



Human rights are for all, regardless of age. The older adults are seen as vulnerable because biological, psychological and social ageing predispose the ageing person to frailty, infirmity, and in many cases dependency, setting the older person apart from the rest of the population in need of special protection and rights. Although the implementation of legislation, policies, and a package of integrated programmes and projects to cater to the needs of older persons had helped them to uplift their status, more has to be done to stem the increase of the reach of laws in a more fruitful manner.
AimTo develop a colloquial structured Healthcare Policies & Programmes Awareness Questionnaire and assess the awareness about the government healthcare provisions and benefits available for senior citizens among health professionals, older patients, and their caregivers.
MethodsThis study was conducted in two phases, the development of the questionnaire consisting of relevant healthcare national policies and programmes followed by a cross sectional pilot study on 335 participants.
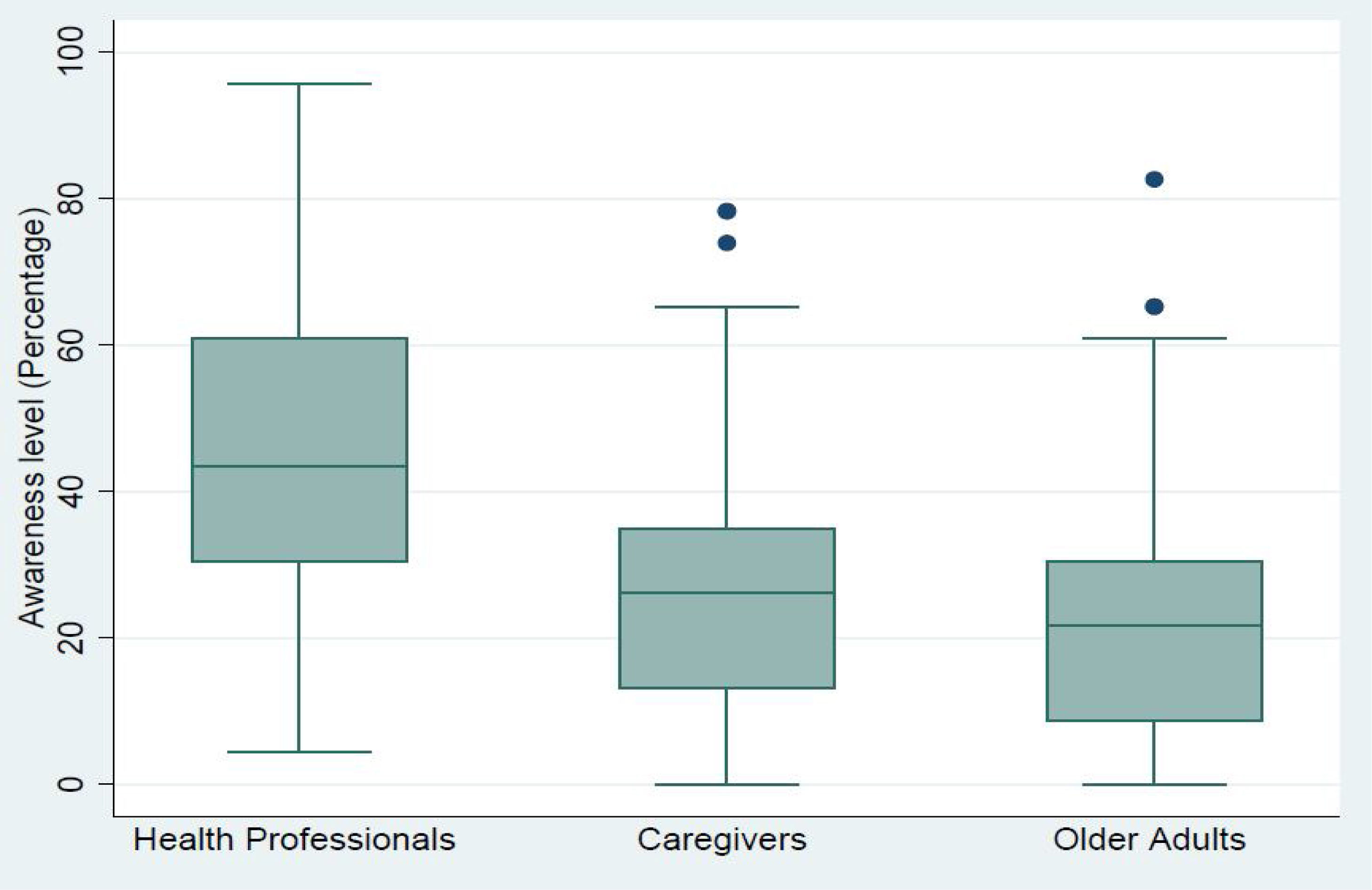
ResultsThe level of awareness was only 45.6% among health professionals followed by 26.4% & 22.2% of awareness among the caregivers and the older adults respectively.
ConclusionThere is a huge gap between the healthcare providers and healthcare takers knowledge due to which the preventive and promotive care of older adults is poor in our country. There is a need to strengthen institutions and mechanism that can more systematically promote interaction between researchers, policymakers and other stakeholders who can influence the uptake of the research findings in a synergistic manner.
Los derechos humanos son para todos, independientemente de la edad. Los mayores son considerados vulnerables, ya que el envejecimiento biológico, psicológico y social predispone a dicha población a fragilidad, enfermedad y en muchos casos dependencia, alejándola del resto de la población, ya que necesitan protección y derechos especiales. Aunque la introducción de medidas legislativas, políticas y una serie de programas y proyectos integrados para satisfacer las necesidades de los mayores ha ayudado a estos a mejorar su estatus, ha de realizarse más para aprovechar el incremento del alcance de la legislación de manera más fructífera.
ObjetivoDesarrollar un cuestionario estructurado sobre concienciación de programas y políticas de atención sanitaria, así como evaluar la concienciación acerca de las disposiciones y beneficios sanitarios del gobierno para los ciudadanos mayores, entre los profesionales sanitarios, los pacientes mayores y sus cuidadores.
MétodosEste estudio fue realizado en dos fases: el desarrollo del cuestionario que incluía políticas y programas nacionales relevantes, seguido de un estudio piloto transversal de 335 participantes.
ResultadosEl nivel de concienciación entre los profesionales sanitarios fue de sólo el 45,6%, del 26,4% entre los cuidadores y del 22,2% entre los mayores, respectivamente.
