




Emotional dysregulation (ED) is a dimensional psychological domain, previously operationalized by instruments of the Achenbach System of Empirically Based Assessment (ASEBA) for children and adolescents; however, its cross-cultural and bottom-up characteristics among adult populations are still unknown.
MethodWe examined scores obtained on the Adult Self-Report (ASR) by 9,238 18- to 59-year-olds from 10 societies that differed in social, economic, geographic, and other characteristics. A Latent Class Analysis was performed on the data from each society.
ResultsIn each society, a dysregulated class (DYS) was identified, which was characterized by elevated scores on most ASR syndromes. The mean prevalence of DYS was 9.2% (6.1-12.7%). The best models ranged from three to five latent classes in the different societies.
ConclusionsAlthough the number of identified classes and the prevalence of ED varied across societies, a DYS class was found in each society, suggesting the need to adopt a dimensional view of psychopathology and a cross cultural perspective also in adult populations.
La desregulación emocional (DE) es un ámbito dimensional en Psicología, previamente operacionalizado por los instrumentos del Sistema de Evaluación Basado Empíricamente de Achenbach (ASEBA, por sus siglas en inglés) para niños y adolescentes; sin embargo, aún se desconocen sus características interculturales y su enfoque ascendente en su aplicación a la población adulta.
MétodoExaminamos las puntuaciones obtenidas en el Autoinforme de Adultos (ASR, por sus siglas en inglés) por 9.238 personas de 18 a 59 años de edad pertenecientes a 10 sociedades que diferían en cuanto a sus características sociales, económicas, geográficas y de otro tipo. Se realizó un Análisis de Clases Latentes con los datos de cada sociedad.
ResultadosEn cada sociedad se identificó una clase desregulada (DES), que se caracterizaba por puntuaciones elevadas en la mayoría de los síndromes ASR. La prevalencia media de DES fue del 9,2% (6,1-12,7%). Los mejores modelos oscilaron entre tres y cinco clases latentes en las diferentes sociedades.
ConclusionesAunque el número de clases identificadas y la prevalencia de DE variaron entre las diversas sociedades, se encontró una clase DES en cada sociedad, lo que sugiere la necesidad de adoptar una visión dimensional de la psicopatología y una perspectiva intercultural también en las poblaciones adultas.
Interest has increased in multicultural perspectives on psychopathology. The replicability of psychological categorical and dimensional constructs in different societies has become a relevant research field with significant influences on clinical practice (Ivanova, Achenbach, Rescorla, Tumer, Ahmeti-Pronaj et al., 2015). Hence, several cross-cultural studies, using different instruments and approaches, have been conducted to evaluate the generalizability of psychological profiles in societies with very different social, political, and economic systems as well as languages, ethnicities, religions, and geographical regions (Gardiner et al., 2019; Ivanova, Achenbach, Rescorla, Turner, Árnadóttir et al., 2015; Vindbjerg et al., 2019).
Emotional dysregulation (ED) is a dimensional psychological domain that has received strong scientific attention and, recently, has been investigated in cross-cultural studies (e.g., Rescorla et al., 2020). Emotional self-regulation includes the individual ability to identify and properly interpret environmental emotional stimuli, to recognize individual self-emotions, and to deal with them, generating appropriate social responses (Dumont et al., 2019). Therefore, ED reflects both failure of cognitive control and high intensity of arousal (Soloff et al., 2015). These deficits cause higher sensitivity to emotional arousal, slower return to baseline activation, and deficits in coping strategies.
This transdiagnostic construct is relevant to patients with developmental disorders as well as to adults with psychiatric pathologies (Garofalo et al., 2018; Murray et al., 2021). It may be encountered in adult ADHD patients (Christiansen et al., 2019) and is common in patients with conditions such as bipolar and borderline personality disorders (Garofalo et al., 2018).
Different facets of ED can be evaluated in clinical and general populations. The ASEBA research group (Achenbach, 2009) initially operationalized it with a latent class approach through the Dysregulation Profile (DP), by summing the scores of items comprising the Anxious/Depressed (ANXD), Attention Problems (ATT), and Aggressive Behavior (AGG) syndromes of the Child Behavior Checklist for Ages 6-18 (CBCL/6-18; Althoff et al., 2010). DP originally was linked only to bipolar disorder (Biederman et al., 1995). Recent studies have demonstrated that it is associated with multiple categorical psychiatric diagnoses from childhood to adulthood, with an increased risk of problems in affect, behavior, and cognition (Aitken et al., 2019; Althoff et al., 2010; De Caluwé et al., 2013; Deutz et al., 2018; Holtmann et al., 2011).
Several studies have also demonstrated that the DP, rather than being a predictor of a specific disorder, is a marker for persistent psychopathology and significant impairment, as well as personality pathology, suicidality, and substance use (Rescorla et al., 2020). A longitudinal 4-year follow-up study showed that ADHD is associated with ED in children with a higher number of psychiatric comorbidities, greater social impairment, and persistence of ADHD, if compared with ADHD without ED or healthy controls (Biederman et al., 2012).
