



Background/Objective: A weight-related Quality of Life (QoL) questionnaire elicits parents’ perceptions to understand the impacts of weight on children's QoL. Sizing Them Up, a parent-proxy of a weight-related instrument, is a proper measure for the purpose, but its psychometric properties have not been validated on a non-clinical child population. This study aimed to thoroughly examine the psychometric properties of the Sizing Them Up on a non-clinical child population. Methods: Children from Taiwan (Mage=11; SD=1.02; N=236) filled out a weight-related QoL instrument (Sizing Me Up) while their parents completed Sizing Them Up and two generic QoL instruments. Confirmatory factor analysis (CFA), concurrent validity, and known-group validity were conducted. Results: CFA supported the factor structure of Sizing Them Up. The concurrent validity of the Sizing Them Up total score was satisfactory: r=.46 to .53 with other QoL instruments. Known-group validity was supported as obese children had significantly lower Sizing Them Up total score than did normal-weight and underweight children. Conclusions: We extended the use of Sizing Them Up from clinically obese children to a community-based sample of underweight as well as overweight children. Healthcare providers may use Sizing Them Up to measure the weight-related QoL for children.
Antecedentes/objetivo: Un cuestionario que relaciona peso y calidad de vida (CV) estimula la percepción de los padres para comprender los impactos del peso sobre la CV de los niños. Sizing Them Up es un instrumento para padres, relacionado con el peso, pero sus propiedades psicométricas no se han validado en población infantil no clínica. Este estudio examina minuciosamente dichas propiedades en una población infantil no clínica. Método: Niños de Taiwán (Medad=11,00; DT=1,02; N=236) completaron el Sizing Me Up, mientras sus padres completaron este mismo instrumento y otros dos genéricos de CV. Se realizó análisis factorial confirmatorio (CFA), y se examinó la validez concurrente y validez de grupo conocido. Resultados: El CFA apoya la estructura factorial del Sizing Them Up. La validez concurrente fue satisfactoria. La validez de grupo conocido fue apoyada, ya que los niños obesos obtuvieron una puntuación en Sizing Them Up significativamente menor que los niños de peso normal o bajo peso. Conclusiones: Los proveedores de atención médica pueden utilizar Sizing Them Up para medir la CV relacionada con el peso de los niños.
The rising prevalence of overweight and obesity has been described as a global pandemic (Popkin, Adair, & Ng, 2012; Swinburn et al., 2011), and the long-term consequences may lead to detrimental threats to the economy and healthcare systems (Trasande & Chatterjee, 2009), a possibility that should increase our awareness of childhood overweight and obesity, which can cause unfavorable health conditions later in life (Wardle, Brodersen, Cole, Jarvis, & Boniface, 2006). Between 1980 and 2013, the combined global prevalence of childhood overweight and obesity rose by 47.1% (Chang, Wu, Chen, Wang, & Lin, 2014). More specifically, the prevalence of overweight and obese children was estimated to be 23.8% for boys and 22.6% for girls in developed countries, and 12.9% for boys and 13.4% for girls in developing countries (Karnik & Kanekar, 2015; Ng et al., 2014). In Taiwan, the prevalence of obesity and overweight in children 6-13 years old is 30.2% for boys and 23.5% for girls (Lin, Su, Wang, & Ma, 2013), which is comparable to the trend in developed countries, except that the rate for boys is higher in Taiwan, regardless of age (Liou, Huang, & Chou, 2009). Chronic overweight puts a child at great risk of weight-related physical, emotional, and social deficits (Jafari, Allahyari, Salarzadeh, & Bagheri, 2016). Indeed, studies showed that weight-related issues such as body dissatisfaction or impaired body image may contribute to a person's psychological problem: eating disorder (Dakanalis et al., 2016; Lucena-Santos, Carvalho, da Silva Oliveira & Pinto-Gouveia, 2017). These problems should be investigated and measured along with health-related quality of life (HRQoL) in local and international discussions about weight management and overweight prevention (Ahuja et al., 2014; Lin, Su et al., 2013).
HRQoL contains a broad range of elements that explains how quality of life (QoL) influences the physical health, psychological condition, social interaction, independence, and environmental impact of an individual (World Health Organization, 1993). Evaluating HRQoL provides subjective perceptions of overall health and well-being, which is information essential for healthcare decision-making, especially when we want to understand which treatment (e.g., practicing physical activity) is effective (Carbó-Carreté, Guàrdia-Olmos, Giné, & Schalock, 2016). Yet, in practical terms, these generic instruments are designed to compare children's general health condition to certain diseases such as obesity for further clarification, but not to identify emerging weight-related concerns. Studies show that, even when using standard medical criteria, many people misclassify their weight status due to overlooking contextual factors, such as cultural/ethnic preferences of body size or obesity bias (Cachelin, Rebeck, Chung, & Pelayo, 2002; Olvera, Suminski, & Power, 2005). It is, therefore, necessary to assess whether using a particular instrument is suitable for a non-clinical population, such as children from a community (Eiser & Morse, 2001), in order to monitor children's health and detect potential weight-related problems early.