ConclusiónExiste una gran brecha en cuanto a conocimiento entre los profesionales sanitarios y los receptores de la atención sanitaria, por lo que el cuidado preventivo y promocional de los mayores es malo en nuestro país. Es necesario fortalecer las instituciones y los mecanismos, que puedan promover de manera más sistemática la interacción entre los investigadores, los responsables políticos y demás interesados, quienes pueden influir en la captación de los hallazgos de la investigación, de manera sinérgica.
There is generally low understanding and awareness of the Human Rights Act among older adults and those working with older people. Recently, increasing attention has been paid to the need to promote the human rights of older people as population ageing has become a worldwide concern.1 Older people in industrialized, as well as developing countries, face numerous challenges such as poverty, age-based discrimination, vulnerability to neglect, abuse and violence and a lack of access to adequate health-care and geriatric services.1
This is usually attributed to the fact that older people are especially vulnerable to ill-treatment and human rights abuses in a health and social care context because of their dependency on others for their basic needs. Such a situation is quite prevalent worldwide. However, in India, it is of pressing need, due to the unprecedented rate of growth of this section of the population.1 According to the India Ageing Report 2017, the share of population over the age of 60 is projected to increase from 8 percent in 2015 to 19 percent in 2050. By the end of the century, older adults will constitute nearly 34 percent of the total population in the country. Therefore, relatively young India soon will grow old rapidly in the coming decades. One direct implication of such an increase would be inflated prevalence of chronic disorders. As per the 2012 report of the Population Reference Bureau, it is estimated that nearly 45% of India's disease burden is projected to be borne by older adults in 2030.2 Additionally, an analysis of morbidity patterns by age clearly indicated that the older adults experience a greater burden of ailments due to either social determinant such as feminization, ruralization, caste, education, economic dependency or due to physical or affordability determinants.3 To deal with such misery situation, various national healthcare reforms such as National Policy for older persons4 (NPOP) 1999, National Policy on Senior citizens5 2011, National Programme for Health Care for Elderly6 (NPHCE) 2011, The Integrated Programme for Older Persons7 (IPOP) 2015, Indira Gandhi National Old Age Pension Scheme8 (2011) has taken impetus as these schemes cover major healthcare benefits, including health financing, drug procurement, community participation in health, health management, and physical and financial norms for health and human resources for older persons. Regrettably, the target population and healthcare professionals lack awareness about such reforms. This can be attributed to rampant illiteracy among geriatric population in need at the one end, and lack of knowledge of community services available for the geriatric patients among the healthcare professionals at the other end, thus resulting into the disrupted sender-receiver process.
These national healthcare reforms are important and at times the only means of support for older adults. To assess the impact and steps for further improvement in future policies, it is important to have updated information about the level of awareness and practical problems faced by older adults and health care professionals dealing with them.9 There was many studies9,10 conducted recently to assess the level of awareness about the healthcare schemes, however, none of them developed a structured questionnaire which entails specific information about the exclusive healthcare provisions and benefits available for the senior citizens. Therefore, the current study was conducted to assess the level of awareness about existing healthcare provisions and benefits of available national healthcare policies & programmes for senior citizens and provide them the best of information so that the target stakeholders receive the services they are bound to receive.
MethodologyThis study was conducted in two phases. The first phase involved the development of the Healthcare Policies and Programmes Awareness Questionnaire (HPPAQ). The development process was rigorous and extensive. After the extensive literature review, we followed focused group discussions with stakeholders & experts; followed by precise drafting of questions in colloquial language and finally synthesizing 23 questions in structured open-ended manner with clear meaning. A 23-items questionnaire was prepared, for three groups, older adults (OA), caregivers’ (CG), and healthcare professionals (HP). Questions in the questionnaire explored knowledge about the existing government programmes and policies and its healthcare rights for older adults. The second phase involved surveying among the participants. A total of 335 participants were recruited in the study; 133 were older adults, 101eachwere caregivers’ and healthcare professionals, specifically working with older adults. This study was conducted from June 2018 to July 2019. Statistical analysis was performed using SPSS for Windows 10.1 statistical package. To compare the opinions of two groups, and to examine the hypothesis that the distribution of the variables is independent to each other, the Chi-squared test was used. Significance level (p) less than 0.05 was considered as statistically significant. The study was approved by the institutional Ethics Committee (IEC-321/01.06.2018).
Healthcare programmesThe Ministry of Social Justice & Empowerment4, is the nodal Ministry of Government of India for the overall policy, planning and coordination of programmes for the development of the vulnerable groups. One of the group is senior citizens group. The Ministry focuses on policies and programmes for the Senior Citizens in close collaboration with State governments, Non-Governmental Organizations and civil society. The programmes aim at their welfare and maintenance, especially for indigent senior citizens, by supporting old age homes, day care centres, mobile medicare units, and many social, health and financial welfare policies & programmes. The five major programmes that deal exclusively with older persons’ welfare are summarized as following:
- 1.
The National Policy on Older Persons4 (NPOP): this policy was announced by Government of India in January, 1999. It envisages State support to ensure financial and food security, health care, shelter and other needs of older persons, equitable share in development, protection against abuse and exploitation, and availability of services to improve the quality of their lives. The policy also covers issues like social security, inter-generational bonding, family as the primary caretaker, role of Non-Governmental Organizations, training of manpower, research and training. The primary objectives are:
- •
to encourage individuals to make provision for their own as well as their spouse's old age.
- •
to encourage families to take care of their older family members.
- •
to enable and support voluntary and non-governmental organizations to supplement the care provided by the family.
- •
to provide care and protection to the vulnerable elderly people.
- •
to provide adequate healthcare facility to the elderly;
- •
to promote research and training facilities to train geriatric care givers and organizers of services for the elderly; and
- •
to create awareness regarding elderly persons to help them lead productive and independent live.
- 2.
National Policy on Senior Citizens5 (2011): this policy was updated in November 2011, as a review of NPOP. Considering the changing demographic pattern, socio-economic needs of the senior citizens, social value system and advancement in the field of science and technology. The government review committee made key recommendation including:
- •
Lifelong healthcare facilities for Padma award winners, gallantry award winners.
- •
Setting up of a department of senior citizens and national council for senior citizens.
- •
Increase in old age pension amount.
http://socialjustice.nic.in/writereaddata/UploadFile/dnpsc.pdf
- 3.
