




Electroconvulsive therapy (ECT) is effective for treatment-resistant and psychotic depression. One previously reported side effect of ECT is the disruption of memory reconsolidation. This study examines whether this disruption induced by ECT can be detected in routine neuropsychological assessments.
MethodsIn this retrospective study, the Autobiographical Memory Interview (AMI) was applied before and after ECT. Memories of the same events and facts were tested pre and post ECT treatments. 38 patients, receiving ECT for the treatment of unipolar or bipolar depression, were matched for age, sex, and stimulus intensity and divided into two groups: Group A was tested on the day before the first ECT treatment, whereas group B two or more days before.
ResultsPatients who were tested by AMI on the day before ECT and thus reactivated memorie shortly before the first ECT treatment deteriorated in AMI score. Patients who had at least two days between memory activation and treatment improved regarding the number of recalled memories. Memory impairment was not associated with depression severity.
ConclusionThis finding suggests that ECT might be capable of impairing reconsolidation. The study demonstrates that memories of personal events can potentially be affected by ECT within a time interval of 24 h of memory vulnerability after reactivation. Implications for practice and future research are discussed.
Electroconvulsive therapy (ECT) is a widely used and established procedure for the treatment of severe and/or chronic depressive symptoms within conditions of unipolar and bipolar depression. It involves the induction of seizures by the administration of electrical stimuli via electrodes placed on the scalp. Even though ECT is effective, various side effects are well known. Among these, memory impairments are frequently reported, although their full extent and nature is still under investigation. A possible explanation for some of these impairments can be understood as an interference of memory reconsolidation. Reconsolidation of memory describes the process in which memories are reorganized after initial encoding in the hippocampus and neocortex (Dudai & Morris, 2013). This integration of newly learned knowledge or experiences into already existing memories takes place every time these are reactivated. This seems to be a rather unstable state, in which a memory can also be changed or lost (Forcato, et al. 2007). Kroes et al. (2013) found that a single session of ECT was able to disrupt reconsolidation processes if memories that were induced during the study itself were brought to mind shortly before the ECT session. These memories could then no longer be recalled or only partially be recalled at a later point in time. These findings inspired further studies examining the possibility to reduce PTSD symptoms by reactivating traumatic memories directly before ECT being administered (Gahr, et al. 2014). Still, many questions regarding the processes of reconsolidation and its susceptibility to interference by ECT remain. In the present study, the ECT-induced manipulation of autobiographical memories, i.e. non-traumatic personal events and facts, was examined with a retrospective quasi-experimental design. These memories are more complex with regard to emotions and visual imagery, they seem to be distributed across a broader network of brain areas and usually require more time-consuming reconstructive processes than laboratory-based memories would (Daselaar, et al. 2008). We hypothesized that patients who had their autobiographical memories reactivated within 24 h before ECT would be impaired in the reproduction of those memories after treatment compared to patients who recalled their memories more than 24 h before the first ECT session.
MethodsAutobiographical memory interviewThe core instrument of the study comprises routine clinical data from the “Autobiographical Memory Interview” (AMI; Brakemeier, Kathmann & Bajbouj, 2005) which has been created as a hybrid version of the Autobiographical Old Memory Interview by Schmidtke and Vollmer-Schmolck (1999) and the Autobiographical Memory Interview by Kopelman et al. (1990). In its present version, the AMI has been applied in clinical studies, also in the context of ECT and depression (e. g. Brakemeier, et al., 2014). It is a structured interview that tests episodic and semantic autobiographical memories and is divided into four parts: the first part measures episodic autobiographical memory, which is compiled of three categories (Christmas Eve, vacations, and visits to the doctor within the last five years). Part two tests personal semantic knowledge by asking various questions about previous residences. Part three, old memory and childhood memories, tests both semantic and episodic knowledge from childhood. Part four tests general knowledge by asking questions about, for example, capital cities of Europe. The AMI consists of 71 separate items, the possible maximum and minimum scores are 71 and 0 points, respectively. The time required for testing varies greatly depending on how many and how detailed memories can be recalled by the test subject.
The strength of the AMI is to quantitatively measure and describe retrograde amnesia. There are no parallel versions for repeated testing. Thus, the same memories and facts were assessed pre and post ECT. A reduction in AMI scores can therefore not only be seen as a limitation in autobiographical memory, but also as a limited recall of a particular memory or factual knowledge.