When a generic instrument for investigations or follow-up interventions is used, specific health conditions might not subsequently be considered for in-depth measurement (Ahuja et al., 2014). For instance, even though the psychosocial outcomes of obese children are important, they are often under-reported. This might jeopardize the chances of assessing and managing their health condition (Al-Hashimi, Davis, & Bull, 2016). Therefore, a weight-related questionnaire about QoL might be needed to more precisely measure QoL for overweight and underweight children.
Also, being brief but comprehensive, and having adequate psychometric properties, are essential for developing a HRQoL instrument with both self-report and parent-proxy report versions (Eiser & Morse, 2001). Children's subjective evaluations, combined with parallel parental perceptions, can help shape a more precise description of children's QoL (Varni, Seid, & Kurtin, 2001; Varni, Seid, & Rode, 1999). That is, the proxy report is a helpful and fairly accurate approach when children are unable to respond to measures themselves because of their youth or difficult health conditions. Even though discrepancies between parent-proxy reports and child self-reports were found, parent-proxy reports can give healthcare professionals a more holistic picture of children's QoL (Upton, Lawford, & Eiser, 2008); for example, healthcare providers can know how the parents percieve their children's health. Parental perspectives are also more likely to influence whether or not healthcare services are sought (Tsiros et al., 2009).
Parents who observe their children engaging in various activities are, therefore, more familiar with their children's feelings and thoughts than are parents who do not may be able to provide more comprehensive estimations of their child's QoL. Although parents’ ratings might be biased because of their parenting expectations or their own concerns, their children's subjective reports can balance out and reconcile those ratings to create a more precise description of QoL (Chan, Mangione-Smith, Burwinkle, Rosen, & Varni, 2005).
With the aforementioned features, Sizing Them Up, a parent-proxy weight-related instrument, is a proper measure for evaluating the HRQoL of overweight and obese children. Only one American study (Modi & Zeller, 2008) has validated Sizing Them Up using clinically obese children, and no other study has validated the psychometric properties of this measure. Furthermore, the factor structure of Sizing Them Up has been tested using only exploratory factor analysis (EFA). Hence, our study aimed to fill this research gap by (1) testing the factor structure of Sizing Them Up with a confirmatory factor analysis (CFA); and by (2) extending the use of Sizing Them Up from clinically obese children to a community-based sample that includes underweight and overweight children.
MethodParticipantsThe Institutional Review Board of the National Cheng Kung University Hospital approved our study protocol (IRB No. ER-98-0256), and we did the study between February 12 and July 11, 2010, in the Southern Taiwan. With the help of teachers in the 11 elementary schools, we enrolled 236 parent-child dyads for this study, and each dyad signed an informed consent. Each child filled out a weight-related QoL instrument (Sizing Me Up), and each parent completed the following questionnaires: a weight-related QoL instrument (Sizing Them Up), two generic QoL instruments (KINDL and PedsQL), and a background information sheet. In addition, 82 parents completed the Sizing Them Up again after 7 to 14 days.
InstrumentsBody Mass Index. Anthropometric data of the children were obtained from school records, and that of the parents was based on the height and weight that they provided. Body mass index (BMI) was then calculated and used to assign each child and parent to a weight status. The cutoffs for parents were based on the general standards in Taiwan, where BMI<18.5 is underweight; 18.5-24 is normal weight; 24-27 is overweight; and>27 is obese (Pan et al., 2004). The children's gender and age difference cutoffs were considered; detailed cutoff information is available elsewhere (Chu & Pan, 2007).