National Programme for Health Care of Elderly6 (NPHCE): This programme is a centrally sponsored scheme as an articulation of the international and national commitments of the government as envisaged under (UNCRPD), National Policy on older Persons (NPOP) adopted by the Government of India in 1999 and Section 20 of “The Maintenance and Welfare of Parents and Senior Citizens Act, 2007” dealing with provisional for medical care of senior citizen. The vision of the NPHCE is:
- •
Community based Primary Healthcare approach.
- •
Strengthening of health services for senior citizens at District Hospitals/CHC/PHC/Sub-Centres.
- •
Dedicated facilities at 100 District Hospitals with 10 bedded wards for the elderly;
- •
Strengthening of 8 Regional Medical Institutions to provide dedicated tertiary level Medical Care for the elderly, with 30 bedded wards, at New Delhi (AIIMS), Chennai, Mumbai, Srinagar, Vanarasi, Jodhpur, Thiruvananthapuram and Guwahati; and
- •
Introduction of PG courses in Geriatric Medicines in the above 8 Institutions and In-Service training of health personnel at all level.
- 4.
Integrated Programme for Older Persons7 (IPOP): The Scheme is being implemented since 1992 and was revised in April 2008 and 2015. Financial assistance is provided under it to State Governments/Panchayati Raj Institutions/Urban Local Bodies and Non Governmental Organisations for running and maintenance of projects like- Old Age Home, Day Care Centre; Mobile Medicare Unit; Day Care Centre for Alzheimer's Disease/Dementia Patients; Physiotherapy Clinic for Older Persons; Help-lines and Counselling Centres for Older Persons; Sensitizing Programmes for Children particularly in Schools and Colleges; and providing Regional Resource and Training Centres.
http://www.socialjustice.nic.in/writereaddata/UploadFile/IPOP%202016%20pdf%20document.pdf
- 5.
Indira Gandhi National Old Age Pension Scheme 8 (IGNOAPS): This scheme was introduced as a part of National Social Assistance Programme (NSAP) in June 2011. Under this scheme, all BPL Indians above 60 years are covered. The monthly pension amount for them is Rs.300 for age 60–79 years and 500 above 80 years. This scheme playa vital role in providing financial safety to the elderly to maintain their basic healthcare, social and personal needs.
http://nsap.nic.in/Guidelines/nsap_guidelines_oct2014.pdf
Inclusion criteria (older adults’ respondents)
- (1)
Any older adult aged 60 years or more registered under Department of Geriatric medicine, AIIMS, New Delhi
- (2)
Education: elementary schooling and above
- (3)
Gender: both males and females
- (4)
Language of speech and understanding: Hindi or English
- (5)
Consenting and willing to participate in the study.
Inclusion criteria (Healthcare Professionals)
- (1)
Any medical or paramedical professional working in a hospital set up.