Nowadays, DP is now viewed as including both internalizing and externalizing psychopathology areas. Rescorla and colleagues (2018) reported international comparisons of DP (calculated by summing ratings of the items on the ANXD, ATT, and AGG) on the CBCL/6-18, Teacher's Report Form (TFR), and Youth Self Report (YSR) in 42, 34, and 27 societies, respectively. The authors found that participants in many societies reported similar DP scores, despite cultural differences between societies.
ED has also been studied with bottom-up methods. Rather than pre-selecting specific items or subscales, bottom-up methods involve identifying profiles via person-centered statistical approaches. Among these, latent class analysis (LCA) is one of the most common. LCA is a finite mixture model in which each participant is assigned to a specific class depending on how they respond to items or scales of a questionnaire (McCutcheon, 1987). Each class has a specific profile of responses (Goodman, 1974). LCA provides models based on the sample data, to find the solution that maximizes the difference between the identified classes and minimizes the heterogeneity within each class (Jung & Wickrama 2008). Several studies using LCA have identified a dysregulated class (DYS) among infants, children, and adolescents from different countries (Basten et al., 2013; Bianchi et al., 2017; Connell et al., 2008; De Caluwè et al., 2013).
In two studies, LCA was used to investigate the presence of a DP in multiple societies. Jordan et al., (2016) used YSR data from 34 societies and Rescorla et al., (2020) used CBCL/6-18 data from 29 societies to identify a DP class in each society, with prevalences ranging from 1% to 26% in the YSR data and from 2% to 18% in the CBCL/6-18 data. In both studies, the DP class comprised participants with higher scores in the ANXD, ATT, and AGG syndrome scales. Not surprisingly, in many societies, the DP class showed elevated scores on all eight syndrome scales. The results thus revealed a remarkably high prevalence of ED, characterized by a wide range of problems in children and adolescents, not limited to the ANXD, ATT, and AGG syndromes included a priori in DP.
Considering the advance of globalization, mental health clinicians need to be aware of patterns of psychopathology found in different societies. Although studies have tested the generalizability of child and adolescent DP across societies, the prevalence and characteristics of DP among adults have not been tested in multiple societies, to our knowledge. (We use “societies” in reference to geopolitically demarcated populations having a dominant language).
The purpose of this study was to test the cross-societal generalizability of ED profiles in adult populations assessed with the Adult Self Report (ASR), a self-report questionnaire for ages 18-59 that assesses behavioral, emotional, and social problems (Achenbach & Rescorla 2003), using LCA as a person-centered statistical approach. LCA is well suited for ASEBA syndromic data from various societies because it enables researchers to test whether similar concurrent elevations in syndrome scales can be detected among members of different populations, without a priori conception and apart from cultural differences.
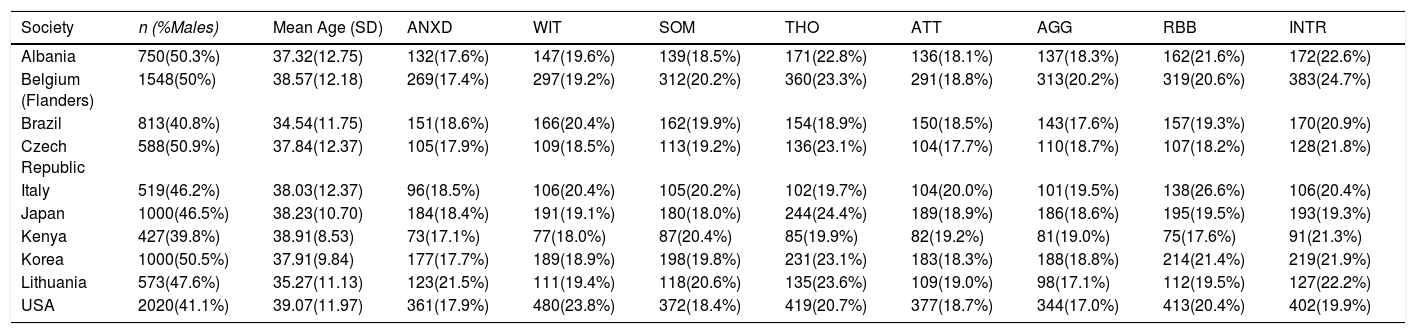
MethodParticipantsASR data were obtained from population samples of ≥400 adults in each of 10 societies, with most being countries. The societies differed with respect to ethnicity, religion, geographical location, socioeconomic and mental health systems, and population size. Specific data on cultural differences and sociodemographic level were not taken into account. Data were analyzed from 9,238 18- to 59-year-olds living in Albania, Belgium (Flanders), Brazil, Czech Republic, Italy, Japan, Kenya, Korea, Lithuania, and USA, as summarized in Table 1. The sample sizes ranged from 427 in Kenya to 2,020 in the USA; the percentage of male subjects ranged from 38.9% in Kenya to 50.9% in the Czech Republic; and the mean age ranged from 34.54 years (SD = 11.75) in Brazil to 39.07 (SD = 11.97) in the USA. Investigators followed local ethical protocols and obtained informed consent from participants. All data were de-identified.