Sizing Them Up and Sizing Me Up. Sizing Them Up and Sizing Me Up contain 22 items each. They were developed to capture children's weight-related QoL (Modi & Zeller, 2008; Zeller & Modi, 2009). Sizing Them Up is a parent-proxy report, and has acceptable internal consistency (alpha=.59 to .91), test-retest reliability (intraclass correlation coefficient [ICC]=.57-.80), and convergent validity (r with two other QoL instruments on similar constructs=.22-.70 [Modi & Zeller, 2008]). There are 7 domains (Emotion, Physical, Teasing/Marginalization, Positive Attributes, Mealtime, School, and Adolescent Developmental Adaptation) in Sizing Them Up; however, we did not use the Adolescent Developmental Adaptation domain because none of our participants were adolescents. Sizing Me Up is a child-reported QoL instrument, and has acceptable internal consistency (alpha=.68-.85), test-retest reliability (ICC=.53-.78), and convergent validity (r with other QoL instruments similar constructs=.35-.65 [Zeller & Modi, 2009]). There are 5 domains (Emotion, Physical, Social Avoidance, Positive Attributes, and Teasing/Marginalization) in Sizing Me Up. In addition, the underlying structure has been supported using CFA in community samples (Cushing & Steele, 2012), including a Taiwanese sample (Strong, Lin, Tsai, & Lin, 2017). The stem of each item in Sizing Me Up is “…because of your size”, and in Sizing Them Up is “…because of their weight/shape/size”. Each item describes a condition from the previous month for respondents to answer. Response descriptors are none of the time, a little, a lot, and all of the time for Sizing Me Up, and never, sometimes, often, and always for Sizing Them Up. The developers suggested that the items in both instruments be converted into a 0-100 scale with a higher score indicating a better QoL.
Parent-proxy KINDL. The KINDL includes 24 items that ask about the frequency of a condition (e.g., had a headache; felt alone; had lots of good ideas; felt fine at home; played with kids; enjoyed my lessons) that occurred in the previous week. It is scored using a 5-point Likert scale: 1 point=“always” and 5 points=“never”; negatively worded-items are reversely coded (Lin, Luh et al., 2013; Ravens-Sieberer et al., 2006). The parent-proxy KINDL has been translated into Mandarin, and the psychometric properties of its score were satisfactory for Taiwan's population (Lee, Lin, Tsai, Strong, & Lin, 2016). We used the total score of the parent-proxy KINDL as a criterion for testing concurrent validity, with a higher score representing a better QoL. Thus, positive correlations between Sizing Them Up and KINDL were anticipated.
Parent-proxy PedsQL 4.0. The PedsQL includes 23 negatively-worded items which ask the frequency of a condition (e.g., hard to run; feel angry; have trouble getting alone with other kids; forget things) that occurred in the previous two weeks. It is scored using a 5-point Likert scale: 0 points=“never” and 4 points=“almost always” (Chan et al., 2005; Varni et al., 2001). The parent-proxy PedsQL has been translated into Mandarin, and the validity and reliability of its score were satisfactory for Taiwan's population (Cheng, Luh, Yang, Su, & Lin, 2015; Lin, Su et al., 2013). In addition to the total score of KINDL, we used the total score of the parent-proxy PedsQL as another criterion for testing concurrent validity, with a higher score representing a better QoL. Thus, positive correlations between Sizing Them Up and the PedsQL were expected.
Translation procedure for Sizing Them Up. We obtained permission from the developers to translate Sizing Them Up into Mandarin before conducting further psychological testing. A standard translation procedure was used. In brief, we did a forward translation, a back translation, and reconciliation (Eremenco, Cella, & Arnold, 2005). Two Taiwanese translators who had independently lived and studied in the US for more than 2 years did the forward translation, and the same two translators did the reconciliation with the corresponding author. Afterward, one Taiwanese translator with a master's degree in English literature did the back translation. The developers then examined the back translation and gave instructions to revise the translated Taiwan version of Sizing Them Up. Finally, we produced a developer-approved translated version of Sizing Them Up for parents in Taiwan.
Statistical analysisReliability was analyzed using Cronbach's alpha and McDonald's omega for internal consistency, and test-retest reliability using Pearson correlation. The reason of using Cronbach's alpha is because of its popularity; the reasons of using McDonald's omega is because it has more robust estimates than Cronbach's alpha (Dunn, Baguley, & Brunsden, 2014; McNeish, 2017). Although the recommended value for satisfactory internal consistency is .70 (Chang et al., 2014) and for test-retest reliability is also .70 (Paiva et al., 2014), some believe that an alpha ≥ .60 for internal consistency (Modi & Zeller, 2008) and an r ≥ .30 for test-retest reliability (Cheng et al., 2015) are acceptable, especially for a newly developed instrument like Sizing Them Up. In addition, floor and ceiling effects for Sizing Them Up were calculated as follows: the number of “0” responses divided by all responses (N=236) was the floor effect, and the number of “100” responses divided by all responses was the ceiling effect.