- (2)
Consenting and willingness to participate in the study
Exclusion criteria (older adults’ respondents)
- (1)
Seriously ill patient.
- (2)
Focal neurological features including hemiparesis, sensory loss, and visual field deficits
- (3)
Not consenting and willingness to participate in the study
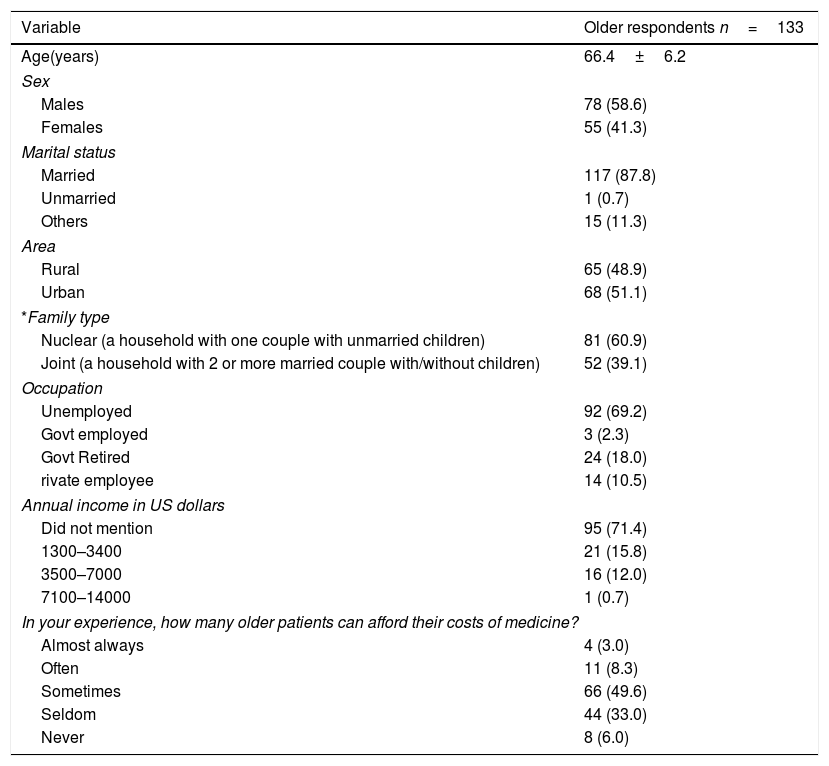
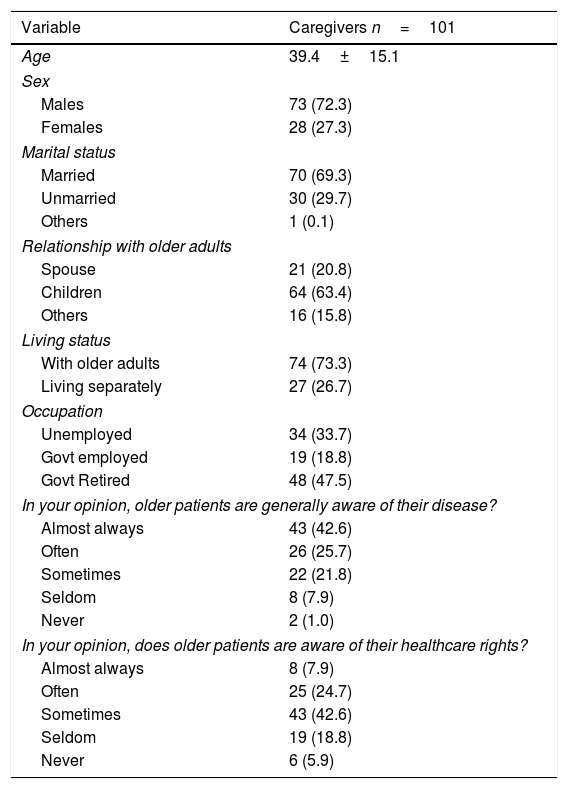
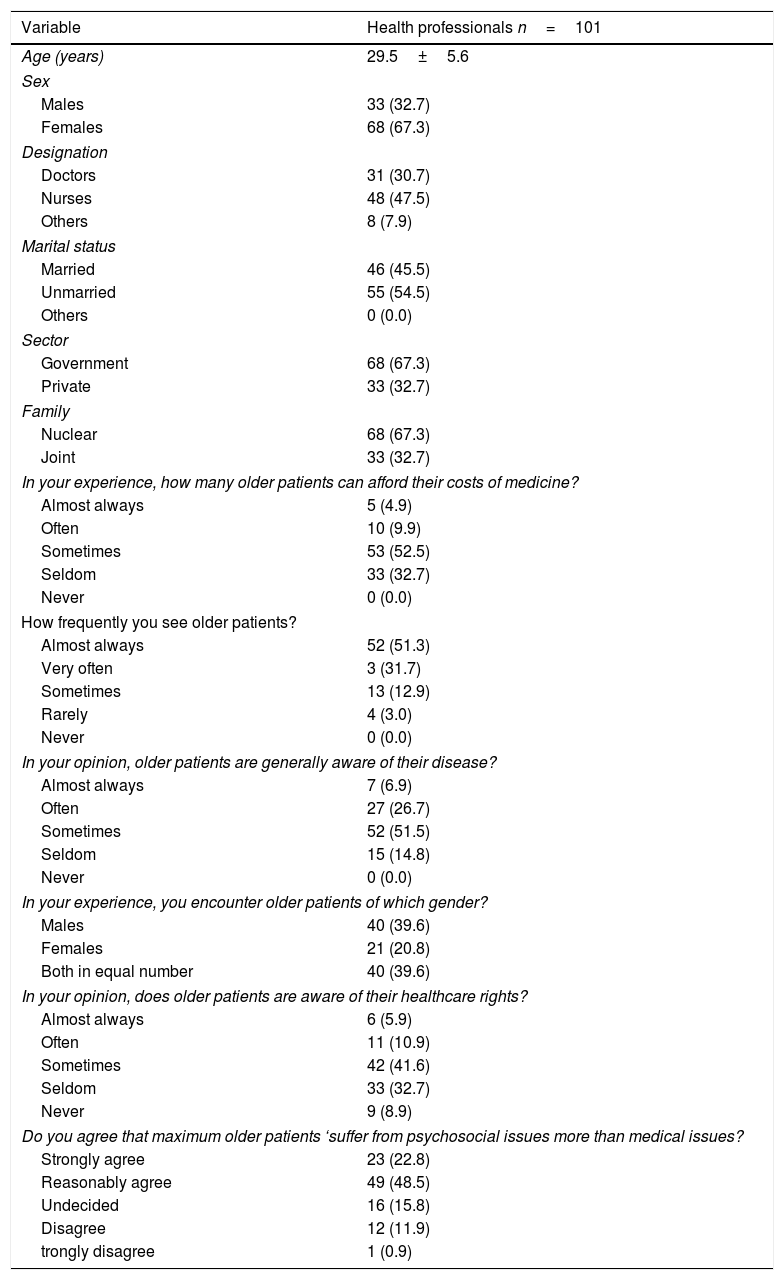
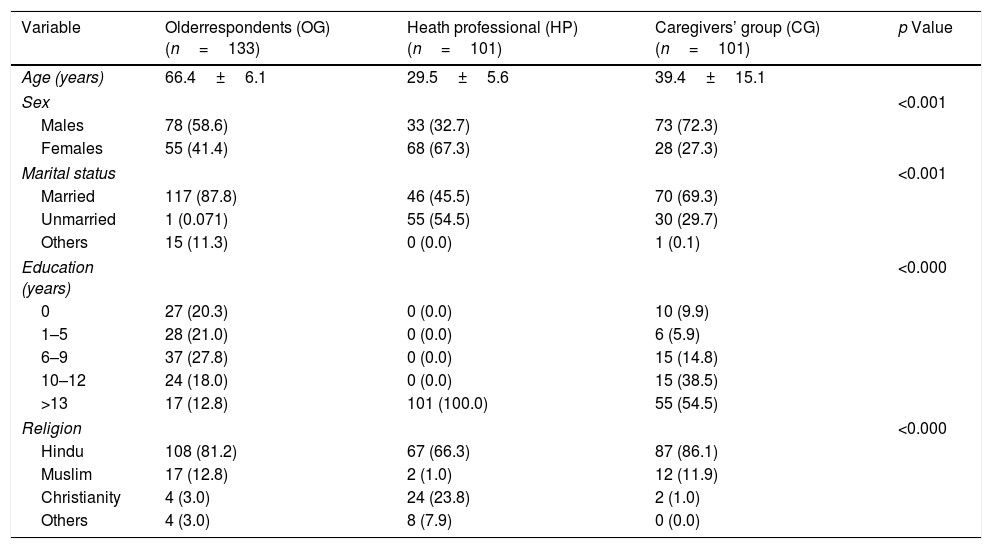
The average age of the older adults was 66.4±6.0; healthcare professionals was 29.5±5.6 years; the caregivers’ 39.4±15.1years (Tables 1–4). The proportion of males was higher in the older adults group and caregivers group respectively (59% vs. 41%; 72% vs. 27%). While in healthcare professional group, females outnumbered the males (67% vs. 33%). The healthcare professionals group consisted of physicians/geriatricians (30.4%), nurses (47.5%), and paramedics (21.8%) (Table 3). According to Table 1, 69% of older adults were unemployed, implying that they have limited financial support which directly affects their healthcare costs. This is supported in our study as well wherein 39% of older adults agree that they cannot afford their costs of medical care. Thus, they look forward to government health setups and senior citizen welfare programmes and schemes which aid in maintaining their healthcare at minimal costs. Another major finding of this study is evident in Table 2, wherein the caregivers’ stated that 60% older adults are aware about their disease, but 25% of them are not aware about their healthcare rights. This can be attributed to two hypothesis- intergenerational consequences or governance/policymakers inefficient implementation planning. As seen in Table 2, 74% caregivers’ are living with their older parents but they are married (70%) and have family, which bifurcate their personal, social and financial responsibilities between their parents and their own family; this consequently lead to feelings of loneliness, negligence, pessimism, isolation, low self-esteem, self-confidence in older adults and thus form a vicious cycle of poor physical, mental and social syndrome. Hence, older adults get so much engrossed in this syndrome, that they become ignorant to the available healthcare welfare schemes and programmes. While another hypothesis could be governance/policymakers inefficient implementation planning. It refers to the lack of promotion of the available healthcare schemes and programmes by the policymakers. It has not been adequately and efficiently promoted at the grass root level wherein the older adults can readily get aware or make use of such schemes independently. Both of these hypothesis can be found to be equally responsible of such poor level of awareness among the older adults and the caregivers.
