited higher AS toward physical symptoms than boys in 2017 (t(212) = 2.00, p < .05, Cohen's d = .16). No other significant differences were obtained.
Mean and standard deviation of psychological variables by gender and year.
| 2016 | 2017 | |||||||
|---|---|---|---|---|---|---|---|---|
| Boys (n = 97) | Girls (n= 117) | Total (n= 214) | t-value | Boys (n = 97) | Girls (n = 117) | Total (n = 214) | t-value | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||
| Children Anxiety Sensitivity Index (CASI) | ||||||||
| Physical concerns | 20.00 (4.86) | 20.85 (4.98) | 20.46 (4.93) | 1.27 | 19.87 (4.81) | 21.32 (5.64) | 20.67 (5.32) | 2.00* |
| Mental concerns | 3.79 (1.40) | 3.80 (1.29) | 3.79 (1.35) | - 0.10 | 3.80 (1.25) | 3.94 (1.46) | 3.88 (1.36) | 0.73 |
| Attention to Positive and Negative Information Scale (APNIS) | ||||||||
| Attention to negative information | 3.34 (0.55) | 3.36 (0.59) | 3.35 (0.57) | - 0.23 | 3.42 (0.54) | 3.38 (0.49) | 3.40 (0.51) | - 0.48 |
| Attention to positive information | 3.68 (0.45) | 3.76 (0.53) | 3.71 (0.49) | -1.21 | 3.71 (0.47) | 3.70 (0.47) | 3.71 (0.47) | - 0.06 |
| Revised Child Anxiety and Depression Scale (RCADS) | ||||||||
| RCADS anxiety | 33.21 (16.81) | 38.47 (19.80) | 36.09 (18.65) | 2.07* | 35.16 (18.21) | 37.99 (17.68) | 36.71 (17.93) | 1.15 |
| RCADS depression | 8.46 (4.73) | 9.13 (5.84) | 8.83 (5.36) | 0.91 | 8.51 (4.96) | 10.07 (5.77) | 9.36 (5.46) | 2.10* |
| RCADS total | 41.68 (20.27) | 47.61 (24.73) | 44.92 (22.96) | 1.89^ | 43.67 (22.09) | 48.05 (22.46) | 46.06 (22.35) | 1.43 |
* p < .05, ^ p = .06
Paired-sample t-tests were conducted to compare the scores of the psychological variables between 2016 and 2017. Separate analyses were conducted for girls and boys, owing to the significant gender differences in the RCADS scores. Only one significant result was obtained: girls reported a significant increase in the RCADS-Depression score from 2016 to 2017 (t(116) = -2.35, p < .05, Cohen's d = .22). No other significant differences were obtained.
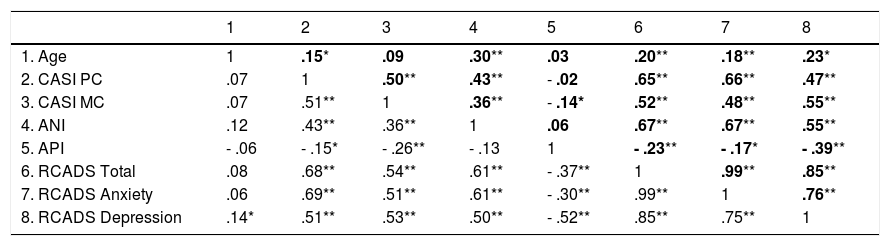
CorrelationsPartial correlation analyses were conducted for 2016 and 2017 separately, with gender controlled as a covariate. The results are shown in Table 2.
Partial correlation with gender as a covariate (N = 214).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Age | 1 | .15* | .09 | .30** | .03 | .20** | .18** | .23* |
| 2. CASI PC | .07 | 1 | .50** | .43** | - .02 | .65** | .66** | .47** |
| 3. CASI MC | .07 | .51** | 1 | .36** | - .14* | .52** | .48** | .55** |
| 4. ANI | .12 | .43** | .36** | 1 | .06 | .67** | .67** | .55** |
| 5. API | - .06 | - .15* | - .26** | - .13 | 1 | - .23** | - .17* | - .39** |
| 6. RCADS Total | .08 | .68** | .54** | .61** | - .37** | 1 | .99** | .85** |
| 7. RCADS Anxiety | .06 | .69** | .51** | .61** | - .30** | .99** | 1 | .76** |
| 8. RCADS Depression | .14* | .51** | .53** | .50** | - .52** | .85** | .75** | 1 |
** p < .01, * p < .05.
Notes. Results 2016 are shown in the upper right hand corner in bold and results for 2017 are shown in the lower left hand corner. Gender (0 = female and 1 = male) is statistically controlled as a covariate. Age = concurrent age, CASI PC = Children Anxiety Sensitivity Index Physical Concerns; CASI MC = Children Anxiety Sensitivity Index Mental Concerns; ANI = Attention to Negative Information; API = Attention to Positive Information; RCADS Total = Revised Child Anxiety and Depression Scale Total Score; RCADS Anxiety = Revised Child Anxiety and Depression Scale Anxiety Score; RCADS Depression = Revised Child Anxiety and Depression Scale Depression Score.