ECT and data collectionAll patients were treated for unipolar or bipolar depression at the Department of Psychiatry and Neurosciences, Charité – Universitätsmedizin Berlin, Germany, and received routine neuropsychological assessment including the AMI pre and post ECT. All patients received unilateral, ultrabrief pulse ECT with a pulse length of 0.25 ms at a frequency of 20 Hz. ECT was performed 3 times per week and with no set limitation for the number of treatments. This high frequency phase is in the following referred to as acute ECT. Usually, between 6 and 15 ECT sessions were performed before a response was observed and treatment was shifted to treatment once weekly, then every other week and lastly monthly. This phase of treatment is in the following referred to as maintenance ECT. At the beginning of each ECT treatment, patients received a sedative and a muscle relaxant intravenously. Only pulses with a pulse length of < 0.5 ms were used with a unilateral electrode placement. Seizure duration was aimed to be between 20 and 60 s. However, correlations between seizure duration, seizure threshold and response rate do not seem to exist, as long as a minimum duration can be reached (Chung, 2002). For early detection of negative side effects, a series of neuropsychological tests was conducted before and after acute ECT treatment. In accordance with side effects most likely to appear, these tests focused on different memory systems. For study purposes, the data of 298 ECT patients treated and tested as mentioned above between 2012 and 2019 was collected. Retrospective data analyses for study purposes were approved by the ethics committee of Charité – Universitätsmedizin Berlin. Each case was then checked and filtered for diagnoses with potential confounding effects on memory, such as strokes. Regardless of severity, location and time of event, these patients were excluded from the survey. After also excluding all incomplete cases, which mostly stemmed either from discontinuation of treatment due to discharge or change of treatment, or rejection of neuropsychological testing by patients, 86 patients were included in the study and thus formed the basis for matching.
GroupingIn each patient included, a series of neuropsychological tests, including the AMI, had been administered before ECT treatment (T0) and after the last acute ECT (T1). Patients could be devided in two groups: In group A, testing took place within 24 h before the first ECT session. In group B, testing took place between 2 and 20 days before the first treatment. The loosely set time criteria for T0 in group B was caused by several factors. These included: 1. the urgency of the start of treatment, largely determined by the decisions made by the treating physicians and patients. 2. Availability of test personnel. 3. Availability of patients, determined by treatment plan and symptoms as well as various other individual factors.
MatchingTo minimize bias due to the quasi-experimental design of this study, patients were matched into pairs. Variables with the potential to influence the allocation of groups or test results were therefore defined as matching criteria. These are:
- 1
Age at treatment start. A tolerance of plus/minus five years was chosen for this criterion.
- 2
Sex.
- 3
Seizure threshold. The seizure threshold is relevant to patients' test results for two reasons and was therefore controlled for by matching. First, it indicates the stimulus intensity of the first ECT session, with the greatest temporal proximity to testing and the greatest potential to disrupt reconsolidation processes. On the other hand, the seizure threshold can be seen as an indicator of the stimulus intensity of further treatment, which cannot be excluded as an influencing factor on the test results.
Based on these criteria, 19 pairs of patients were determined who matched in all three characteristics. Each pair consisted of one patient from Group A and one from Group B.
Patient and treatment characteristicsIn addition to the three factors age, sex and seizure threshold, further patient and treatment characteristics were controlled to minimize their potential influence on the outcome. The aim was to ensure the best possible homogeneity of groups in all independent variables that might have affected memory performance due to the quasi-experimental study design. Although matching allows for higher quality results, group comparisons of variable distribution was preferred to maintain a reasonable sample size.
The variables chosen were:
- 1
Severity of depression: Depressed patients show a limited autobiographical memory compared to healthy controls (Farina, Barry, Damme, Hie, & Raes, 2019). To ensure that symptoms of depression were not a moderating factor, we controlled for the patients' symptom severity before and after ECT, determined by Montgomery Asberg depression rating scale, (MADRS) (Montgomery & Asberg, 1979).
- 2
Number of ECT sessions: To the best of our knowledge, there are no studies investigating the correlation between autobiographical side effects and number of ECT sessions. Therefore, an interaction cannot be ruled out and the total number of ECT sessions was controlled for.
- 3
Seizure duration: Influence of seizure duration on disturbances of memory has not been reported by previous studies (Daniel, Weiner, & Crovitz, 1983). However, prolonged seizures are correlated with delirium following the awakening (Tsujii, et al., 2019) which itself correlates with retrograde amnesias (Sobin, et al., 1995). An association between seizure length and retrograde amnesia could therefore not be ruled out, so the duration of seizure of the first ECT session was controlled for.