Health professionals too echo the caregivers’ and older adults’ group opinion. According to Table 3, health professional too reported that although 33% of older adults know about their disease but only 15% can afford the healthcare facility; and 17% are aware about their healthcare rights. This too is found to be consistent with the social and financial dependency issues.
Moreover, as healthcare professional, they reported that 70% of older adults suffer from psychosocial issues than medical issues, a major concern of old age. This can be attributed to many intergenerational factors such as nuclearisation, urbanization, and technology driven life style, which make an older adult vulnerable to many mental and psychological health issues.
1 Descriptive characteristics of older adults group.
| Variable | Older respondents n=133 |
|---|---|
| Age(years) | 66.4±6.2 |
| Sex | |
| Males | 78 (58.6) |
| Females | 55 (41.3) |
| Marital status | |
| Married | 117 (87.8) |
| Unmarried | 1 (0.7) |
| Others | 15 (11.3) |
| Area | |
| Rural | 65 (48.9) |
| Urban | 68 (51.1) |
| *Family type | |
| Nuclear (a household with one couple with unmarried children) | 81 (60.9) |
| Joint (a household with 2 or more married couple with/without children) | 52 (39.1) |
| Occupation | |
| Unemployed | 92 (69.2) |
| Govt employed | 3 (2.3) |
| Govt Retired | 24 (18.0) |
| rivate employee | 14 (10.5) |
| Annual income in US dollars | |
| Did not mention | 95 (71.4) |
| 1300–3400 | 21 (15.8) |
| 3500–7000 | 16 (12.0) |
| 7100–14000 | 1 (0.7) |
| In your experience, how many older patients can afford their costs of medicine? | |
| Almost always | 4 (3.0) |
| Often | 11 (8.3) |
| Sometimes | 66 (49.6) |
| Seldom | 44 (33.0) |
| Never | 8 (6.0) |
Descriptive characteristics of Caregivers group.
| Variable | Caregivers n=101 |
|---|---|
| Age | 39.4±15.1 |
| Sex | |
| Males | 73 (72.3) |
| Females | 28 (27.3) |
| Marital status | |
| Married | 70 (69.3) |
| Unmarried | 30 (29.7) |
| Others | 1 (0.1) |
| Relationship with older adults | |
| Spouse | 21 (20.8) |
| Children | 64 (63.4) |
| Others | 16 (15.8) |
| Living status | |
| With older adults | 74 (73.3) |
| Living separately | 27 (26.7) |
| Occupation | |
| Unemployed | 34 (33.7) |
| Govt employed | 19 (18.8) |
| Govt Retired | 48 (47.5) |
| In your opinion, older patients are generally aware of their disease? | |
| Almost always | 43 (42.6) |
| Often | 26 (25.7) |
| Sometimes | 22 (21.8) |
| Seldom | 8 (7.9) |
| Never | 2 (1.0) |
| In your opinion, does older patients are aware of their healthcare rights? | |
| Almost always | 8 (7.9) |
| Often | 25 (24.7) |
| Sometimes | 43 (42.6) |
| Seldom | 19 (18.8) |
| Never | 6 (5.9) |
Descriptive characteristics of healthcare professionals group.
| Variable | Health professionals n=101 |
|---|---|
| Age (years) | 29.5±5.6 |
| Sex | |
| Males | 33 (32.7) |
| Females | 68 (67.3) |
| Designation | |
| Doctors | 31 (30.7) |
| Nurses | 48 (47.5) |
| Others | 8 (7.9) |
| Marital status | |
| Married | 46 (45.5) |
| Unmarried | 55 (54.5) |
| Others | 0 (0.0) |
| Sector | |
| Government | 68 (67.3) |
| Private | 33 (32.7) |
| Family | |
| Nuclear | 68 (67.3) |
| Joint | 33 (32.7) |
| In your experience, how many older patients can afford their costs of medicine? | |
| Almost always | 5 (4.9) |
| Often | 10 (9.9) |
| Sometimes | 53 (52.5) |
| Seldom | 33 (32.7) |
| Never | 0 (0.0) |
| How frequently you see older patients? | |
| Almost always | 52 (51.3) |
| Very often | 3 (31.7) |
| Sometimes | 13 (12.9) |
| Rarely | 4 (3.0) |
| Never | 0 (0.0) |
| In your opinion, older patients are generally aware of their disease? | |
| Almost always | 7 (6.9) |
| Often | 27 (26.7) |
| Sometimes | 52 (51.5) |
| Seldom | 15 (14.8) |
| Never | 0 (0.0) |
| In your experience, you encounter older patients of which gender? | |
| Males | 40 (39.6) |
| Females | 21 (20.8) |
| Both in equal number | 40 (39.6) |
| In your opinion, does older patients are aware of their healthcare rights? | |
| Almost always | 6 (5.9) |
| Often | 11 (10.9) |
| Sometimes | 42 (41.6) |
| Seldom | 33 (32.7) |
| Never | 9 (8.9) |
| Do you agree that maximum older patients ‘suffer from psychosocial issues more than medical issues? | |
| Strongly agree | 23 (22.8) |
| Reasonably agree | 49 (48.5) |
| Undecided | 16 (15.8) |
| Disagree | 12 (11.9) |
| trongly disagree | 1 (0.9) |
Comparison of the socio-demographic characteristics (mean and standard deviation) among groups (older respondents group, health professional group, and caregivers’ group).