We used three QoL instruments as the criteria for concurrent validity: Sizing Me Up, reported by children who self-rated their QoL, and KINDL and PedsQL, reported by parents who rated their children's QoL. We used Pearson correlations to examine the relationship between the total scores of the three criteria and the scores of Sizing Them Up (including each domain score and the total score). Because a better QoL is indicated by higher scores for all instruments, it is expected to result in positive correlations, and an r>.30 is recommended (Chang et al., 2014).
We did a CFA to test Sizing Them Up's theoretical framework, which consists of six correlated underlying constructs. However, we decided to eliminate some constructs if they did not have adequate reliability or concurrent validity. The data-model fit was examined using seven indices: chi-square, normed chi-square (chi-square/df), the Tucker-Lewis index (TLI), the comparative fit index (CFI), the incremental fit index (IFI), the root mean square error of approximation (RMSEA), and the standardized root mean residual (SRMR). In addition to a nonsignificant chi-square, the acceptable values for the other six fit indices are a normed chi-square<3 (Bollen, 1989; Schweizer, 2010); TLI, CFI, and IFI>.90 (Lin & Tsai, 2015); an RMSEA<.06 (Doostfatemeh, Ayatollahi, & Jafari, 2015); and an SRMR<.08 (Wu, Chang, Chen, Wang, & Lin, 2015).
We used one-way analysis of variance (ANOVA) with a Bonferroni adjustment of the significance level (i.e., we set the significance level at p<.0083 based on 6 comparisons of 4 groups of underweight, normal-weight, overweight, and obese children) to test the known-group validity. We hypothesized that obese children would have the lowest Sizing Them Up scores across all domains and the total score. In addition, Cohen's d was used to assist in the known-group validity.
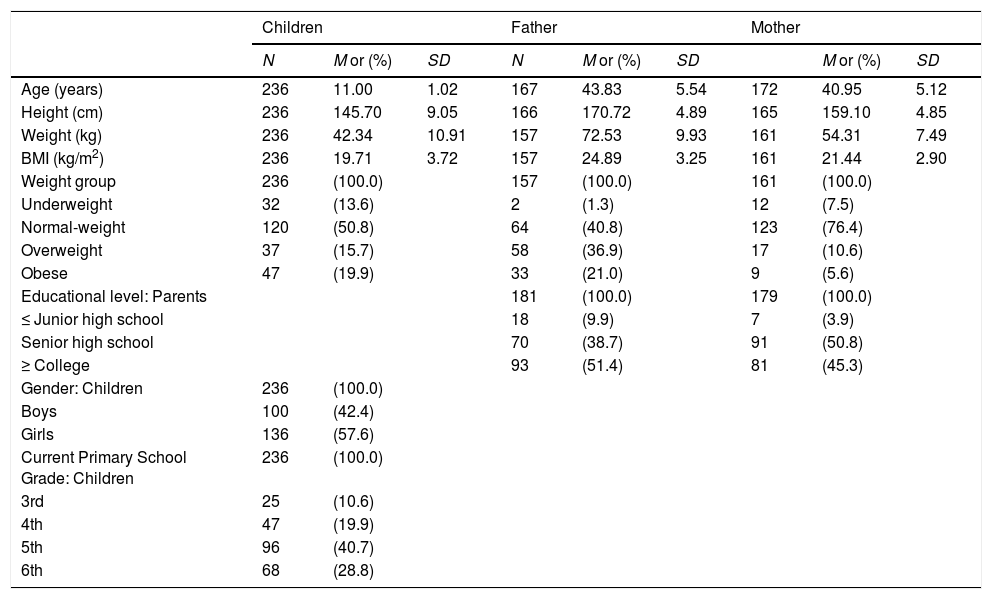
ResultsOf the 236 parents who participated in this study, 53 were fathers, 173 were mothers, and 7 were grandparents. Table 1 presents other demographic information.
Demographic data of children and their parents.
