




Background/Objective: Eating disorders (EDs) represent serious yet understudied mental health issues, particularly amongst young adult men attending colleges, who are at the average age of onset. Despite this and recent evidence that in young adult men the core ED symptoms are prevalent and remain relatively stable over the college period, little is known about factors associated with both the onset and maintenance of diagnosable EDs in this population. This work sought to address these research gaps. Method: Logistic regression analyses were conducted using data from an on-going longitudinal study of eating and mental health issues to examine the influence of theoretically relevant factors in predicting the onset and maintenance of men's (DSM-5) EDs at 4-year follow-up (N=2,507). Results: Body dissatisfaction, self-objectification, appearance-ideal internalization, dieting, and negative affectivity were all predictors of ED onset and maintenance. Self-objectification was the largest contributor to both ED onset and maintenance. Conclusions: The findings highlight potentially similar psychosocial foci for prevention and treatment efforts. Implications for improving existing preventive and treatment approaches are discussed.
Antecedentes/Objetivo: Los trastornos de la conducta alimentaria (TCAs) representan graves, aunque poco estudiados, problemas de salud mental en las universidades, especialmente en hombres jóvenes, quienes se encuentran en la edad media de inicio. A pesar de la evidencia de que en hombres adultos jóvenes los principales síntomas de TCA son frecuentes y se mantienen relativamente estables durante el período universitario, poco se sabe sobre los factores asociados con la aparición y el mantenimiento de los TCAs en esta población. Este trabajo trata de abordar estas lagunas de investigación. Método: Se realizaron análisis de regresión logística utilizando datos de un estudio longitudinal en curso sobre alimentación y salud mental para examinar la influencia de factores teóricamente relevantes para predecir la aparición y el mantenimiento de los TCAs (DSM-5) en hombres durante 4 años de seguimiento (N=2.507). Resultados: La insatisfacción corporal, la auto-objetivación, la internalización de la apariencia ideal, las dietas, y la afectividad negativa fueron predictores de inicio y mantenimiento de TCA. La auto-objetivación fue el mayor contribuyente a la aparición y mantenimiento de TCA. Conclusiones: Los resultados destacan focos similares para su prevención y tratamiento. Se discuten las implicaciones para mejorar los enfoques preventivos y de tratamiento existentes.
Threshold eating disorders (EDs), i.e., anorexia nervosa (AN), bulimia nervosa (BN), and binge eating disorder (BED), but also other specified feeding and EDs (OSFEDs) recognized in DSM-5, i.e., atypical AN, BN and BED of low frequency and/or limited duration, and purging disorder (American Psychiatric Association [APA], 2013), are all marked by chronicity, functional impairment, emotional distress, and physical morbidity (e.g., Allen, Byrne, Oddy, & Crosby, 2013; Raevuori, Keski-Rahkonen, & Hoek, 2014). They represent serious yet understudied mental health issues, particularly amongst young men attending colleges, who are at the average age of onset (Raevuori et al., 2014). For instance, according to recent prospective data from community-recruited male samples (Allen et al., 2013), the peak onset age is 18-20 years for any ED and OSFED. College has been identified as a possible precipitating factor of the initiation and/or deterioration of the component symptoms of EDs, i.e., behavioural features shared across ED/OSFED diagnoses such as binge-eating, laxative/diuretic misuse, fasting, excessive exercise, and self-induced vomiting (e.g., Cain, Epler, Steinley, & Sher, 2012; Dakanalis, Clerici et al., 2016; Dakanalis, Timko et al., 2016). Contemporaneous research with young adult men also showed that the aforementioned component symptoms of EDs are prevalent (Dakanalis, Clerici et al., 2016) but also relatively stable over the four traditional years of college (Cain et al., 2012). Consistently, DSM-5 (APA, 2013), that outlined more sex-neutral diagnostic criteria for threshold EDs and their OSFED variants, provided opportunities for improved recognition and diagnosis of EDs in young adult men (Raevuori et al., 2014). Nonetheless, our knowledge regarding the course and the factors mainly associated with both the onset and maintenance of diagnosable EDs in this population is limited.