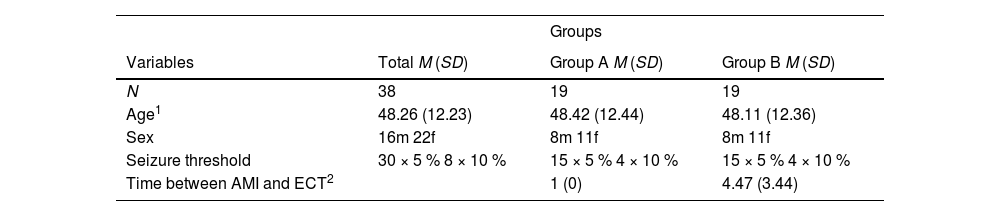
Groups A (AMI less than 24 h before first ECT session) and B (AMI more than 24 h before first ECT session) were matched according to age, sex, seizure threshold and time between AMI and first session of ECT. 19 matched pairs could be formed from the data set of N = 86, as displayed in Table 1.
Distribution of matching criteria.
| Groups | |||
|---|---|---|---|
| Variables | Total M (SD) | Group A M (SD) | Group B M (SD) |
| N | 38 | 19 | 19 |
| Age1 | 48.26 (12.23) | 48.42 (12.44) | 48.11 (12.36) |
| Sex | 16m 22f | 8m 11f | 8m 11f |
| Seizure threshold | 30 × 5 % 8 × 10 % | 15 × 5 % 4 × 10 % | 15 × 5 % 4 × 10 % |
| Time between AMI and ECT2 | 1 (0) | 4.47 (3.44) |
Notes.1Matched +/- five years. 2Measured in days. m = male; f = female
Then the two groups were compared regarding depression severity, as measured by the MADRS (Montgomery & Asberg, 1979), as well as seizure duration and total number of ECT sessions. Independent groups T-tests were conducted. No significant group differences were found. Furthermore, none of these variables were significantly correlated with the change in AMI score (see Table 2). There was no statistical difference between groups respective AMI baseline scores (p = .661)
Further patient and treatment characteristics
| Groups | |||||
|---|---|---|---|---|---|
| Variables | Total M (SD) | Group A M (SD) | Group B M (SD) | Mean group difference p | Correlation to AMI∆T0-T1r (p) |
| MADRS T0 | 30.38 (8.69) | 30.75 (9.48) | 30.06 (8.19) | .917 | .188 (.288) |
| MADRS T1 | 11.23 (8.37) | 12.17 (10.37) | 10.24 (5.7) | .974 | -.099 (.573) |
| MADRS T0-T1 | 18.51 (10.04) | 17.67 (11.7) | 19.31 (8.5) | .579 | -.185 (.320) |
| ECT sessions | 11.92 (2.32) | 12.37 (2.73) | 11.47 (1.8) | .317 | .103 (.537) |
| Seizure duration1 | 43.6 (22.3) | 40.4 (20,1) | 46.6 (24,3) | .549 | .112 (.504) |
Notes.1Measured in seconds by EEG
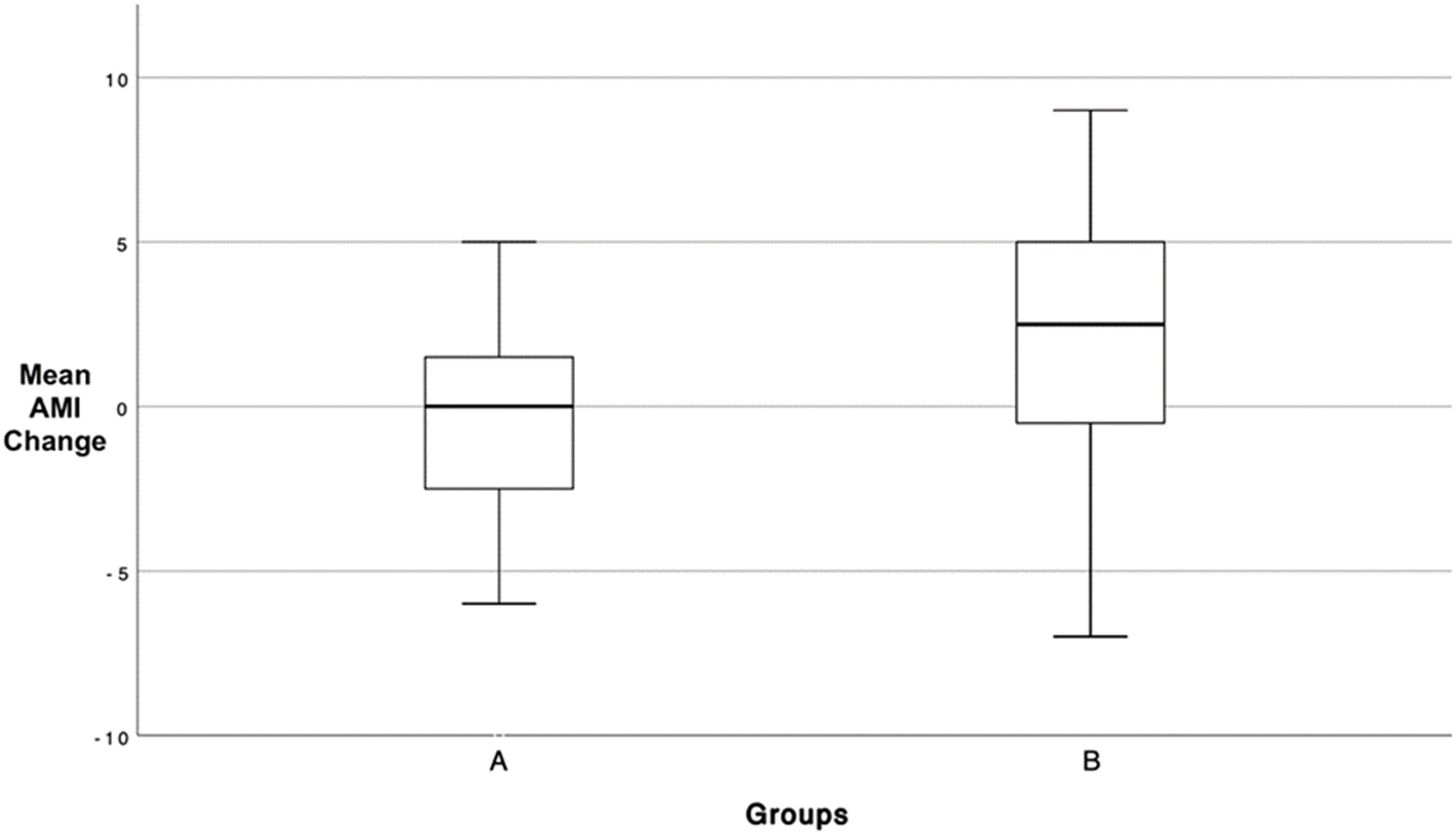