| Children | Father | Mother | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | M or (%) | SD | N | M or (%) | SD | M or (%) | SD | ||
| Age (years) | 236 | 11.00 | 1.02 | 167 | 43.83 | 5.54 | 172 | 40.95 | 5.12 |
| Height (cm) | 236 | 145.70 | 9.05 | 166 | 170.72 | 4.89 | 165 | 159.10 | 4.85 |
| Weight (kg) | 236 | 42.34 | 10.91 | 157 | 72.53 | 9.93 | 161 | 54.31 | 7.49 |
| BMI (kg/m2) | 236 | 19.71 | 3.72 | 157 | 24.89 | 3.25 | 161 | 21.44 | 2.90 |
| Weight group | 236 | (100.0) | 157 | (100.0) | 161 | (100.0) | |||
| Underweight | 32 | (13.6) | 2 | (1.3) | 12 | (7.5) | |||
| Normal-weight | 120 | (50.8) | 64 | (40.8) | 123 | (76.4) | |||
| Overweight | 37 | (15.7) | 58 | (36.9) | 17 | (10.6) | |||
| Obese | 47 | (19.9) | 33 | (21.0) | 9 | (5.6) | |||
| Educational level: Parents | 181 | (100.0) | 179 | (100.0) | |||||
| ≤ Junior high school | 18 | (9.9) | 7 | (3.9) | |||||
| Senior high school | 70 | (38.7) | 91 | (50.8) | |||||
| ≥ College | 93 | (51.4) | 81 | (45.3) | |||||
| Gender: Children | 236 | (100.0) | |||||||
| Boys | 100 | (42.4) | |||||||
| Girls | 136 | (57.6) | |||||||
| Current Primary School Grade: Children | 236 | (100.0) | |||||||
| 3rd | 25 | (10.6) | |||||||
| 4th | 47 | (19.9) | |||||||
| 5th | 96 | (40.7) | |||||||
| 6th | 68 | (28.8) | |||||||
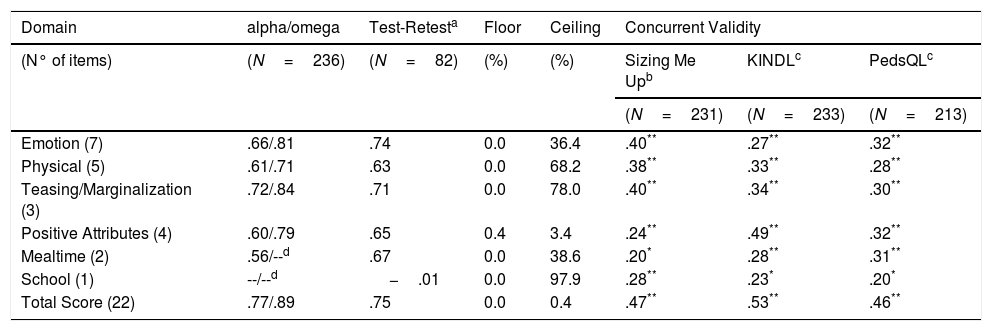
The internal consistency was solid for the Teasing/Marginalization domain score (alpha=.72; omega=.84) and the total score (alpha=.77; omega=.89), nearly acceptable using alpha and acceptable using omega for the Emotion, Physical, and Positive Attributes domain scores (alpha=.60 to .66; omega=.71 to .81), and slightly unsatisfactory for the Mealtime domain score (alpha=.56). However, the test-retest reliability was adequate for all domain scores and the total score (r=.63 to .75), except for the School domain score (r=−.01). All of the domain scores and the total score of Sizing Them Up were moderately correlated with at least one of the criteria scores, except for the School domain score (r=.28 with Sizing Me Up, .23 with the KINDL, and .20 with the PedsQL) (Table 2).