Descriptive statistics and frequencies of syndrome scales T-scores in the clinical range (≥85th percentile) (n, %), for each included society.
Note. AGG = Aggressive Behavior; ANXD = Anxious/Depressed; ATT = Attention Problems; INTR = Intrusive; RBB = Rule-Breaking Behavior; SOM = Somatic Complaint; THO = Thought Problems; WIT = Withdrawn.
The ASR (Achenbach & Rescorla, 2003) has been shown to be a valid transcultural self-report measure of psychopathological problems for ages 18-59 in all the societies included in our study, presenting a homogeneous structure across cultures (Achenbach, 2019; Ivanova, Achenbach, Rescorla, Tumer, Ahmeti-Pronaj et al., 2015).
The ASR obtains self-ratings of 120 items assessing behavioral, emotional, social, and thought problems, based on the preceding 6 months, and scored on eight syndromes derived from factor analysis (Achenbach & Rescorla, 2003). The problem items are rated 0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true. The 0-1-2 ratings are summed to provide scale scores for syndromes designated as Anxious/Depressed, Withdrawn, Somatic Complaints, Thought Problems, Attention Problems, Aggressive Behavior, Rule-Breaking Behavior, and Intrusive.
Achenbach and Rescorla (2003) reported that the test-retest reliability of the ASR syndrome scales in the U.S. national sample ranged from .83 to .91, while Cronbach's internal consistency alphas ranged from .51 to .88 for the eight syndrome scales. The Multicultural Supplement to the Manual for the ASEBA Adult Forms & Profiles (Achenbach & Rescorla, 2015) and the Manual for the ASEBA Adult Forms & Profiles (Achenbach & Rescorla, 2003) report additional psychometric properties.
Researchers from all societies except the USA used translations of the ASR that were validated through independent back-translations and were approved by the authors.
For each of the 10 samples, T-scores (Table 1) were calculated for the eight syndrome scales, separately for each sex at ages 18-35 and 36-59, using the following formula:
50 + [10 * (raw score − mean score) / standard deviation]
The T-scores then were dichotomized to create an additional variable as “not at risk” (< 85th percentile) versus “at risk” (≥ 85th percentile).
ProcedureAfter checking for the model assumptions, we performed a LCA to examine whether specific homogeneous groups of subjects could be identified in each sample. Specifically, LCA was performed on the dichotomized ASR scales (as explained in the Instruments section) in each sample, separately. Models estimating solutions from two classes to N classes were compared. The number of classes was increased until the log-likelihood (LLH) value stopped replicating or until N-class solution fit-indexes were worse than N-1 class solution fit-indexes. The best solution was determined following the LCA procedures used by Althoff et al., (2010): we assessed model fit with the sample size–adjusted Bayesian information criterion (adj-BIC), the Voung–Lo–Mendel–Rubin likelihood ratio test (VLMRT), and the bootstrapped likelihood-ratio test (BLRT). Based on procedures described by Althoff et al., (2010), we took the BLRT as being more definitive than the VLMRT when the two did not agree. Therefore, the model considered as having the best fit should have the lowest adj-BIC and a significant BLRT when compared with the k − 1 class model. In addition, we considered the rule of parsimony, the substantive relevance of a class, and the value of entropy—ranging from 0 to 1, with a value of 1 when all respondents have a probability of 1 of being in one class, and a value of 0 when the probabilities of being assigned to a class are constant for all subjects. We aimed to choose the highest number of classes, such that none of the classes would be too small (e.g., less than 5% of the sample). This rule has long been used in practice as a part of the idea of domain-usefulness but also has been discovered to have theoretical justification (Nasserinejad et al., 2017).
The identified classes were given descriptive labels based on the authors’ consensus after reviewing each class's unique profile. Specifically, the DYS class was identified as the one presenting the highest scores on the ANXD, ATT, and AGG scales, according to the literature (Aitken et al., 2019; Althoff et al., 2010; Holtmann et al., 2011). During the validation phase of the latent classes, each subject was assigned to their highest probability class using the “known classes” algorithm. LCA were performed using Mplus 6.11 (Muthén & Muthén, 1998).
After identifying the best class solution and checking for model assumptions, to detect between-classes statistical differences between each society, we performed ANOVAs using the eight syndrome scales’ T-values as the dependent variables and class assignment as the independent variable. ANOVAs were performed using SPSS (Version 21).
The University of Vermont Committee on Human Research in the Medical Sciences (CHRMS) approved this study. The University of Vermont (UVM) IRB protocol number is 14-237.