| Variable | Olderrespondents (OG) (n=133) | Heath professional (HP) (n=101) | Caregivers’ group (CG) (n=101) | p Value |
|---|---|---|---|---|
| Age (years) | 66.4±6.1 | 29.5±5.6 | 39.4±15.1 | |
| Sex | <0.001 | |||
| Males | 78 (58.6) | 33 (32.7) | 73 (72.3) | |
| Females | 55 (41.4) | 68 (67.3) | 28 (27.3) | |
| Marital status | <0.001 | |||
| Married | 117 (87.8) | 46 (45.5) | 70 (69.3) | |
| Unmarried | 1 (0.071) | 55 (54.5) | 30 (29.7) | |
| Others | 15 (11.3) | 0 (0.0) | 1 (0.1) | |
| Education (years) | <0.000 | |||
| 0 | 27 (20.3) | 0 (0.0) | 10 (9.9) | |
| 1–5 | 28 (21.0) | 0 (0.0) | 6 (5.9) | |
| 6–9 | 37 (27.8) | 0 (0.0) | 15 (14.8) | |
| 10–12 | 24 (18.0) | 0 (0.0) | 15 (38.5) | |
| >13 | 17 (12.8) | 101 (100.0) | 55 (54.5) | |
| Religion | <0.000 | |||
| Hindu | 108 (81.2) | 67 (66.3) | 87 (86.1) | |
| Muslim | 17 (12.8) | 2 (1.0) | 12 (11.9) | |
| Christianity | 4 (3.0) | 24 (23.8) | 2 (1.0) | |
| Others | 4 (3.0) | 8 (7.9) | 0 (0.0) | |

The older adults represent a highly significant group of users of the health care system, and their care has a major impact on health care costs. Additionally, being a regular consumer of medical services is a significant part of daily life for many older adults around the globe.11 As the “third age” has been extended through longer average life-spans, so too are older persons living with more chronic and acute health problems and relying on care through the health system to maintain functioning and prolong life.12 However, the disease burden among Indian older adults places unique demands on the country's public healthcare system.13 It ranges from many personal, social and cultural barriers such as family nuclearisation, financial dependency, the salience of pre-existing inequities on the axes of gender, education, caste, and religion and many more. Therefore, the older adults get entangled in such barriers and lack awareness about the available healthcare benefits.
Such finding was found to be evident in the present study as well. Majority of the older adults were unemployed (69.2%) males (58.6%), and was living in a nuclear family (60.9%) (Table 1). In the present study, males, in general were more aware of their rights (58.6%) than females (Table 4). This finding was comparable with other national14 and international15 studies. Besides this, financial and social dependency plays a pivotal role in the accessibility of healthcare rights. Majority of older adults (71.4%) did not mention about their annual income which could be attributed to social stigma. According to the last published study16 on financial status of older adults in India, the average yearly income is approximately about $1600 which is not adequate to maintain basic healthcare facilities. Thus, financial status is a major factor impacting the accessibility of healthcare facilities by older adults. At awareness level, 48.5% older adults were aware of government social & healthcare schemes; more than half (82%) were from nuclear family and nearly 92% were below the poverty line. The present findings are consistent with the past studies as well.17
Furthermore, a larger proportion of the healthcare professionals (45.6%) in comparison to the older adults (26.4%) and their caregivers (22.2%) have more awareness about the government healthcare provisions (Fig. 1). However, the percentage of awareness was still very low. This could be because there is an alarming dearth of adequately prepared geriatricians, nurses, social workers, researchers, and public health professionals, and poor course curriculum. This is consistent with the international literature as well.18 Although the unique needs of older adults and valued geriatric coverage has been recognized globally, lack of geriatrics-trained educators, shortage of time in packed curricula and low student demand (due to limited exposure to older adults and gerontological stereotyping) still exist as barriers to improving geriatric healthcare training.19 Further, this limited geriatric didactic content is congruent with findings from a survey of nurse practitioners as well in which the majority of the respondents reported that they were only somewhat comfortable caring for older adults; however, they have limited knowledge taught about existing healthcare policies and programmes in their course curriculum.20 Overall, it is the lack of synergistic relationship among the policymakers, educators, and the healthcare professionals which implicate such low awareness about the existing healthcare provisions for older adults.21
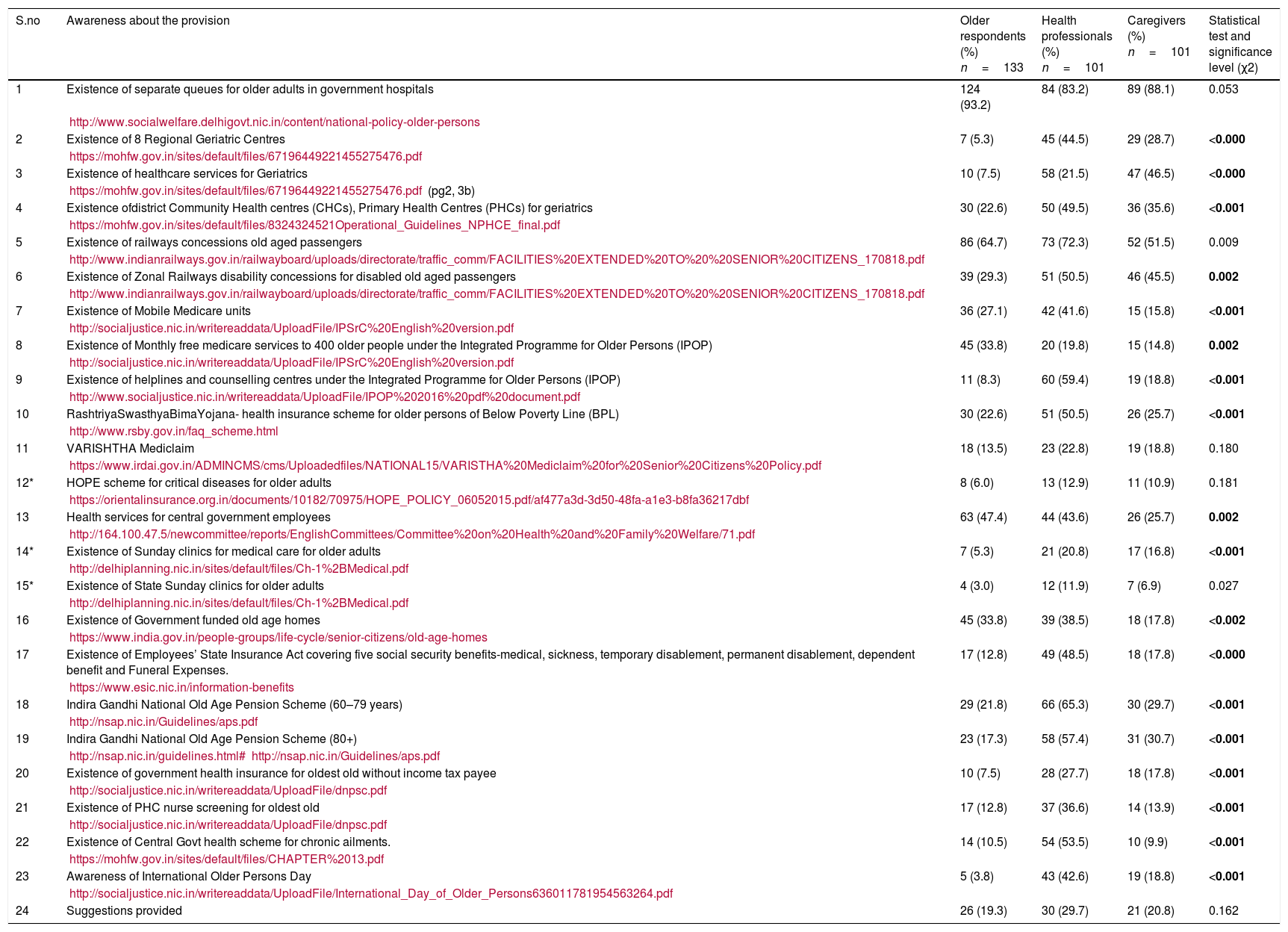
Additionally, the study findings suggest that out of 23 provisions, three most aware provisions were number 1, 5 and 18 among health care professionals (Table 5). This includes awareness about existence of separate queues for older adults in government hospitals (83.2%), the existence of railway concessions for older adults (72.3%), and Indira Gandhi National Old Age Pension Scheme (IGNOPAS) (65.3%). In contrast, the least three aware provisions were, 15, 12 and 8 (Table 5). It covers the existence of Sunday Clinics service for older adults (11.9%), followed by Health of Privileged Elder (HOPE) scheme for hospitalization expenses coverage(12.9%) and availability of Medicare Unit for older adults at rural places (19.8%).