Reliability and concurrent validity of Sizing Them Up (Taiwan version).
| Domain | alpha/omega | Test-Retesta | Floor | Ceiling | Concurrent Validity | ||
|---|---|---|---|---|---|---|---|
| (N° of items) | (N=236) | (N=82) | (%) | (%) | Sizing Me Upb | KINDLc | PedsQLc |
| (N=231) | (N=233) | (N=213) | |||||
| Emotion (7) | .66/.81 | .74 | 0.0 | 36.4 | .40** | .27** | .32** |
| Physical (5) | .61/.71 | .63 | 0.0 | 68.2 | .38** | .33** | .28** |
| Teasing/Marginalization (3) | .72/.84 | .71 | 0.0 | 78.0 | .40** | .34** | .30** |
| Positive Attributes (4) | .60/.79 | .65 | 0.4 | 3.4 | .24** | .49** | .32** |
| Mealtime (2) | .56/--d | .67 | 0.0 | 38.6 | .20* | .28** | .31** |
| School (1) | --/--d | −.01 | 0.0 | 97.9 | .28** | .23* | .20* |
| Total Score (22) | .77/.89 | .75 | 0.0 | 0.4 | .47** | .53** | .46** |
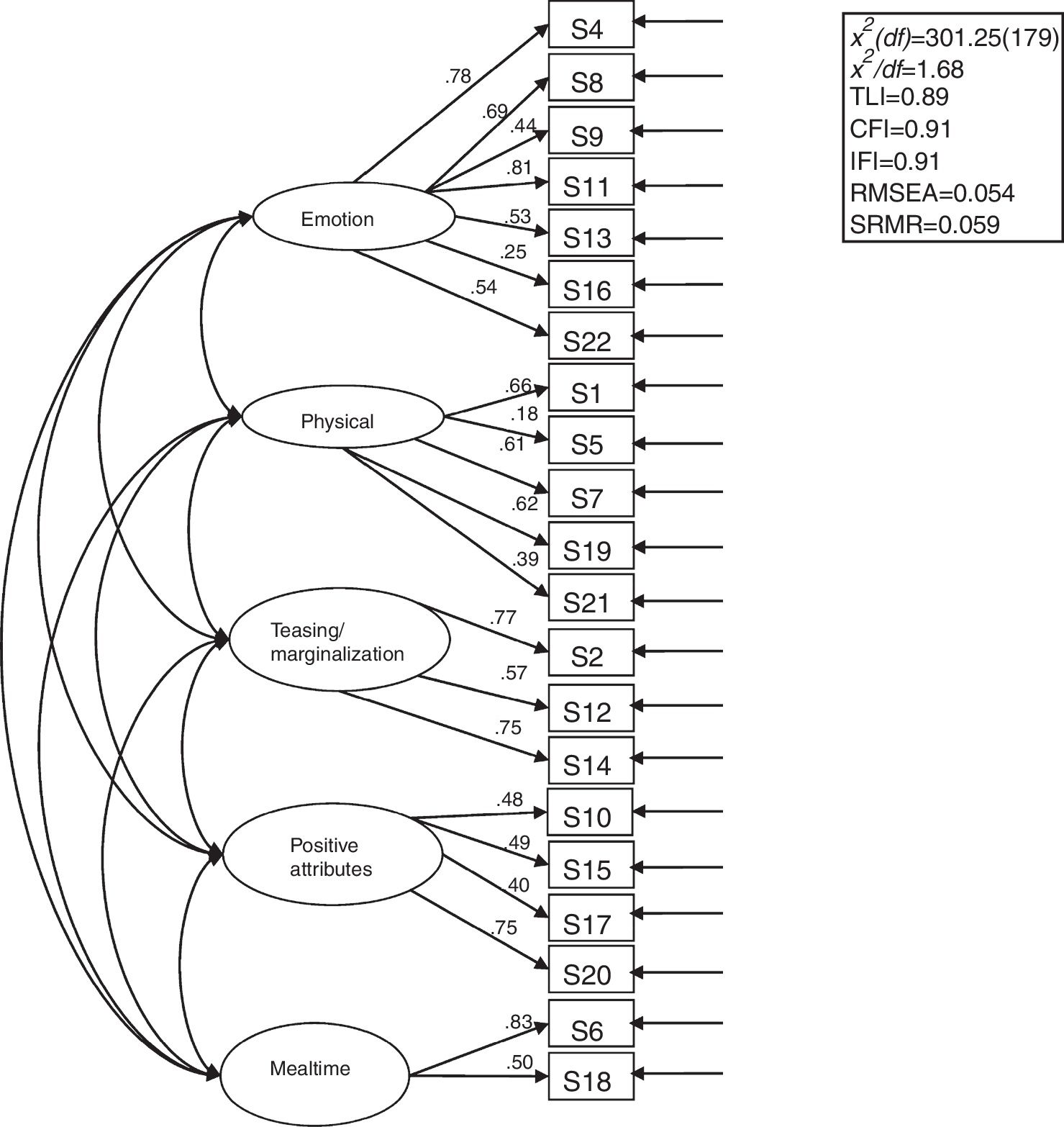
Based on the findings of unsatisfactory psychometric properties for the School domain from Table 2, we decided to remove the only item in the School domain (Chose not to go to school because of their weight/shape/size) from the CFA analysis. Thus, the structure of the CFA model contained five domains with a total of 21 items (Figure 1). Although the chi-square test was significant and indicated a misfit for the structure, all other fit indices were satisfactory or close to acceptable, and suggested a good data-model fit (chi-square/df=1.68, TLI=.89, CFI=.91, IFI=.91, RMSEA=.054, and SRMR=.059).
; df=degree of freedom; TLI=Tucker-Lewis index; CFI=comparative fit index; IFI=incremental fit index; RMSEA=root mean square error of approximation; SRMR=standardized root mean residual. Item S3 was omitted because of its unsatisfactory psychometric properties in Table 2.")