In group A, tested less than 24 h before ECT, the mean AMI score decreased by M∆ = –1.44, (SD = 1.56) from MT0 = 61.87 (SD = 8.27) to MT1= 60.42 (SD = 11.23). In group B, tested more than 24 h before ECT, the mean AMI score increased by M∆ = 2.42, (SD = 1.52) from MT0 = 62.95 (SD = 5.97) to MT1 = 65.37 (SD = 4.25).
To test the hypothesis that temporal proximity of AMI testing to ECT had a negative effect on post-ECT results, a Mann-Whitney-U test was performed.
The Mann-Whitney-U test confirmed the mean difference between the groups (∆MA, MB = 3.87) as statistically significant (p = .043). Consequently, patients with an AMI test < 24 h before ECT showed significantly worse AMI results post ECT (d = 0.56). According to Cohen's (1992) guidelines, this can be considered a medium effect size. A graphical representation of group means and the associated confidence intervals is shown in Fig. 1.
Discussion
In this study using a quasi-experimental design, the influence of ECT on patients’ reactivated autobiographical memories was evaluated depending on the temporal proximity of reactivation and ECT session. Our data show that patients who had been tested by AMI on the day before ECT, and thus reactivated memories, deteriorated in AMI score over the course of treatment. Patients who had at least two days between memory activation and treatment improved regarding the number of recalled memories. These results are consistent with Kroes et al. (2013) who observed a difference in memory performance between a group with reactivated memory and non-reactivated memory prior to ECT.
Our findings could even extend the results of Kroes et al. (2013): First of all, the time interval, in which reactivated memories were found to be vulnerable to interference by ECT, has been extended to 24 h prior to treatment. Second, the present findings demonstrate that the process of disrupted reconsolidation potentially induced by ECT does not seem to be limited to memories generated in an experimental setting but also applies to autobiographical memories. To our knowledge, this has only been demonstrated by one case study by Gahr, Schönfeldt-Leucona, Spitzer, & Graf (2014).