Awareness about each healthcare provision among older respondents, health professionals, and caregivers’ group.
| S.no | Awareness about the provision | Older respondents (%) n=133 | Health professionals (%) n=101 | Caregivers (%) n=101 | Statistical test and significance level (χ2) |
|---|---|---|---|---|---|
| 1 | Existence of separate queues for older adults in government hospitals | 124 (93.2) | 84 (83.2) | 89 (88.1) | 0.053 |
| http://www.socialwelfare.delhigovt.nic.in/content/national-policy-older-persons | |||||
| 2 | Existence of 8 Regional Geriatric Centres | 7 (5.3) | 45 (44.5) | 29 (28.7) | <0.000 |
| https://mohfw.gov.in/sites/default/files/67196449221455275476.pdf | |||||
| 3 | Existence of healthcare services for Geriatrics | 10 (7.5) | 58 (21.5) | 47 (46.5) | <0.000 |
| https://mohfw.gov.in/sites/default/files/67196449221455275476.pdf (pg2, 3b) | |||||
| 4 | Existence ofdistrict Community Health centres (CHCs), Primary Health Centres (PHCs) for geriatrics | 30 (22.6) | 50 (49.5) | 36 (35.6) | <0.001 |
| https://mohfw.gov.in/sites/default/files/8324324521Operational_Guidelines_NPHCE_final.pdf | |||||
| 5 | Existence of railways concessions old aged passengers | 86 (64.7) | 73 (72.3) | 52 (51.5) | 0.009 |
| http://www.indianrailways.gov.in/railwayboard/uploads/directorate/traffic_comm/FACILITIES%20EXTENDED%20TO%20%20SENIOR%20CITIZENS_170818.pdf | |||||
| 6 | Existence of Zonal Railways disability concessions for disabled old aged passengers | 39 (29.3) | 51 (50.5) | 46 (45.5) | 0.002 |
| http://www.indianrailways.gov.in/railwayboard/uploads/directorate/traffic_comm/FACILITIES%20EXTENDED%20TO%20%20SENIOR%20CITIZENS_170818.pdf | |||||
| 7 | Existence of Mobile Medicare units | 36 (27.1) | 42 (41.6) | 15 (15.8) | <0.001 |
| http://socialjustice.nic.in/writereaddata/UploadFile/IPSrC%20English%20version.pdf | |||||
| 8 | Existence of Monthly free medicare services to 400 older people under the Integrated Programme for Older Persons (IPOP) | 45 (33.8) | 20 (19.8) | 15 (14.8) | 0.002 |
| http://socialjustice.nic.in/writereaddata/UploadFile/IPSrC%20English%20version.pdf | |||||
| 9 | Existence of helplines and counselling centres under the Integrated Programme for Older Persons (IPOP) | 11 (8.3) | 60 (59.4) | 19 (18.8) | <0.001 |
| http://www.socialjustice.nic.in/writereaddata/UploadFile/IPOP%202016%20pdf%20document.pdf | |||||
| 10 | RashtriyaSwasthyaBimaYojana- health insurance scheme for older persons of Below Poverty Line (BPL) | 30 (22.6) | 51 (50.5) | 26 (25.7) | <0.001 |
| http://www.rsby.gov.in/faq_scheme.html | |||||
| 11 | VARISHTHA Mediclaim | 18 (13.5) | 23 (22.8) | 19 (18.8) | 0.180 |
| https://www.irdai.gov.in/ADMINCMS/cms/Uploadedfiles/NATIONAL15/VARISTHA%20Mediclaim%20for%20Senior%20Citizens%20Policy.pdf | |||||
| 12* | HOPE scheme for critical diseases for older adults | 8 (6.0) | 13 (12.9) | 11 (10.9) | 0.181 |
| https://orientalinsurance.org.in/documents/10182/70975/HOPE_POLICY_06052015.pdf/af477a3d-3d50-48fa-a1e3-b8fa36217dbf | |||||
| 13 | Health services for central government employees | 63 (47.4) | 44 (43.6) | 26 (25.7) | 0.002 |
| http://164.100.47.5/newcommittee/reports/EnglishCommittees/Committee%20on%20Health%20and%20Family%20Welfare/71.pdf | |||||
| 14* | Existence of Sunday clinics for medical care for older adults | 7 (5.3) | 21 (20.8) | 17 (16.8) | <0.001 |
| http://delhiplanning.nic.in/sites/default/files/Ch-1%2BMedical.pdf | |||||
| 15* | Existence of State Sunday clinics for older adults | 4 (3.0) | 12 (11.9) | 7 (6.9) | 0.027 |
| http://delhiplanning.nic.in/sites/default/files/Ch-1%2BMedical.pdf | |||||
| 16 | Existence of Government funded old age homes | 45 (33.8) | 39 (38.5) | 18 (17.8) | <0.002 |
| https://www.india.gov.in/people-groups/life-cycle/senior-citizens/old-age-homes | |||||
| 17 | Existence of Employees’ State Insurance Act covering five social security benefits-medical, sickness, temporary disablement, permanent disablement, dependent benefit and Funeral Expenses. | 17 (12.8) | 49 (48.5) | 18 (17.8) | <0.000 |
| https://www.esic.nic.in/information-benefits | |||||
| 18 | Indira Gandhi National Old Age Pension Scheme (60–79 years) | 29 (21.8) | 66 (65.3) | 30 (29.7) | <0.001 |
| http://nsap.nic.in/Guidelines/aps.pdf | |||||
| 19 | Indira Gandhi National Old Age Pension Scheme (80+) | 23 (17.3) | 58 (57.4) | 31 (30.7) | <0.001 |
| http://nsap.nic.in/guidelines.html#http://nsap.nic.in/Guidelines/aps.pdf | |||||
| 20 | Existence of government health insurance for oldest old without income tax payee | 10 (7.5) | 28 (27.7) | 18 (17.8) | <0.001 |
| http://socialjustice.nic.in/writereaddata/UploadFile/dnpsc.pdf | |||||
| 21 | Existence of PHC nurse screening for oldest old | 17 (12.8) | 37 (36.6) | 14 (13.9) | <0.001 |
| http://socialjustice.nic.in/writereaddata/UploadFile/dnpsc.pdf | |||||
| 22 | Existence of Central Govt health scheme for chronic ailments. | 14 (10.5) | 54 (53.5) | 10 (9.9) | <0.001 |
| https://mohfw.gov.in/sites/default/files/CHAPTER%2013.pdf | |||||
| 23 | Awareness of International Older Persons Day | 5 (3.8) | 43 (42.6) | 19 (18.8) | <0.001 |
| http://socialjustice.nic.in/writereaddata/UploadFile/International_Day_of_Older_Persons636011781954563264.pdf | |||||
| 24 | Suggestions provided | 26 (19.3) | 30 (29.7) | 21 (20.8) | 0.162 |
Among the older adults and caregivers’ group as well, three major provisions they were aware was number 1, 5 and 13. This includes the existence of separate queues for older adults in government hospitals (93.2% and 88.1%), existence of railway concessions for older adults (64.7% and 51.5%), and entitlement of health services to central government employees (47.4% and 25.7%) respectively.