In 2016, age was positively correlated with both anxiety (r2 = .03, p < .01) and depression (r2 = .05, p < .05) scores, but in 2017, it was moderately correlated with depression score only (r2 = .01, p < .05). All other psychological variables were related in the expected directions. Generally, higher AS toward physical concerns and mental concerns and higher negative attentional bias were related to greater current anxiety and depression symptoms. Higher positive attentional bias, in contrast, was related to lower psychopathology. It should be noted that the negative attentional bias (ANI) and positive attentional bias (API) scores were not related to each other in either 2016 or 2017, suggesting that higher habitual tendency to attend to negative environmental stimuli did not necessarily imply lower tendency to attend to positive stimuli, and vice versa.
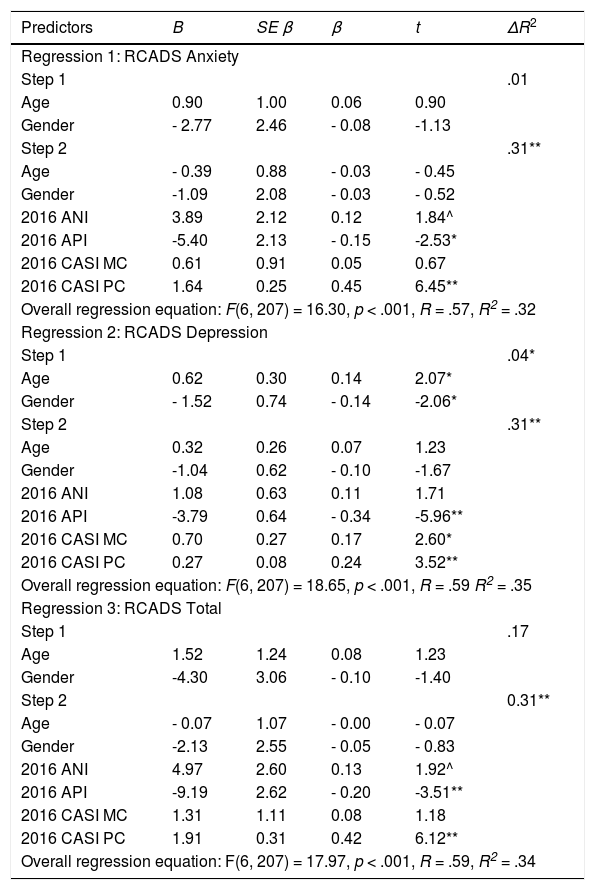
Regression analysisFollowing the strategies of Brown et al. (2016), three independent hierarchical multiple regression analyses were conducted with the 2017 RCADS-Anxiety (Regression 1), 2017 RCADS-Depression (Regression 2), and 2017 RCADS-Total scores as outcome measures (Regression 3). In all of the regression equations, current age and gender were entered in step 1, while prior year (2016) attentional bias (APN and API) and AS (CASI PC and CASI MC) scores were entered in step 2. It should be noted that the 2016 RCADS-Anxiety, RCADS-Depression, and RCADS-Total scores were not included in the regression equations. The variance inflation factors (VIFs) of the RCADS scores in their respective regression equations were all above 2.5 and were much higher than those of other variables, and so were excluded due to multi-collinearity issues. The results are shown in Table 3.
Regression 1: Multiple regression analyses with 2017 RCADS scores as a dependent variable.