The dual-pathway model of eating pathology (e.g., Stice, Marti, & Durant, 2011) has emerged as a key framework for explaining the development and persistence of EDs (Culbert, Racine, & Klump, 2015). It posits that body dissatisfaction, resulting from appearance-ideal internalization (i.e., endorsement of unattainable societal body shape ideals as own ideals and standards for comparison) promotes unhealthy dieting behaviours that may progress to AN (Stice et al., 2011). Further, people may think the restriction of food intake for limited periods allows them to binge eat but not gain weight/body fat “which might promote a cycle of acute restriction punctuated by overeating” (p. 623). Body dissatisfaction is also thought to promote negative affectivity (i.e., shame, anxiety, sadness) because of the importance of physical appearance in western culture, which in turn may trigger binge-eating as a means of coping with aversive feelings. In some individuals binge-eating (i.e., eating unusually large quantities of food accompanied by subjective feelings of loss of control) may be followed by a range of compensatory behaviours (i.e., self-induced vomiting, excessive exercise) aimed at counteracting the effects of calories consumed and avoiding weight/body fat gain, which can “turn into a vicious cycle” (p. 623). Indeed, longitudinal studies with adolescent girls have shown that body dissatisfaction and dieting increase risk for any threshold ED and OSFED, with appearance-ideal internalization and negative affectivity predicting onset of any OSFED and threshold BN and BED (e.g., Culbert et al., 2015; Stice et al., 2011). Furthermore, elevated body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity are all associated with the development and persistence of clinically significant ED pathology amongst initially asymptomatic and symptomatic college-aged women (Dakanalis, Timko et al., 2016).
Amongst young adult men, strong concurrent relationships between body dissatisfaction, appearance-ideal internalization, negative affectivity, and component symptoms of EDs have long been observed (Dakanalis & Riva, 2013a), with symptoms remaining relatively stable over the college period (Cain et al., 2012). Additionally, recent longitudinal research with late adolescent boys and young adult men indicated that body discontent motivates later dieting attempts as a means of losing subcutaneous body fat (that can hide musculature) and appearing more consistent with the male lean-muscular ideal standard, which in turn predict binge-eating (Dakanalis, Carrà, Calogero et al., 2015), followed by compensatory behaviours (Dakanalis, Clerici et al., 2016). Whether body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity predict future onset and/or maintenance of diagnosable EDs in male samples, as in female samples, remains uncertain (Culbert et al., 2015). Nonetheless, the reviewed evidence (Dakanalis & Riva, 2013a) that (a) only a subset of young adult men meet diagnostic criteria for EDs, even though the majority of this population report high appearance-ideal internalization, dieting and body dissatisfaction rates, and (b) negative affectivity also predates and maintains other psychopathological conditions (i.e., substance abuse) highlight the importance to identify additional specific factors that distinguish between men who do and do not develop and/or maintain an ED. Identification of new risk factors could be useful for improving the effectiveness of prevention programmes by enabling clinicians to gear them toward and address needs of young men who are at particularly high risk (Raevuori et al., 2014). Identification of new maintenance factors to be targeted in existing treatment approaches for improving recovery rates or to guide the design of novel interventions in men, which account for up to 25% of all eating disordered cases (Dakanalis & Riva, 2013a), is also important. It is arguably more important to identify men at increased risk for the onset and maintenance of any ED (including OSFEDs) since a substantial amount of those who do seek treatment have OSFEDs, and prevention programmes should ideally target all EDs, rather than just one type of ED/OSFED (Raevuori et al., 2014; Stice et al., 2011).
The tendency to experience one's body from an outside observer's (or third-person) perspective (i.e., principally as an object, to be evaluated for its appearance rather than for its effectiveness) is a major target of such investigation (Dakanalis & Riva, 2013a; Tiggemann, 2013). This experience, i.e., self-objectification, describes a particular perspective on the (bodily) self - a form of self-consciousness characterised by habitual and constant monitoring of the body and thinking of it in terms of how it looks (Riva, Gaudio, & Dakanalis, 2015). Though traditionally studied in relation to women's ED pathology, accumulated reviewed evidence from research involving young adult men (Dakanalis & Riva, 2013a, 2013b; Hausenblas et al., 2013; Tiggemann, 2013) indicates that (a) they are preoccupied with how their body appears from a third-person perspective, (b) opportunities for self-objectification (i.e., experimental or daily exposure to media idealized-images or appearance-focused comments/conversations) result in increased body dissatisfaction, dieting, and negative affectivity, and (c) experimental manipulations of self-objectification increased self-reported component symptoms of EDs. In addition, to reliably distinguish individuals (also males) with any type of ED (OSFEDs included) from healthy controls, the degree of self-objectification influences the severity of ED pathology and comprehensive recovery from any type of ED is associated with reduced levels of this variable (e.g., Dakanalis, Carrà, Timko et al., 2015; Dakanalis, Timko, Clerici, Riva, & Carrà, 2015; Fitzsimmons-Craft, Bardone-Cone, & Kelly, 2011; Riva et al., 2015; Tiggemann, 2013). Nevertheless, little is currently known about the role of self-objectification as a prospective predictor of the onset and/or maintenance of diagnosable EDs.