Similar results were seen in another cross-sectional study,9 where a pre-tested, semi-structured schedule was used to assess the awareness about Indira Gandhi National Old Age Pension Scheme (IGNOAPS). The findings indicated that the majority of the sample (79.4%) was aware of the scheme; however, only 50.2% were utilizing the scheme. Such reduced utilization was attributed to tedious administrative formalities as a major barrier.
Another observational cross sectional study22 too focused on assessing awareness of Indira Gandhi National Old Age Pension Scheme. The findings indicated that 74.6% were aware of the scheme and only 45.4% utilized it. The proportion of elderly who were aware of concession in railway ticket and higher interest rates on deposits in Bank/Post office respectively was 34.9% and 32.9%. The utilization rate was however abysmally low with 27.8% utilizing railway ticket concession and 10.1% depositing money to get higher interest in Bank/Post office. Less than 1% elderly utilized income tax benefits. The authors concluded that there is an urgent need to review the existing policy guidelines and amend them to suit and benefit the elderly.
Such a trend of awareness shows that National Policy on Older Persons4 1999 was among the most aware scheme. The policy provides broad guidelines to State Governments to ensure the well-being of senior citizens and improve quality of their lives through providing specific facilities, concessions, relief, services, etc., and helping them cope with problems associated with old age. It provides a comprehensive picture of various facilities and covers many areas of financial and health care security.
Healthcare and social aegis reforms are a safeguard mechanism, which a society extends to its fellow members to warrant income security and attainability of the welfare services, especially for the vulnerable sections of the society such as senior citizen groups. However, many past studies have shown that such section of the population lacks awareness about such schemes. According to the latest study,16 only 48.5% of older adults were aware of government social & healthcare schemes. This study also states that major challenge faced in the utilization of schemes was mainly due to lack of awareness, only 40.9% of elderly people were unaware of such schemes. This shows a lack of effective promotion of such policies and programmes on part of the healthcare sector.
Thus, the current study and the existing national research mentioned above demonstrate that older adults are poorly aware of their government geriatric healthcare welfare services. It could be inferred that the benefits of various schemes and entitlements to the older adults are not publicized adequately and proper strategies to reach out to them have not been conceived. Such studies eventually help in creating amendments in improving the policy and programme more visible among the targeted beneficiaries and the healthcare providers. For an example, under NPHCE scheme, the latest dementia awareness through Memory Clinics, and management booklets improved among older adults. Although individual rights are universal, the mechanism of their implementation varies between countries. Universally, however, the strategy development to promote older adults’ rights has to be carefully prepared, to ensure that the intention is translated into effective and practical action, which commands the support of all stakeholders involved. Hence, as a future implementation, we are preparing welfare schemes pictorial guide for older adults so that they can easily avail the healthcare welfare services, we have started counselling guidance rooms at dedicated geriatric medicine department of our institute, we have added seminars in course curriculum of geriatric medicine post graduates to improve their awareness level about the current schemes and programmes; further step is been taken to spread the course of action to other 12 regional geriatric centres as well to enhance the geriatric services awareness nationally and improve the national older adult well being at all levels.
ConclusionThese results indicate that healthcare professionals are not fully aware of the existing healthcare rights of older adults. This can be attributed to lack of knowledge and assertiveness in the older respondents they serve. The study concludes that effective measures should be taken to improve the overall awareness not only among older adults but also among different stakeholders in the healthcare delivery system. Continuing medical, paramedical, and nursing education should focus on patients’ rights, particularly, older adults and its importance, its need for awareness and its consequences should be taught to students and hospital staff. Brief short brochures and pamphlets in simple language about the rights and responsibilities of the older adults and their caregivers should be provided to them at the hospitals during their admission and discharge with due attention to the rural and illiterate population using pictorial messages and using appropriate translations of the local language. A system should be in place including the establishment of senior citizens Rights Committee in the hospital for supervision, monitoring, and observance of their rights.
Conflict of interestsThe authors declare no conflict of interest.
This study was carried out in department of Geriatric Medicine, All India Institute of Medical Sciences, New Delhi. It is a departmental study where no funding was involved from any funding agency. A special acknowledgement to National Programme for Healthcare for Elderly Ministry of Health and Family Welfare, Government of India for supporting the concept of the study.