ResultsSelection of the LCA modelsFor five of the 10 societies (Brazil, the Czech Republic, Italy, South Korea, and the USA), LCA was tested for models with two to five classes. Regarding the other five, the data model testing for Kenya ended at three classes; in addition, a six-class solution was tested for Albania, Belgium, Japan, and Lithuania. Because multiple indices were considered in selecting the optimal LCA model and those indices did not always agree, some degree of judgment was involved in the selection process.
In eight of the 10 societies (Brazil, the Czech Republic, Italy, Japan, Kenya, Lithuania, South Korea, and the USA), the BLRT and the adj-BIC agreed in identifying the best class solution, and in four of these societies (Czech, Kenya, South Korea, the USA), the indexes also were in line with the VMLR. For the remaining four (Brazil, Italy, Japan, and Lithuania), the BLRT was considered the more definitive test of model fit. For one society (Belgium), the adj-BIC was lower in the model, with one less class than the chosen model, but the entropy and BLRT were better in the latter model. When selecting the final model, in this case, we also considered the rule of parsimony, the frequencies of subjects in each class, and the clinical features of the classes. Regarding the Albanian data, the five-class solution was excluded because it included one class with a percentage of subjects lower than 5%. Concerning entropy, most of our models showed good but not optimal values. Only the