Using data from an on-going longitudinal study on men's eating and mental health issues, we sought to examine the influence and utility of self-objectification and another four traditionally accepted vulnerability factors (body dissatisfaction, appearance-ideal internalization, dieting, negative affectivity; Culbert et al., 2015) in predicting the onset and maintenance of men's (DSM-5) EDs at 4-year follow-up. The relative variance explained by each of the emerged predictors was examined to identify the most salient contributor to both ED onset and maintenance.
MethodDesign and participantsAs part of an on-going longitudinal study on men's eating and mental health issues (from college entrance to after graduation) all first-year male students identified through the registrar's database of one of the largest Italian universities were contacted via e-mail and invited to respond voluntarily to an online survey in autumn 2010 [first college year; Time 1 (T1)/baseline] and 2014 [last college year; Time 2 (T2)/follow-up]. Of those who were initially contacted (N=3,303), 2,689 men responded to the survey at T1. The participation rate (81.4%) is quite close to that reported by other studies involving the same recruitment methodology (i.e., 80.4% for Dakanalis, Clerici et al., 2016). Additionally, based on the information provided by the registrar (at T1) regarding age, diversity of family socio-economic status and region of residence before university, and ethnic composition of all first-year male students, analyses (i.e., two-tailed t-test for age and χ2 test for the remaining category variables; Reid, 2014), not shown but available on request, revealed no significant differences in any of these demographic variables between non-participants and participants. Thus, according to the registrar's database of the university from which the sample was recruited, the geographical region of residence before university (33% Northern Italy, 31% Central Italy, 32% Southern Italy, and 4% out of Italy), family socio-economic status (60% middle class, 20.5% lower-middle class, and 19.5% upper-middle class), ethnic composition (78.5% Caucasian, 8.5% Hispanic/Latino, 7% Asian, and 6% other or mixed ethnic heritage), and age (M=18.5, SD=1.41 years) of male first-year college participants was representative. At T1, participants had a mean body mass index (BMI) of 23.48 (SD=5.89) kg/m2; the majority of them were identified as heterosexual (92.5%) and reported they did not reside with their parents (90%). Of the 2,689 participants who responded to the T1 survey, 2,507 (93.2%) men (final analytic sample) responded to the survey at T2. Attrition analyses verified that participants who provided data at both time points did not significantly differ from those who only provided data at T1 on all aforementioned continuous (i.e., age, BMI) and categorical (i.e., ethnic composition) demographic variables, and also on mean scores of all measures of putative factors (described in instruments subsection that follow) and survey-based ED diagnostic rates determined through algorithms applied to the responses on Eating Disorder Diagnostic Scale (EDDS) items (as detailed in the instruments subsection). Due to the space constrictions, the results of the aforementioned attrition analyses (performed through two-tailed t-test and χ2 test for continuous and categorical variables, respectively; Reid, 2014) are available on request.
Using a two-stage design (Holland, Bodell, & Keel, 2013), men whose survey responses on EDDS items indicated they met DSM-5 criteria for any ED (OSFEDs included) at T1/baseline or T2/follow-up (“cases”, N=184) and “controls” (matched on demographics and BMI; N=185) were invited to participate in a face-to face interview assessment in a case-control design in which interviewers/clinicians were blind to survey-based (EDDS) diagnoses; further details are embedded in the instruments and procedure subsections below. A total of 333 men (91% and 90% of the invited cases and controls) volunteered for interview assessments, conducted up to two months after the time frame on which survey-based diagnoses were made; the overall participation rate is quite close to that reported by other studies using the same design (i.e., 89.9% for Holland et al., 2013) and comparisons (available on request) of survey- or interview-based diagnostic rates (through χ2 test) and mean scores of all measures of putative factors (through t-test), described below, revealed no significant differences between participants and non-participants with and without EDs/OSFEDs.
InstrumentsSelective standardized questionnaires and clinical interviews with well-established psychometric properties among Italian ED patients (men included) and community-based male samples were used to assess EDs and all putative factors in this study.