Moreover, our results show a significant difference depending on the time of reactivation: While in group B (tested two days or more before treatment) we saw an increase of the ability to recall these memories after ECT, in group A (reactivation within 24 h before ECT), the same ability decreased. It is not quite clear why group B showed an increase in recalled memories. The recall of certain autobiographical memories could have improved due to a test-retest effect, so the re-testing could have led to a better retrieval of recently reactivated memories. To test this effect, a control group without ECT treatment would have been necessary. While this effect would equally affect group A, it could have been concealed by the postulated impaired reconsolidation which we hypothesize would be stronger in group A due to the temporal proximity of AMI and ECT session as well as a potentially impaired consolidation of AMI learning.
In addition, we were not able to find a significant correlation between the AMI and either depression severity, change in symptoms of depression over the course of ECT treatment (both measured by MADRS) as well as seizure duration and number of ECT sessions. However, despite these results, an influence by these variables on AMI scores cannot be fully excluded and should be evaluated by future research. The lack of correlation is, at least, in line with recent findings in patients with depression where difficulties accessing specific memories seem to persist even after remission (Hallford, Rusanov, Yeow & Barry, 2022). Seizure duration is known to not have an influence on the efficacy of ECT as long as a minimum duration is reached (Delva, et al., 2000). It could be hypothesized that the same holds true for its influence on the retrieval of autobiographical memory. Previous studies were not able to show any influence of the number of ECT sessions on cognitive side effects (Kirov, et al. 2016). Our results seem to be in line with this finding. However, in both groups the variation of the number of ECT sessions was minimal (see Table 2) and therefore might not have been able to produce any effect.
The study has several limitations. One major point is the absence of data regarding neural activity and functional connectivity changes in the hippocampus due to the retrospective nature of the study. To fully demonstrate an impaired reconsolidation by ECT such data would be needed. Another limitation is its quasi-experimental design. Matching according to further criteria, such as duration of seizure, anesthetic medication, and severity of depressive symptoms would have been desirable but not feasible in our case. The design also did not allow for follow-up testing: Since data had been collected as part of routine clinical assessment pre and post ECT treatment, no data was available beyond the period of treatment. This does not allow for any statement about the duration of observed effects. Since patients’ subjective reports of cognitive side effects of ECT might be more pessimistic than previous studies have concluded (Brakemeier, et al. 2011), long-term observations of cognitive side effects would be particularly helpful. Moreover, the study design does not allow conclusions regarding the effects of individual ECT sessions, as no further assessments were conducted during the course of treatment. Lastly, the risk of confabulations and the inability to detect them, pose another problem in interpreting the results. Some items of the AMI are not falsifiable by their nature. Primarily emotional memory items cannot be answered correctly or incorrectly, but rather answered or not answered. This leaves room for errors in measurement due to confabulations or deliberately untrue reports. Along that line it might have been preferable to apply an autobiographical memory test that had been validated in large populations, as for the AMI version used here, no psychometric properties are available yet, so it was not possible to calculate the Reliable Change Index. Findings of this retrospective approach might nevertheless inspire future prospective studies, which may be better able to demonstrate the potential relation between ECT and changes in autobiographical memory recall.
The study results show how autobiographical memories are potentially affected by ECT treatment in patients with depression. It is common practice to combine ECT with other treatment forms, primarily in-patient psychotherapy. As reactivation of personal memories in therapy sessions before and during the course of ECT treatment is quite common, psychotherapists should be aware of a possible interference of ECT and reactivated autobiographical memories. To avoid the risk of “losing” such memories, even if temporary, a better understanding of impaired reconsolidation through ECT is needed. However, in some cases altered memory reconsolidation could be the intention of treatment: Gahr et al. (2014) presented a case of a patient with PTSD whose trauma-related symptoms could be reduced by reactivating traumatic memories before ECT treatments. In a recent randomized controlled trial (Tang, et al. 2021) memory reactivation pre ECT has not been observed to have an effect on PTSD symptoms though. Traumatic memories have been shown to differ from non-traumatic memories in their neurofunctional mechanisms with an increased activity in amygdala, hippocampus, lateral temporal, retrosplenial, and anterior cingulate cortices (Piefke, et al. 2007). Their narratives are also more dominated by sensorial/perceptual and emotional details (Crespo & Fernández-Lansac, 2016), suggesting that traumatic memories considerably differ from non-traumatic memories in various ways. Due to the not yet fully understood difference between traumatic and non-traumatic memories as well as the limited number of studies, more research is needed to explore whether ECT could be used to specifically alter reconsolidation of traumatic memories. Also, as long-term effects are not well understood so far, further studies should focus on the time interval of memory vulnerability as well as on the question which types of autobiographical memories are mostly affected.