| Predictors | B | SE β | β | t | ΔR2 |
|---|---|---|---|---|---|
| Regression 1: RCADS Anxiety | |||||
| Step 1 | .01 | ||||
| Age | 0.90 | 1.00 | 0.06 | 0.90 | |
| Gender | - 2.77 | 2.46 | - 0.08 | -1.13 | |
| Step 2 | .31** | ||||
| Age | - 0.39 | 0.88 | - 0.03 | - 0.45 | |
| Gender | -1.09 | 2.08 | - 0.03 | - 0.52 | |
| 2016 ANI | 3.89 | 2.12 | 0.12 | 1.84^ | |
| 2016 API | -5.40 | 2.13 | - 0.15 | -2.53* | |
| 2016 CASI MC | 0.61 | 0.91 | 0.05 | 0.67 | |
| 2016 CASI PC | 1.64 | 0.25 | 0.45 | 6.45** | |
| Overall regression equation: F(6, 207) = 16.30, p < .001, R = .57, R2 = .32 | |||||
| Regression 2: RCADS Depression | |||||
| Step 1 | .04* | ||||
| Age | 0.62 | 0.30 | 0.14 | 2.07* | |
| Gender | - 1.52 | 0.74 | - 0.14 | -2.06* | |
| Step 2 | .31** | ||||
| Age | 0.32 | 0.26 | 0.07 | 1.23 | |
| Gender | -1.04 | 0.62 | - 0.10 | -1.67 | |
| 2016 ANI | 1.08 | 0.63 | 0.11 | 1.71 | |
| 2016 API | -3.79 | 0.64 | - 0.34 | -5.96** | |
| 2016 CASI MC | 0.70 | 0.27 | 0.17 | 2.60* | |
| 2016 CASI PC | 0.27 | 0.08 | 0.24 | 3.52** | |
| Overall regression equation: F(6, 207) = 18.65, p < .001, R = .59 R2 = .35 | |||||
| Regression 3: RCADS Total | |||||
| Step 1 | .17 | ||||
| Age | 1.52 | 1.24 | 0.08 | 1.23 | |
| Gender | -4.30 | 3.06 | - 0.10 | -1.40 | |
| Step 2 | 0.31** | ||||
| Age | - 0.07 | 1.07 | - 0.00 | - 0.07 | |
| Gender | -2.13 | 2.55 | - 0.05 | - 0.83 | |
| 2016 ANI | 4.97 | 2.60 | 0.13 | 1.92^ | |
| 2016 API | -9.19 | 2.62 | - 0.20 | -3.51** | |
| 2016 CASI MC | 1.31 | 1.11 | 0.08 | 1.18 | |
| 2016 CASI PC | 1.91 | 0.31 | 0.42 | 6.12** | |
| Overall regression equation: F(6, 207) = 17.97, p < .001, R = .59, R2 = .34 | |||||
** p < .01, * p < .05, ^ p < .06.
Note. CASI PC = Children Anxiety Sensitivity Index Physical Concerns; CASI MC = Children Anxiety Sensitivity Index Mental Concerns; ANI = Attention to Negative Information; API = Attention to Positive Information; RCADS Anxiety = Revised Child Anxiety and Depression Scale Anxiety Score; RCADS Depression = Revised Child Anxiety and Depression Scale Depression Score.
For anxiety symptoms, both age and gender were unable to predict current levels of anxiety. AS toward physical symptoms (β = .45, p < .001) and attention to positive information (β = -0.15, p < .05) were significant individual predictors. Greater physical concerns and less positive attentional style were related to higher anxiety levels. The effect of negative attentional bias was marginally non-significant (β = 0.12, p < .06) when the effect of other variables was taken into consideration.
A slightly different picture emerged when RCADS-Depression was the dependent variable. API (β = -0.34, p < .001), CASI PC (β = 0.24, p < .001), and CASI MC (β = 0.17, p < .05) were significant individual predictors in the final equation. Attention to negative information was again not a significant predictor in the final regression equation (β = 0.17, ns).
Regression 3 used the RCADS-Total score as the dependent variable. This allowed examination of the relative importance of each predictor when both depression and anxiety symptoms were taken into account. As expected, both prior year AS toward physical symptoms (β = 0.42, p < .01) and positive attentional bias (β = -0.20, p < .01) were significant individual predictors. Prior year negative attentional bias was marginally non-significant in predicting current year psychopathology (β = 0.13, p < .06).
DiscussionThe major aim of this study is to investigate whether prospective AS and attentional bias account for later anxiety and depression symptoms in a school-based sample of adolescents in Hong Kong. Our results show that the physical-concerns dimension of AS, positive attentional bias, and to a lesser extent negative attentional bias are related to the development of both anxiety (Table 3, Regression 1) and depression (Table 3, Regression 2) symptoms one year later. As expected, they remained as significant predictors when both anxiety and depression symptoms were taken into account (Table 3, Regression 3). Providing partial support to the specific hypothesis that the lower-order AS dimensions are differentially related to anxiety and depression disorders (Naragon-Gainey, 2010), it was found that mental concerns were related only to future depressive symptoms in this study (re Table 3, Regression 2).