- -
EDs. The Italian EDDS (Conti, 2009) is a 22-item questionnaire (combination of Likert, dichotomous and frequency scores, and open-ended questions about weight and height, allowing BMI calculation) that assesses the DSM-IV criteria for EDs and generates both a symptom composite scale (reflecting the overall level of disordered eating symptoms) and a diagnostic scale. As detailed elsewhere (Flament et al., 2015), the EDDS also provides all relevant information to assess the DSM-5 criteria for EDs with the exception that items assessing criteria for BED referred to the past 6 months (i.e., duration stipulation of the DSM-IV). In our study, these items were adapted to cover the past 3 months (i.e., duration stipulation of the DSM-5) consistent with the adaption made by prior research, which also provided accompanying (adapted) computer algorithms to generate DSM-5 diagnoses (Flament et al., 2015). By applying these algorithms to the survey data, participants were classified as meeting (or not) DSM-5 criteria for threshold EDs or OSFEDs at T1 and T2. EDs were collapsed across diagnoses and thus measured as a dichotomous variable (present v. absent) in line with prior community-based studies noticing that the prevalence of diagnosable EDs is not in favour of an examination of associations of vulnerability factors with specific threshold ED and OSFED entities (Stice et al., 2011), particularly in men (Holland et al., 2013). Employing the Italian Eating Disorder Examination (EDE) 17.0D (Calugi et al., 2015) as a gold-standard interview for assessing DSM-5 EDs in our case-control design (described above), sensitivity (ranging from .91 to .93) and specificity (ranging from .99 to 1.00) of the survey-based diagnoses (based on the EDDS) were excellent at each time point. Since survey data was available for the full sample (N=2,507), and in consideration of the high level of agreement between survey-based and interview-based diagnoses (κ=.90-.93), survey-based diagnoses were used in this study to allow diagnostic status of a larger sample to be determined, crucial for examining predictors of ED onset and maintenance separately (Holland et al., 2013).
- -
Putative factors. The 8-item Body Surveillance subscale of the Italian Objectified Body Consciousness Scale (Dakanalis, Timko, Clerici et al., 2015), which measures the extent to which people consistently think and monitor their own body's outward appearance from an external observer's (third-person) perspective, was included as the gold-standard measure of self-objectification (Tiggemann, 2013). Following relevant recommendations (Dakanalis & Riva, 2013a), the Italian 10-item Male Body Dissatisfaction Scale (Dakanalis, Timko, Madeddu et al., 2015) was included as the gold-standard measure of men's levels of body dissatisfaction. The 9-item General Internalization subscale of the Italian Sociocultural Attitudes Towards Appearance Questionnaire-3 (Conti, 2009; Dakanalis, Zanetti et al., 2015) and the 10-item Negative Affect subscale of the Italian Positive and Negative Affect Schedule (Terracciano, McCrae, & Costa, 2003) were used to assess appearance-ideal internalization and negative affectivity, respectively. Finally, and consistent with prior ED research (e.g., Stice et al., 2011), the 10-item Restrained Eating subscale of the Italian Dutch Eating Behaviour Questionnaire (Dakanalis et al., 2013) was used to measure dieting. In our final analytic sample (N=2,507), just as in subgroups of participants with and without EDs, the internal reliability (α) estimates of each measure were ≥.91 at each time point.
Data for this study was collected following the methodology we have already used successfully in the past and fully detailed elsewhere (Dakanalis, Clerici et al., 2016; Dakanalis, Timko et al., 2016). Briefly, students were contacted through the university's academic information technology centre at each time point. The e-mail message informed students about the study (including the possibility of being contacted, if selected, for a face-to-face interview) and efforts taken to ensure confidentiality of the online data, and directed volunteers to an online survey where they gave electronic informed consent and completed the study measures. The measures were identical at both time points, presented in a counterbalanced order, and formatted so that participants could not skip individual items. Men's surveys from the two waves were matched (100%) through the university ID (last five digits) and no duplicate or erroneous data suggesting inattentive or random responding to T1 and/or T2 surveys were identified. To allow for independent assessment of ED diagnosis, clinicians with at least 10 years’ experience in assessing and treating men's EDs conducted all interviews (κ=1.0 at both time points) in the case-control design described above and detailed elsewhere (Holland et al., 2013). All consenting participants provided written informed consent and assessments took place on the college campus (89%) or in participants’ houses. The ethics review board of the co-ordinating body of the project (UniPV) approved the study.
Data analysisDescriptive statistics on changes in (DSM-5) ED diagnostic status from T1 to T2 (Table 1) are provided. Differences in T1/baseline putative factors/predictors among four groups of participants (described in Table 2) classified based on the presence or absence of an ED at each wave of assessment (e.g., Dakanalis, Timko et al., 2016) were assessed in SPSS 21.0 (IBM, NY) through MANOVA, preceded by checking that the data met all assumptions associated with this statistical technique (i.e., homogeneity of the variance-covariance), and followed by post-hoc tests (Tukey's B) (Reid, 2014). Subsequently, logistic regression models examined the association between each baseline putative predictor (T1) and change in the predictor (T2 - T1) with T2 ED status: “onset” (v. onset-free) or “maintenance” (v. cessation) (Table 3). Each predictor (baseline/T1 value and change value) was entered in a separate/individual model that was adjusted for BMI and disordered eating symptom levels at study entry and changes in BMI between assessments, as recommended (e.g., Dakanalis, Timko et al., 2016); because of the results of pre-analyses demographic variables (other than BMI), described above, were not entered as covariates in the planned analyses. Using SAS 9.3 (Cary, NC) software, one set of these (five) individual models examined the impact of each putative predictor on T2 “onset” amongst individuals without an ED at T1, and the second set of models examined the impact of each putative predictor on T2 “maintenance” amongst individuals with an ED at T1. Consistent with the study goals, Max-rescaled R2, i.e., the only measure of predictive power offered by SAS 9.3 (Cary, NC) for binary logistic regressions (Allison, 2012), examining the explanatory, predictive, value of a model, was calculated for each individual predictor model and for (logistic regression) combined models examining all statistically significant individual predictors and adjustment variables entered together and adjustment variables only.