First-order structure of Sizing Them Up with standardized factor loadings (all p-values<.001); df=degree of freedom; TLI=Tucker-Lewis index; CFI=comparative fit index; IFI=incremental fit index; RMSEA=root mean square error of approximation; SRMR=standardized root mean residual. Item S3 was omitted because of its unsatisfactory psychometric properties in Table 2.
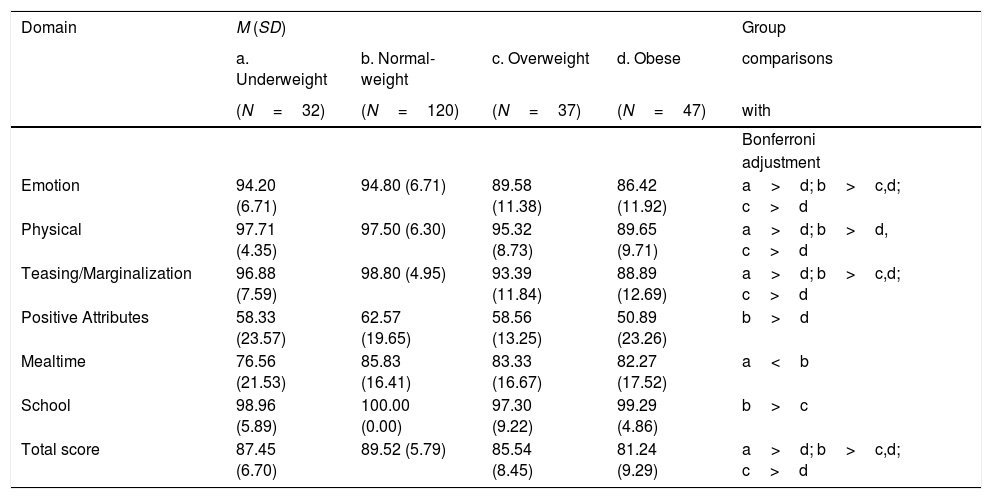
A comparison of all of the domain scores and the total scores of Sizing Them Up between weight statuses to examine the known-group validity showed in Table 3. The total score and the scores in three domains—Emotion, Physical, and Teasing/Marginalization—were significantly lowest for the Obese group (Cohen's d=0.77 [total score], 0.80 [Emotion], 1.07 [Physical], 0.76 [Teasing/Marginalization] as compared with Underweight group;=1.07 [total score], 0.87 [Emotion], 0.96 [Physical], 1.03 [Teasing/Marginalization] as compared with Normal-weight group;=0.48 [total score], 0.27 [Emotion], 0.61 [Physical], 0.37 [Teasing/Marginalization] as compared with Overweight group). The Positive Attributes domain score was also significantly lower in the Obese group than in the Normal-weight group (Cohen's d=0.20). The total score and the scores for the Emotion, Teasing/Marginalization, and School domains were significantly lower for the Overweight group than for the Normal-weight group (Cohen's d=0.55 [total score], 0.56 [Emotion], 0.60 [Teasing/Marginalization]); and scores in the Mealtime domain were significantly lower in the Underweight group than in the Normal-weight group (Cohen's d=0.48).
Known-group validity for Sizing Them Up (Taiwan version).
| Domain | M (SD) | Group | |||
|---|---|---|---|---|---|
| a. Underweight | b. Normal-weight | c. Overweight | d. Obese | comparisons | |
| (N=32) | (N=120) | (N=37) | (N=47) | with | |
| Bonferroni | |||||
| adjustment | |||||
| Emotion | 94.20 (6.71) | 94.80 (6.71) | 89.58 (11.38) | 86.42 (11.92) | a>d; b>c,d; c>d |
| Physical | 97.71 (4.35) | 97.50 (6.30) | 95.32 (8.73) | 89.65 (9.71) | a>d; b>d, c>d |
| Teasing/Marginalization | 96.88 (7.59) | 98.80 (4.95) | 93.39 (11.84) | 88.89 (12.69) | a>d; b>c,d; c>d |
| Positive Attributes | 58.33 (23.57) | 62.57 (19.65) | 58.56 (13.25) | 50.89 (23.26) | b>d |
| Mealtime | 76.56 (21.53) | 85.83 (16.41) | 83.33 (16.67) | 82.27 (17.52) | a<b |
| School | 98.96 (5.89) | 100.00 (0.00) | 97.30 (9.22) | 99.29 (4.86) | b>c |
| Total score | 87.45 (6.70) | 89.52 (5.79) | 85.54 (8.45) | 81.24 (9.29) | a>d; b>c,d; c>d |
The study achieved its aim of filling the research gap in the HRQoL assessment literature by testing the factor structure of Sizing Them Up with a CFA and extending the use of Sizing Them Up from clinically obese children to a community-based sample that also includes overweight and underweight children.