entropies for Kenya, Japan, and Italy were adequate (i.e., ≥ .80) and indicated a good separation between classes. For the other societies, the values ranged from .70 for Brazil to .79 for Albania, suggesting that researchers should pay attention when using “most likely class membership” as a variable for further analysis because some of the classes did not seem to be distinguished.
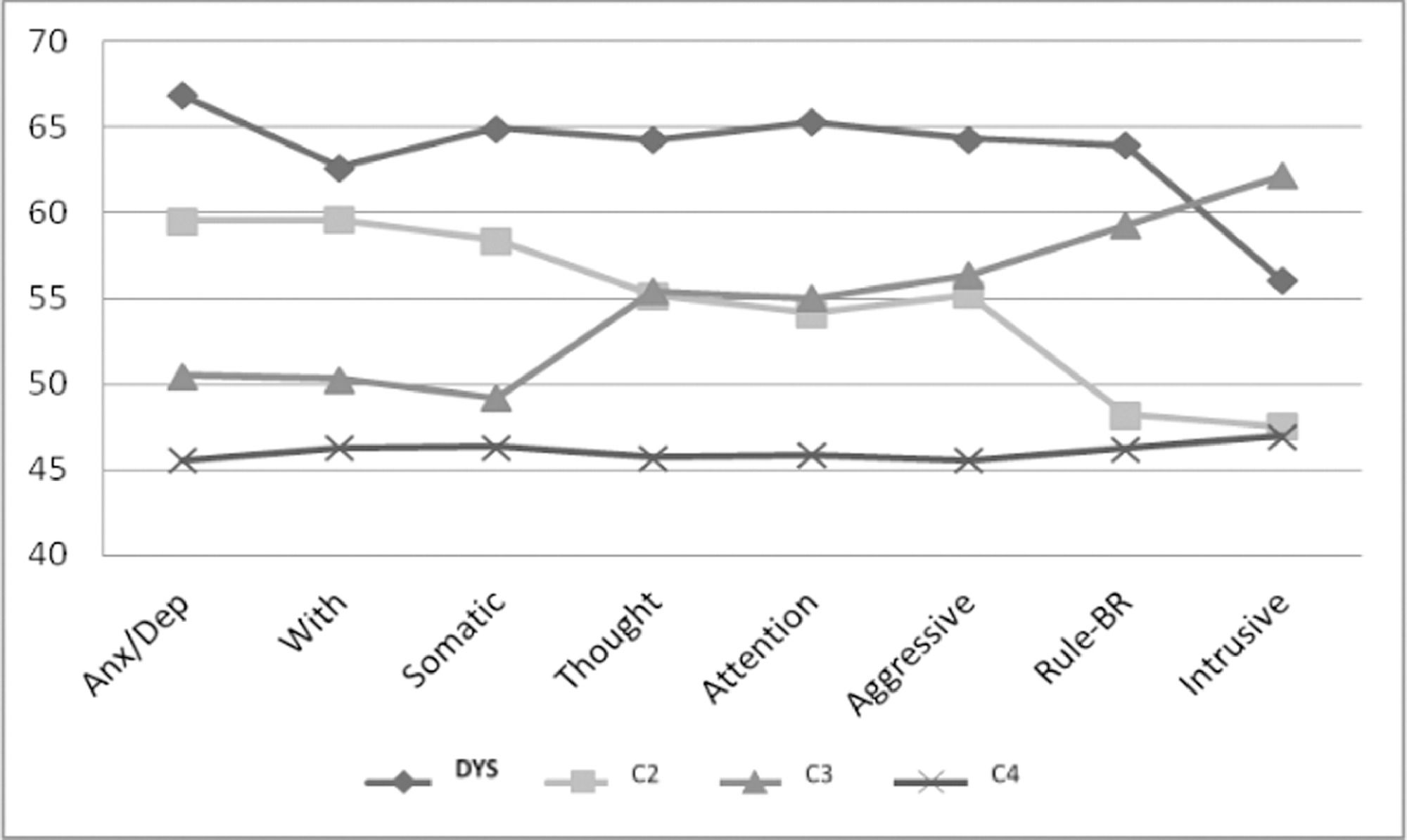
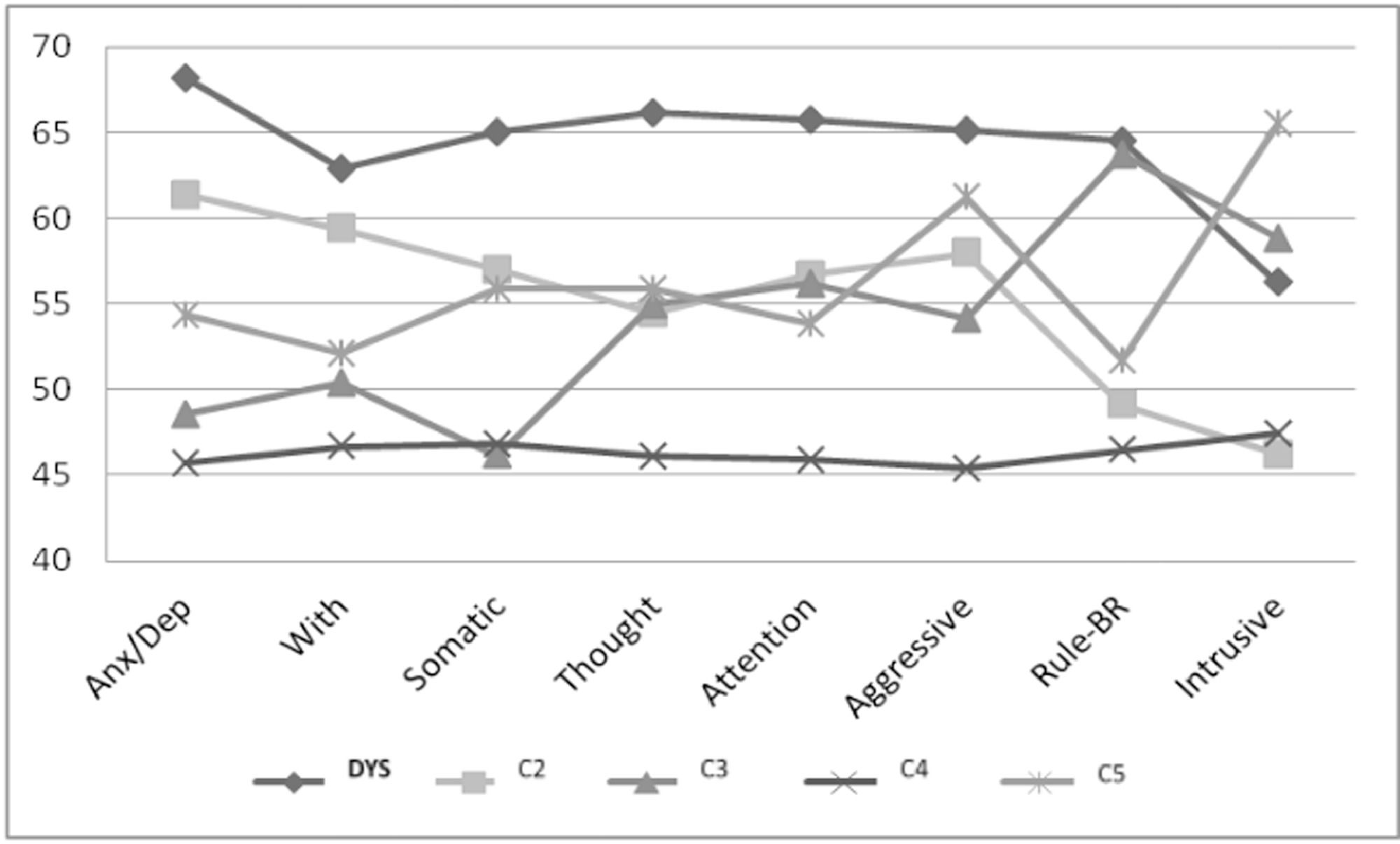
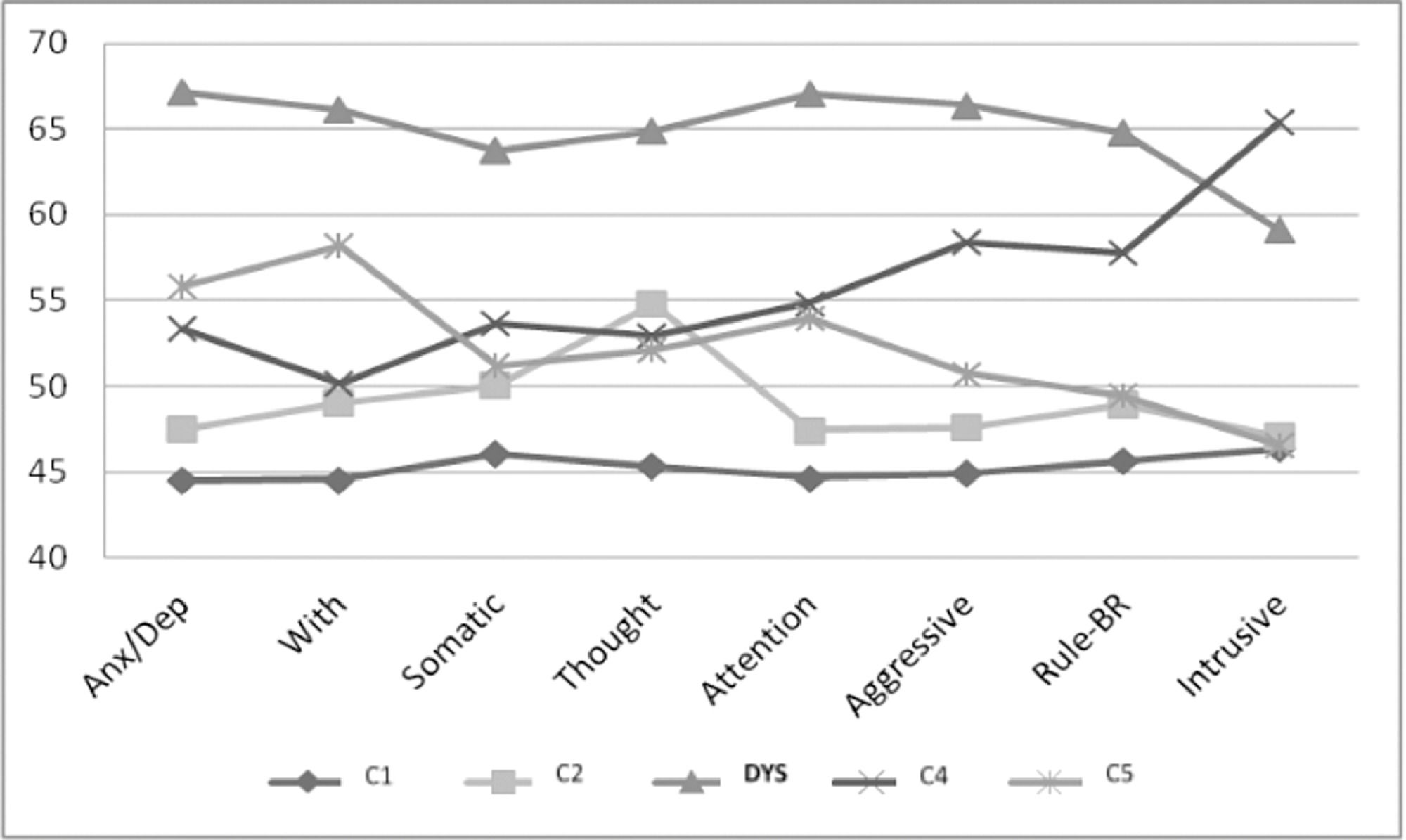
The model selected as best involved five classes in three societies (i.e., Belgium, Japan, and Lithuania), four classes in six societies (i.e., Albania, Brazil, Czech, Italy, South Korea, and the USA), and three classes in one society (i.e., Kenya).