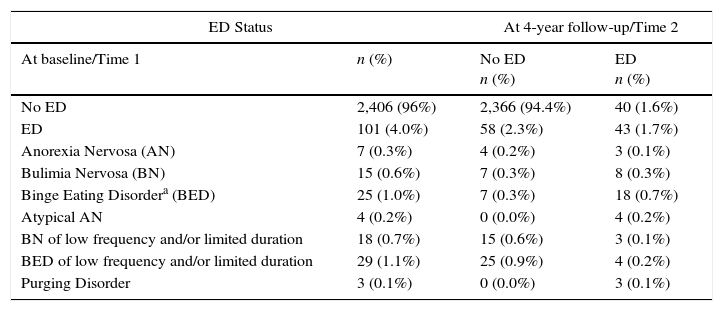
Changes in DSM-5 eating disorder (ED) status from baseline to 4-year follow-up (N=2,507).
| ED Status | At 4-year follow-up/Time 2 | ||
|---|---|---|---|
| At baseline/Time 1 | n (%) | No ED n (%) | ED n (%) |
| No ED | 2,406 (96%) | 2,366 (94.4%) | 40 (1.6%) |
| ED | 101 (4.0%) | 58 (2.3%) | 43 (1.7%) |
| Anorexia Nervosa (AN) | 7 (0.3%) | 4 (0.2%) | 3 (0.1%) |
| Bulimia Nervosa (BN) | 15 (0.6%) | 7 (0.3%) | 8 (0.3%) |
| Binge Eating Disordera (BED) | 25 (1.0%) | 7 (0.3%) | 18 (0.7%) |
| Atypical AN | 4 (0.2%) | 0 (0.0%) | 4 (0.2%) |
| BN of low frequency and/or limited duration | 18 (0.7%) | 15 (0.6%) | 3 (0.1%) |
| BED of low frequency and/or limited duration | 29 (1.1%) | 25 (0.9%) | 4 (0.2%) |
| Purging Disorder | 3 (0.1%) | 0 (0.0%) | 3 (0.1%) |
Differences on baseline putative factors across groups of participants with and without an eating disorder (ED) at baseline and 4-year follow-up.
| Group | Definition |
|---|---|
| Stable no-ED (n=2,366) | Participants without an ED at baseline and 4-year follow-up |
| Onset (n=40) | Participants without an ED at baseline and with an ED at 4-year follow-up |
| Maintenance (n=43) | Participants with an ED at baseline and 4-year follow-up |
| Cessation (n=58) | Participants with an ED at baseline and without an ED at 4-year follow-up |
| Baseline putative factors | Stable no-ED | Onset | Maintenance | Cessation |
|---|---|---|---|---|
| Self-objectification (possible score range: 1-7)a,b,* | 2.88 (1.01) | 5.00 (0.55) | 5.89 (0.40) | 4.44 (0.36) |
| Body dissatisfaction (possible score range: 9-54)a,b,* | 18.49 (6.45) | 32.99 (6.05) | 38.05 (5.60) | 28.04 (11.99) |
| Appearance-ideal internalization (possible score range: 9-45)a,b,* | 18.55 (5.50) | 30.02 (6.55) | 26.69 (8.19) | 23.99 (3.05) |
| Dieting (possible score range: 1-5)a,b,* | 1.85 (1.46) | 3.11 (0.70) | 3.83 (0.45) | 2.50 (1.04) |
| Negative affectivity (possible score range: 10-50)a,b,* | 17.51 (7.01) | 24.16 (4.44) | 26.96 (5.26) | 20.99 (5.00) |
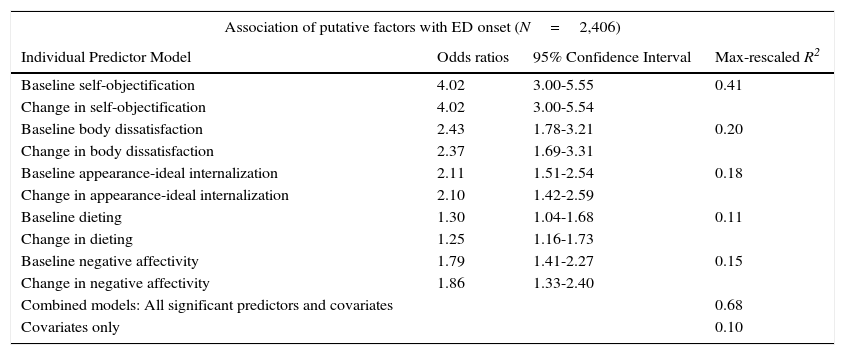
Logistic regression analyses predicting eating disorder (ED) onset and maintenance at 4-year follow-up.