Unlike EFA, which provides the initial factor structure of a newly developed instrument, CFA is based on a theoretically derived technique to test the degree of which data fit a proposed theoretical model (Brown, 2006). After the individual items are forced to load on theoretically derived latent constructs, the total model is estimated by its fit to observed patterns in the data. Using Sizing Them Up with a community-based sample in Taiwan, we found that CFA partially supported the structure of Sizing Them Up proposed by Modi and Zeller (2008). The reason CFA does not fully support that structure is that we removed the School and Adolescent Developmental Adaptation domains from our analyses. However, we believe that these two domains should be removed because: (1) the School domain has only one item and is, therefore, not appropriate for constructing a domain; and (2) we neither recruited nor enrolled any adolescents (≥ 14 years old). We also found that the internal consistency of Sizing Them Up was fairly satisfactory, except for the Mealtime domain, which might be explained by the small number of items in that domain. Moreover, there were high ceiling effects in all domains but Positive Attributes. The lower scale rating on the Positive Attributes modules showed that children's strengths (e.g., humor, success) might be lower than perceived. Therefore, healthcare providers might want to improve the children's perceived strengths.
Sizing Them Up had adequate concurrent validity, test-retest reliability, known-group validity, and construct validity. However, some items had relatively low factor loadings, high ceiling effects, or both; that is, these items might not accurately reflect their underlying constructs. The low factor loading of S5 in the Physical domain (“Had to make changes to surroundings [e.g., furniture, school desks] because of their weight/shape/size”) might be related to cultural differences, because Taiwan has a desk-change policy for children, if needed. That is, primary schools in Taiwan let children sit in the desks that are appropriate for their shape. Therefore, changing surroundings to accommodate children's physical needs was not a problem for our participants. In addition, the unsatisfactory characteristics of item S3 (“Chose not to go to school because of their weight/shape/size”) was represented by high ceiling effects, which indicated that parents in Taiwan did not believe that their children would choose not to go to school because of their weight or size. Moreover, the low factor loading of S16 in the Emotion domain (“Felt concerned about their weight/shape/size”) might also be attributable to different cultural values. Studies (Doolen, Alpert, & Miller, 2009; Lundahl, Kidwell, & Nelson, 2014) report that a prevalent and alarming discrepancy occurs between the actual physical appearance and the parents’ perception of their children's weight. The phenomenon appears to be more evident in Asian culture, in which there is a general belief that, for children, being chubbier is equated with wealth, health, and prosperity (Wong, Sit, Tarrant, & Cheng, 2012). Therefore, their children's body size and weight might not concern Taiwanese parents or provoke their emotional reactions.
Overall, using the total score of Sizing Them Up seemed to yield much better results than did using the individual scores of individual domains or the sum of those individual scores. Furthermore, some items (e.g., S3, S5, and S16) can be omitted for greater reliability in future studies. The alpha of the Emotion domain rose from .66 to .71 after item S16 had been deleted, and the alpha of the Physical domain rose from .61 to .63 after item S5 had been deleted. Nevertheless, the omega values of both domains were satisfactory.
This study has some limitations. Firstly, our participants were apparently healthy; thus, our results might not be generalizable to participants clinically diagnosed with overweight or obesity. Secondly, all of our participants were recruited from the southern Taiwan. Because of this geographical limitation, they might not be representative enough to generalize our findings to the entire population of children in Taiwan. Thirdly, the raters were the children's mothers, fathers, and grandparents, and the equivalence of their perceptions was not clear; in particular, they might have different perspectives about a child's HRQoL because of gender differences (Hubbs-Tait, Kimble, Hingle, Novotny, & Fiese, 2016) or generational gaps (Wardle, Sanderson, Guthrie, Rapoport, & Plomin, 2002). Fourthly, the study had relatively few participants (only slightly>200), but that number fulfilled a minimum requirement for CFA (Su, Ng, Yang, & Lin, 2014).
ConclusionsParents who monitor their children are the most influential people who help their children develop their health. The parents’ perceptions of their children's HRQoL are important because parents are generally the decision-makers about their children's healthcare (Kaartina et al., 2015). Our findings highlight the necessity of raising parental awareness about unhealthy childhood weight and its potential long-term sequelae. If parents, researchers, and healthcare practitioners are interested in measuring parents’ perspectives on the weight-related QoL of children, using the total score of Sizing Them Up is recommended whenever it is used for overweight or underweight children.
FundingThis work was supported in part by (received funding from) the startup fund in the Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong.