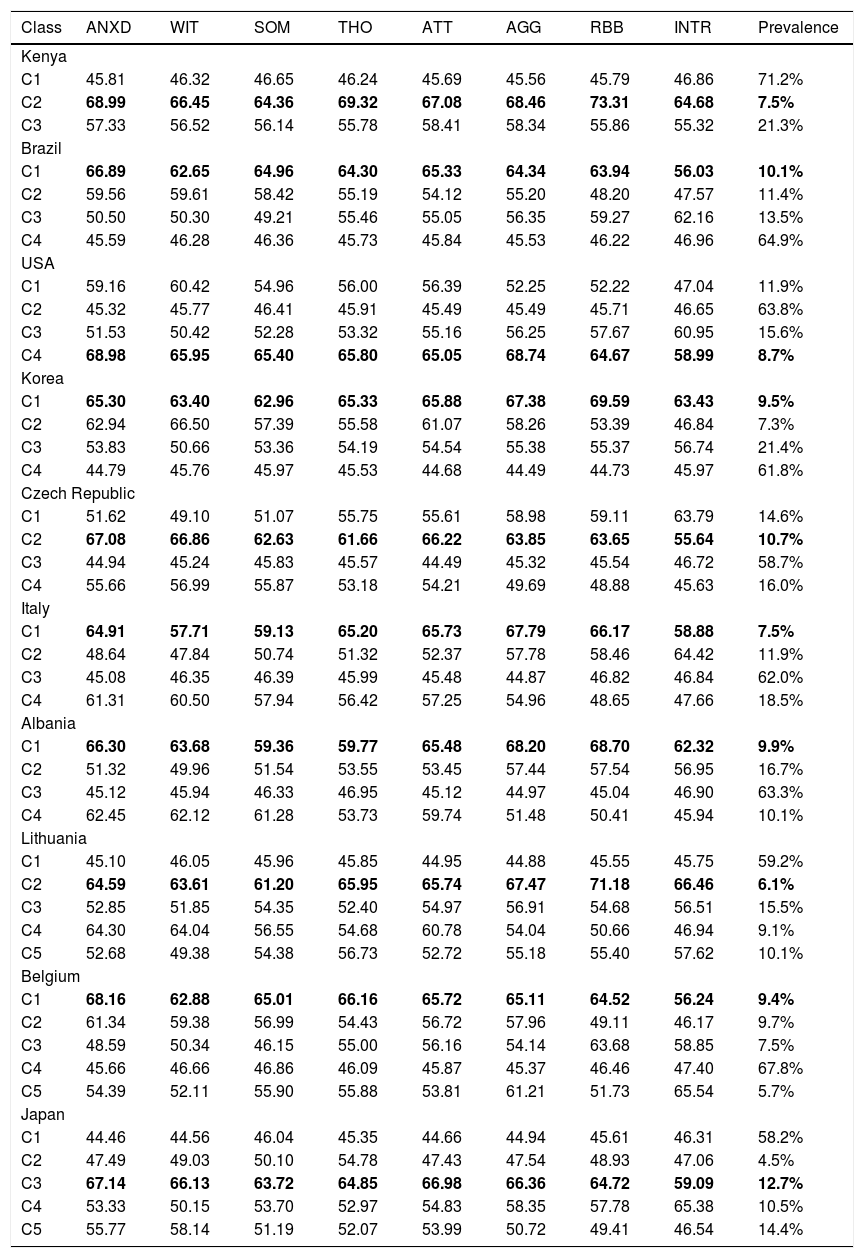
A DYS class was identified in each society. The omnicultural mean prevalence of DYS was 9.2%, ranging from 6.1% (Lithuania) to 12.7% (Japan) (see Table 2).
T-scores means and prevalence for each class in each sample.
Note. AGG = Aggressive Behavior; ANXD = Anxious/Depressed; ATT = Attention Problems; DYS = Severe Dysregulated; INTR = Intrusive; LOW = Low Problems; MILD = Mild Problems; RBB = Rule-Breaking Behavior; SOM = Somatic Complaints; THO = Thought Problems; WIT = Withdrawn.
Class, highlighted in bold, is “DYS-Severe Dysregulated” (including subjects with elevations in ANXD, ATT, and AGG and, more generally, in both externalizing and internalizing ASR areas scales).
The ANOVAs conducted for each society on the eight syndrome scales’ T-values (as dependent variables) and class assignment (as the independent variable) showed that the participants in the DYS class had different scores in all ASR scales, as compared to adults in the other classes (p < .01). Specifically, subjects falling into the DYS class had higher scale scores on ANXD, ATT, and AGG and, more generally, in both internalizing and externalizing areas. This effect was significant for all scales in each society, with few exceptions. Participants in the DYS class and in the INT class had similar scores on the Withdrawn and Somatic Problems scales in Italy and Albania, and on the Withdrawn and Anxious/Depressed scales in Lithuania. In the Belgian sample, Rule-Breaking Behavior scores were similar between the participants in the DYS and EXT classes.
Discussion



We evaluated the presence of ED profiles in samples from 10 societies throughout the world, assessed with the ASR, using LCA as a person-centered, bottom-up approach. To our knowledge, this is the first study focusing on adult general populations, whereas previous studies have focused on children (e.g., Basten et al., 2013; De Caluwè et al., 2013) or adolescents (e.g., Bianchi et al., 2017; Jordan et al., 2016; Rescorla et al., 2020) and on clinical or mixed populations (e.g., Bianchi et al., 2017; Rescorla et al., 2020). In all 10 societies, we found a DYS class that was characterized by elevated T-scores on most syndrome scales. Moreover, despite the DYS class having high scores on the ANXD, ATT, and AGG scales, our findings show that, when using a bottom-up rather than an a-priori approach, a latent class characterized by elevated scores on only the three DP syndromes is less common than classes characterized by elevations on all eight syndromes. This result is consistent with previous findings for children and adolescents (Jordan et al., 2016; Rescorla et al., 2020).
Our sample represented 10 world societies from Europe, North and South America, Eastern Asia, and Eastern Africa having different ethnicities, religions, population sizes, geographic locations, and socioeconomic and geopolitical characteristics. To our knowledge, this study is the first international application of LCA to ED among adults.