| Association of putative factors with ED onset (N=2,406) | |||
|---|---|---|---|
| Individual Predictor Model | Odds ratios | 95% Confidence Interval | Max-rescaled R2 |
| Baseline self-objectification | 4.02 | 3.00-5.55 | 0.41 |
| Change in self-objectification | 4.02 | 3.00-5.54 | |
| Baseline body dissatisfaction | 2.43 | 1.78-3.21 | 0.20 |
| Change in body dissatisfaction | 2.37 | 1.69-3.31 | |
| Baseline appearance-ideal internalization | 2.11 | 1.51-2.54 | 0.18 |
| Change in appearance-ideal internalization | 2.10 | 1.42-2.59 | |
| Baseline dieting | 1.30 | 1.04-1.68 | 0.11 |
| Change in dieting | 1.25 | 1.16-1.73 | |
| Baseline negative affectivity | 1.79 | 1.41-2.27 | 0.15 |
| Change in negative affectivity | 1.86 | 1.33-2.40 | |
| Combined models: All significant predictors and covariates | 0.68 | ||
| Covariates only | 0.10 | ||
| Association of putative factors with ED maintenance (n=101) | |||
|---|---|---|---|
| Individual Predictor Model | Odds ratios | 95% Confidence Interval | Max-rescaled R2 |
| Baseline self-objectification | 3.94 | 2.98-5.24 | 0.40 |
| Change in self-objectification | 3.86 | 2.49-4.44 | |
| Baseline body dissatisfaction | 2.11 | 1.68-2.67 | 0.19 |
| Change in body dissatisfaction | 2.07 | 1.62-2.70 | |
| Baseline appearance-ideal internalization | 2.05 | 1.52-2.55 | 0.18 |
| Change in appearance-ideal internalization | 1.99 | 1.29-2.41 | |
| Baseline dieting | 1.37 | 1.15-1.80 | 0.12 |
| Change in dieting | 1.33 | 1.11-1.83 | |
| Baseline negative affectivity | 1.64 | 1.20-1.81 | 0.14 |
| Change in negative affectivity | 1.67 | 1.19-2.03 | |
| Combined models: All significant predictors and covariates | 0.67 | ||
| Covariates only | 0.11 | ||
Note. All models are adjusted for body mass index (BMI) and disordered eating levels at study entry, and BMI changes between assessments. All odds ratios are statistically significant (p<.05). R2 reflects the percentage of variance (R2value x 100) explained by separate (individual) and combined predictor models. Each of the five single (individual) predictor models includes baseline predictor, change in predictor and adjusted variables/covariates. The combined model includes all baseline predictors as well as change in predictor and adjusted variables/covariates.
Descriptive statistics on changes in ED diagnostic status from T1 to T2 appear in Table 1. At T1, 4% of the sample (n=101) met DSM-5 criteria for an ED. At 4-year follow-up/T2, 3.3% of the sample (n=83) met DSM-5 criteria for an ED, with 48.2% (n=40) of these cases representing new onset EDs, and 51.8% (n=43) of these cases representing men who had maintained an ED from baseline to 4-year follow-up).
As shown in Table 2, the MANOVA indicated differences on all T1/baseline putative factors across the four groups of participants classified based on the presence or absence of an ED at each wave of assessment, with subsequent post-hoc tests revealing that the groups differed significantly from each other in mean baseline scores of all putative factors. The significant differences between groups that were equivalent in terms of presence or absence of an ED at baseline/T1 but showing different outcomes at follow-up/T2 were of interest. Specifically, the “onset” group (i.e., without an ED at T1 and with an ED at T2) reported greater baseline scores on all putative factors as compared to the “stable no-ED”, or onset-free, group (i.e., without an ED at both time points). Likewise the “maintenance” group (with an ED at both time points) reported greater baseline scores on all putative factors as compared to the “cessation” group (i.e., with an ED at T1 and without an ED at T2).