Our results are in accord with a previous prospective study among healthy adolescents finding that AS could predict future occurrence of anxiety symptoms (Hayward et al., 2000). Regarding the lower-order AS dimensions, physical concerns are associated with both prospective anxiety and depression symptoms. This result is contradictory to the specific hypothesis, and to the findings of other studies showing that physical concerns are uniquely related to anxiety but not depression (Allan et al., 2015). In support of this result, however, Grant, Beck, and Davila (2007) conducted a longitudinal study among 94 undergraduate students and also reported that physical concerns predicted both anxiety and depression symptoms one year later. The researchers suggested that physical concerns predict depression symptoms because of the high comorbidity of anxiety and depression, i.e. those exhibiting an increase in anxiety symptoms tend to report an increase in depressive symptoms. The same mechanism may apply to our present findings. Supporting the hypothesis that the lower-order dimensions of AS have distinct effects on anxiety and depression, our results show that mental concerns predict depression symptoms one year later but not anxiety symptoms. Other studies also obtained similar results (Allan et al., 2015). It is possible that hypersensitivity related to mental incapacity may lead to avoidance behavior and reduce positive reinforcement in the environment.
One of our major findings is that a lack of positive attentional bias plays an even more important role than the presence of negative attentional bias in the development of prospective anxiety and depression symptoms among our sample of adolescents. Previous studies also found that anxious individuals, when compared with non-anxious individuals, tended to display diminished positive attentional bias (i.e. they tended to avoid positive stimuli in their environment) (C. T. Taylor, Bomyea, & Amir, 2010; Yu et al., 2014). A similar result was obtained among children and adolescents (Visu-Petra, Tincas, Cheie, & Benga, 2010). This result suggests that training to enhance positive attentional bias, in addition to training to disengage from negative stimuli, may be an effective strategy to prevent depression and anxiety. Recently, Waters et al. (2015) provided an example of such training. The researchers conducted training to modify attentional bias toward positive stimuli among anxious children, and showed that children in the training group (n = 31), when compared with the waiting-list control group (n = 28), showed a significant decrease in anxiety level. Strategies from positive psychology like gratitude training to increase sensitivity toward positive events, such as gratitude visits, may also be relevant to reduce anxiety and depression in adolescents (Joseph, 2015). Furthermore, a recent study reported that intensive high intensity treatment is more effective than low intensity treatment in reducing anxiety symptoms (Bornas, de la Torre-Luque, Fiol-Veny, & Balle, 2017). Taken together, high intensity positive attentional bias training may be developed to reduce anxiety risk among adolescents. Finally, a gender difference was observed in our sample. Combining the findings of 2016 and 2017, girls tended to score significantly higher than boys on the physical-concerns dimension of AS and anxiety and depression symptoms (see Table 1). Consistent with the literature (Walsh, Stewart, McLaughlin, & Comeau, 2004), girls reported greater fears toward anxiety-related somatic sensations as signs of physical illness. The results also indicated that, concordant with previous epidemiological research, girls and boys were equivalent in degree of mental (or psychological) concerns related to anxiety. Regarding anxiety and depression symptoms, the exposure mediation model suggests that girls, compared with boys, are more prone to considerable exposure to stressful events (Mezulis, Funasaki, Charbonneau, & Hyde, 2010). In addition, the reactivity moderation model suggests that girls are more sensitive to such occurrences of stress and in turn experience anxiety and depressive symptoms and episodes in greater increments than boys (Mezulis et al., 2010).
Our study has several limitations. First, the study relied on adolescents’ self-reporting of emotional symptoms and cognitions. Experimental tasks, such as visual-dot probe tasks, were not used because of the large sample size and repeated-measures design. There is some debate regarding the validity of self-reports of such internal processes. However, APNIS is a validated scale used widely in both Western populations and among the Chinese (Chan et al., 2011; Noguchi et al., 2006; Yeung et al., 2015). We believe that this scale is a valid measure of attentional bias. Secondly, the social concerns factor was excluded from our analysis due to low internal consistency. Nevertheless, adolescence is the phase during which teenagers establish interpersonal relationships. It would be interesting for further studies to investigate if students with heightened social fears are at greater risk of internalizing disorders. Finally, we did not measure participants’ attention toward ambiguous events whose valence was not abundantly clear. It might be worthwhile to develop a scale that includes emotionally neutral events.
In conclusion, this study contributes to our current understanding of adolescent anxiety and depression by highlighting the differential roles of sensitivity towards somatic concern and positive attentional bias in the development of both disorders. The findings support future development of evidence-based anxiety sensitivity training and attentional bias modification program among adolescents.
Funding and acknowledgementsWe would like to express our sincere gratitude to teachers and students of The ELCHK Yuen Long Lutheran Secondary School for their participation in this study. This work was supported by the General Research Fund of the University Grant Committee (Project number: 11606715).