The percentage of participants in the DYS class in our study varied from 6.1% (Lithuania) to 12.7% (Japan), with a mean value of 9.2% across all 10 societies. These results were consistent with those of previous studies on child and adolescent samples (Jordan et al., 2016; Rescorla et al., 2018; Rescorla et al., 2020). Specifically, Rescorla et al., (2020) found an omnicultural mean prevalence of the DYS class, using the CBCL, of 9% among 29 societies (Rescorla et al., 2020), while Jordan et al., (2016) found an omnicultural mean prevalence of 9.2% among 34 societies using the YSR.
The similarities between our results for adults and previous results for children and adolescents (Bianchi et al., 2017; Jordan et al., 2016; Rescorla et al., 2020) suggest the persistence of severe dysregulation from childhood to adulthood. Longitudinal studies are needed to test this hypothesis and to disentangle possible homotypic and heterotypic developmental trajectories. Future studies should assess the onset, progress, and changes in the classes over time and to consider biological factors as possible mediators or moderators of environmental risk factors in shaping developmental trajectories (Thapar & Riglin, 2020).
In most societies, members of DYS classes had high scores on more syndrome scales than did members of other classes, suggesting that the DYS classes represent a high level of psychopathology, independent of internalizing and externalizing dimensions. This result opens a question about the specificity of ED. According to previous results, the construct of ED is independent from the presence of a specific diagnosis and has various genetic markers (Christ et al., 2019; Corbisiero et al., 2013; McGough et al., 2008). Other results, as from Althoff et al., (2010), highlighted a heterotypic continuity of ED; nevertheless, its labile border with the concept of psychopathology severity raises the issue of whether this profile is simply a marker of severe psychopathology/high comorbidity rather than a specific phenotype Jordan et al., (2016). also raised the question if members of an LCA-identified class have high scores on most or all of the eight syndromes of the ASEBA questionnaires, should the class be considered to represent the DP, or just severe psychopathology. However, our data did not allow us to disentangle this theoretical differentiation, due to the fact that our sample consists of the general population. Hence, it would be informative to test associations of DYS profiles with specific psychopathological traits and diagnoses to verify the specificity of DYS profile.
Adults in DYS classes did not differ significantly from adults in other classes on some syndrome scales. Specifically, the Anxious/Depressed, Withdrawn, and Somatic Complaints scores of the DYS classes were similar to those of the INT class in Albania, Italy, and Lithuania, while the Rule-Breaking Behavior scores of the DYS classes were similar to those of the EXT class in Belgium. Previous work by our research group (Bianchi et al., 2017) obtained results on a sample of Italian children like our results for the ABCL, suggesting that individuals in the DYS classes retain their DYS characteristics from childhood to adulthood.
Our use of large epidemiological samples is an innovative element of our work. However, future research could apply similar analyses to adult clinical samples in order to test relations between categorical diagnoses and profiles of ED.
Our study has some limitations. Firstly, sociodemographic data were not collected, which represent one of the most important limitations of our study. Future studies could deepen the role of sociodemographic information to disentangle differences in prevalence and characteristics of DYS profile. Furthermore, we did not collect data from multiple informants or sources (e.g., using the Adult Behavior Checklist-ABCL) or information regarding the onset, progress, or changes in the classes over time. Future investigations could add more knowledge about the development and characteristics of dysregulation from different perspectives and could analyze possible cultural differences, which may have some impacts in the expression of DYS profile. The addition of other information and multiple sources could improve the validity and generalizability of the direction of our results. Even though Jordan et al., (2016) already tested the method we used, it is important to highlight that we computed T-scores based on each sample's mean and SD, rather than using norms from each society. Our eight-syndrome T-scores thus showed only “relative” elevations among the classes derived by LCA in each society.
Moreover, in some cases, arbitrary decision rules were needed to determine the optimal number of latent classes because the statistical indices were not always consistent, as was also found in previous studies (Jordan et al., 2016; Nasserinejad et al., 2017; Rescorla et al., 2020).
Finally, the results of the between-class ANOVAs should be viewed with caution, because not all of our models achieved optimal entropy values.
ConclusionsCounterparts of the DYS profile were found in adult population samples from 10 very diverse societies. The prevalence ranged from 6.1% to 12.7%, with an omnicultural mean of 9.2%. Despite major cultural differences across the samples, our findings indicate that clinicians and researchers should be alert to patterns of dysregulation among adults from many backgrounds. ED, independent of possible categorical diagnoses, is linked to poor outcomes (McQuillan et al., 2018; Rescorla et al., 2020). Moreover, the present findings suggest that it is crucial for researchers and clinicians to adopt dimensional and cross-cultural perspectives, given the need for reliable and generalizable constructs and instruments for assessment of diverse populations (Ivanova, Achenbach, Rescorla, Tumer, Ahmeti-Pronaj et al., 2015).
This work was supported by the Italian Ministry of Health (Grant number RC2020-2021-2022 and REMIND Project: REal Matters IN Developmental psychopathology RF-2016-02364582 to MN and AF). The funding source had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