Odds ratios (ORs) from individual predictor models for associations of predictors with T2 “onset” (v. onset-free) and “maintenance” (v. cessation) are shown in Table 3. Amongst individuals without an ED at baseline/T1 assessment, higher levels of self-objectification, body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity at T1 were significantly associated with the “onset” of an ED at T2/follow-up. Amongst those with an ED at T1, higher levels of self-objectification, body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity at T1 were significantly associated with ED “maintenance” at T2/follow-up. Changes in all individual predictor variables between assessments (i.e., from T1 to T2) were also significantly associated with both the “onset” and “maintenance” of an ED at T2/follow-up; ORs were comparable in magnitude to those for the individual predictor values at T1 (Table 3). Importantly, we also confirmed significant findings when restricting analyses to those for whom ED diagnosis was checked/confirmed by the clinical interview in the case-control design.1
Examination of max-rescaled R2 values, also reported in Table 3, indicated that the individual predictor model with the greatest explanatory/predictive value in explaining either “onset” (R2=.41) or “maintenance” (R2=.40) ED was the self-objectification model. In each individual predictor model, the remaining predictors (body dissatisfaction, appearance-ideal internalization, dieting, negative affectivity) had only half (or less) of the explanatory strength for either “onset” or “maintenance” ED. The explanatory value of the combined model, including all statistically significant individual predictors and adjusted variables/covariates (BMI and disordered eating levels at study entry, and changes in BMI between assessments) entered, was high (R2=.68 for onset, .67 for maintenance); the only covariates explained 10% and 11% of the variance in the “onset” and “maintenance ED, respectively.
DiscussionUsing longitudinal data we examined the influence of relevant factors in predicting the onset and maintenance of men's (DSM-5) EDs at 4-year follow-up. Our findings showed that elevated self-objectification, body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity at baseline as well as changes in these factors between assessments were significantly associated with future ED onset. Interestingly, greater initial levels in the aforementioned five factors as well as changes in these factors between assessments also predicted ED maintenance, with ORs comparable to those for individual predictor variables contributing to the ED onset (Table 3). However, examination of the variance explained by each of the examined factors indicates that men's self-objectification tendency emerged as the strongest predictor of both ED onset and maintenance.
Our findings regarding body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity converged with those found in prior studies investigating their role on ED onset amongst adolescent girls (e.g., Culbert et al., 2015; Stice et al., 2011) and on the development and persistence of college women's clinically significant ED pathology (e.g., Dakanalis, Timko et al., 2016). This implies that the effects of these variables are moderately robust and potentially not gender specific. The findings regarding self-objectification are novel and should inform preventive and treatment research. Hyper-focused attention on, and constant monitoring of, the body's appearance (characterizing self-objectification) has been consistently found to be an outcome of the appearance-ideal internalization in both sexes (Tiggemann, 2013). It has also been found to magnify the discrepancy between actual and ideal body attributes and/or perceived body imperfections (Hausenblas et al., 2013; Riva et al., 2015). Thus, self-objectification and its cumulative effect may play a key role in the acceleration of body dissatisfaction, associated affective distress and/or dieting attempts, thereby potentiating meaningful increases in the risk of ED pathology (Dakanalis, Carrà, Timko et al., 2015; Fitzsimmons-Craft et al., 2011). Although support for this suggestion came from a recent study that followed (initially) asymptomatic adolescents of both sexes for four years (Dakanalis, Carrà, Calogero et al., 2015), self-objectification might also be involved in the maintenance process of ED pathology (Tiggemann, 2013). According to ED scholars, when patients with any ED continue to think and monitor their own body “from a third-person perspective, factors that contribute significantly to EDs (i.e., body dissatisfaction, dieting, negative affectivity) remain untouched” (Fitzsimmons-Craft et al., 2011, p. 303). Research needs to validate this process and clarify the temporal sequence of the potential intervening experiences linking self-objectification to both the onset and persistence of ED pathology (Riva et al., 2015).
Even with longitudinal data and statistical control of several factors, unmeasured third variables (i.e., genetic factors) could account for the relationships observed (Culbert et al., 2015). The prevalence estimates of any DSM-5 EDs obtained in our sample at baseline/T1 (4%) and 4-year follow-up/T2 (3.3%) are consistent with those reported in comparable community surveys of young adult men (Holland et al., 2013) and the existing literature on the general population of college-aged men (Dakanalis & Riva, 2013a; Raevuori et al., 2014). The sample size of symptomatic and asymptomatic participants was also appropriate (i.e., above the recommended 10:1 cases-to-variable ratio, Allison, 2012) for individual and combined logistic regression models conducted for examining the impact of each predictor and all five predictors on “onset” and “maintenance” of any ED (Table 3), respectively. Yet the prevalence of specific DSM-5 ED diagnoses (Table 1) was too low to allow examination of associations of putative factors with specific threshold ED and OSFED entities. Although considerably larger prospective studies will be necessary to address this issue, it is worth noting that prior research supports the “trans-diagnostic” relevance of the variables considered in this study (e.g., Culbert et al., 2015; Dakanalis, Timko, Clerici et al., 2015; Fitzsimmons-Craft et al., 2011; Stice et al., 2011; Tiggemann, 2013). Additional descriptive data (not shown) indicating that none of T1 or T2 symptomatic participants reported receiving ED treatment before the T1 and between T1 and T2 assessments may suggest that our findings reflect a naturalistic progression of EDs and the vulnerability factors considered in this study. Despite evidence that the presentation format of measures (paper-and-pencil vs. online) did not change the quality of results (e.g., Dakanalis, Timko, Madeddu et al., 2015), all study variables embedded in online surveys were based on self-report data that is potentially susceptible to self-deceptive responding and assessment error (in the case of survey-based diagnoses). Importantly, survey-based diagnoses demonstrated concurrent validity with interview-based ED diagnoses in our sample, increasing confidence in the reported results. Moreover, we could confirm significant findings also when restricting analyses to those for whom ED diagnosis was checked/confirmed by the clinical interview in the case-control design. Although our analytic sample was representative (as mentioned in methods), men in the current study came from a selective northern Italian university; thus findings may not generalize to populations of dissimilar demographics, including inpatient samples. However, few available studies also involving men, and examining the stability of ED diagnoses in both community-based (Holland et al., 2013) and inpatient (Keel & Brown, 2010) samples reported rates of remission (57-58%) quite close to those observed in this study (57.4%, i.e., 58 of 101 men with an ED at T1 did not retain diagnosis at T2), thereby supporting the representativeness of longitudinal patterns observed in our sample. Additionally, although the duration between T1 and T2 assessment (4 years) was a strength of our study, we were not able to examine potential fluctuations or changes in ED status over the course of illness (i.e., between T1 and T2), and the examined factors may have demonstrated important associations with remission and relapse that we were unable to evaluate. In addition, future research should also test for interactions between the examined factors suggestive of qualitatively distinct risk/maintenance pathways (Dakanalis & Riva, 2013a). This could benefit from, for example, classification tree analyses that are also able to empirically derive cut-points for continuous measures (such as those used in this study for assessing the putative factors) and allowing optimal identification of young adult men at elevated risk for the onset and maintenance of DSM-5 EDs (Stice et al., 2011).
Despite the aforementioned limitations, our findings revealing that self-objectification, body dissatisfaction, appearance-ideal internalization, dieting, and negative affectivity were all predictors of both ED onset and maintenance highlight potentially similar psychological foci for prevention and treatment efforts. Importantly, self-objectification had greater explanatory value with regard to both ED onset and maintenance, as compared to the remaining four traditionally accepted risk/maintenance factors (Culbert et al., 2015). Thus, a focus on reducing self-objectification might be considered as a potential intervention strategy to prevent and treat young men's ED pathology. Indeed, recent research revealed that the addition of self-objectification as a target variable within traditional (evidenced-based) cognitive dissonance prevention programmes targeting appearance-ideal internalization, increased the reduction of undergraduate eating and body-related disturbances as well as the small-to medium effect sizes of these traditional programmes (Culbert et al., 2015). The leading empirically supported cognitive-behaviour (CB) treatment for BN, which has been successfully adapted with the goal of making it “trans-diagnostic” appears “more effective in reducing ED behavioural symptoms rather than producing changes in body image disturbance” (Dakanalis, Carrà, Timko et al., 2015, p.102). Hence, the use of CB or other interventions of proven efficacy in combination with promising approaches (i.e., virtual reality) designed to decrease the hyper-focus on, and scrutiny of, body appearance (characterizing self-objectification), and to address body dissatisfaction and negative reactions to one's image, might be helpful to decrease ED pathology and improve treatment outcomes (Dakanalis, Carrà, Calogero, Fida et al., 2015; Dakanalis, Carrà, Calogero, Zanetti et al., 2015; Dakanalis et al., 2014; Riva, Gaggioli, & Dakanalis, 2013; Riva et al., 2015).
FundingThe work was supported by a grant from the Onassis Foundation (O/RG 2010/G/A212). The authors report no declarations of financial interest.
Specifically, additional restricting analyses (available on request from the corresponding author due to space constrictions) of those individuals for whom ED diagnosis was confirmed by the clinical interview (i.e., EDE) in the case-control design (described in the methods/design and participants subsections) produced the same pattern of results, with ORs comparable to results described in Table 3 from analyses of survey-based data.
