



Leadership communicates purpose and innovative ways to thrive for performance. Leadership support influences and impacts operational excellence in the health sector as a patient-centered operation, with effective management, excellence framework, challenges and constraints, teamwork and value stream mapping. It is hypothesized that: (1) perceived leadership support will positively correlate with perceived operational excellence (Patient-centered Operations, Effective Resource Management, Excellence framework, Eliminating Challenges or Constraints, Team Work, Value Stream Mapping) and (2) the correlation would be highest with Patient-centered Operations. The aim of this study was to examine the relationship between leadership support and operational excellence in the health care sector among a selected group of healthcare managers.
Materials and methodA correlation study between leadership support and operational excellence was designed for a group of health care managers (n=80) from eight hospitals in Kerala, South India. The selection of executives was from NABH accredited hospitals from districts with a minimum of four NABH accredited hospital. A survey was sent to a selected study sample. The respondents were cooperative and provided responses on perceived leadership support for operational excellence.
ResultsFactors of leadership support correlated to operational excellence.
ConclusionIn the health care sector, leadership support for patient-centered operations helps achieve operational excellence.
El liderazgo expresa objetivo y modos innovadores de desarrollo del desempeño. El soporte al liderazgo influye y tiene un impacto en la excelencia operativa en el sector sanitario como operación centrada en el paciente, con gestión efectiva, marco de excelencia, retos y dificultades, equipo de trabajo y análisis rápido del flujo de valor. Se supone que: (1) el respaldo al liderazgo percibido se correlacionará positivamente con la excelencia operativa percibida (operaciones centradas en el paciente, gestión de recursos efectiva, marco de excelencia, eliminación de retos o dificultades, trabajo en equipo, análisis rápido del flujo de valor-value stream mapping) y (2) la correlación será más alta con las operaciones centradas en el paciente. El objetivo de este estudio fue examinar la relación entre el respaldo al liderazgo y la excelencia operativa en el sector sanitario, entre un grupo seleccionado de gestores sanitarios.
Materiales y métodoSe diseñó un estudio de correlación entre respaldo al liderazgo y excelencia operativa para un grupo de gestores sanitarios (n=80) de 8 hospitales en Kerala, en el sur de India. La selección de los ejecutivos procedía de los hospitales acreditados NABH, de aquellos distritos con un mínimo de 4 hospitales acreditados NABH. Se envió una encuesta a una muestra de estudio seleccionada. Los respondedores fueron cooperadores, y aportaron respuestas sobre el respaldo al liderazgo percibido para la excelencia operativa.
ResultadosLos factores de respaldo al liderazgo se correlacionaron con la excelencia operativa.
ConclusiónEn el sector de la atención sanitaria, el respaldo al liderazgo para operaciones centradas en el paciente logra la excelencia operativa.
Leadership must strive to develop build and maintain successful competencies among employees. The knowledge, skills and abilities a leader possess and exhibits along with leadership capabilities of motivation, influence, power, interpersonal relationships, communication and inspiration are crucial factors. In the health care settings, competencies that are relevant to individual roles needs to be developed to do more with less available and skills are to developed to increase professionalism and health education.
Health Care Sector is a complex as well as dynamic environment with leaders from different spheres, specialties and education. In health care, leaders need to continuously breed, change and inspire the employees to use their full potential at all times. Bloom's theory speaks about three types of learning categories namely cognitive (knowledge and mental abilities), affective (attitude, feelings, emotions), psychomotor (physical skills); which is commonly referred to as knowledge, skills and attitude. These help in instructional activities as and when employees face difficulty in progress. Often leaders use motivation to influence employee actions. Traditional leadership of power and aggression has emerged into motivation and inspiration, the theory of affiliation by Schutz states that individuals have three types of need, inclusion need, control need and affection need. A strong organizational culture emerges when a leader subjects the subordinates with these needs. Groups passing through inclusion, control and affection is cyclical and is observable.1 A powerful organizational culture is formed on the balance of inclusion of needs of his subordinates by a leader inclusive of his or her needs for control and affection.2 The self-determination theory3 assists in the human facets of motivation, personality and wellbeing and factors that promote these facets. This theory is based on the fact that humans have three basic needs of autonomy, competence and relatedness.4 Whilst relatedness is relying and respecting others, competence is the ability to take on to complete challenging tasks and autonomy is the choice of own behavior.4 In an organization, the support for these aspects by leadership are very important to promote self-motivation and wellbeing.3 Autonomy is possible only when leadership encourages participatory planning and decision making and also promotes motivation through rewards and recognition (Ledlow and Coppola, 2014); but the onus is on the leaders to ensure that individual and subgroup goals are in sync with organizational goals (Locke and Chesney, 1991).
In health care sector, building interpersonal relation is less easy and important to manage conflict, team building, networking, supporting and mentoring to strengthen relationships (Yukl, 1989). Also in health care sector time is very crucial and most often leadership communication is vocal, thus excellent communication skills are mandatory. Descriptive communication, problem orientation, strategic and spontaneous communication, equality rather than superiority in communication; flexible, open, and genuine thinking supports an excellent organizational climate.1
Health care sector requires vital link between clinical and administrative departments and thus Planning is crucial, especially the operational processes (Granda-Cameron et al., 2007). Yukl5 stated that planning is a process using micro and macro factors, wherein strategic planning is finding the best possible plans for excellence; operational planning is to find the best processes for excellence through resources, processes, systems and methods. Rakich et al. (1992) established the environmental scanning related to the macro and micro forces; macro dealing with the legal, political, cultural, public expectations, economic and ecological forces whilst micro also known as health care environmental forces that includes planning, public policy, competitive forces, financing in health care, technology, research, public health and integration with health disciplines. Decision making needs has to be sensitized to organizational systems through evaluation, information, standardization of documents, time frame, urgency, and training subordinates or group members for the process of decision making (Ledlow and Coppola, 2014). Quality improvement is an ongoing process in health care sector. Leadership, decision making, identification of improvement areas, assessment of situations, gathering information, planning and implementation, feedback are the key factors of quality improvement (Ledlow and Coppola, 2014). These if constantly practiced will form the culture of the organization for operational excellence. The Deming's Total Quality Management (TQM) principles with a 14 step process of constant strive to improve, total quality philosophy adoption, will help leaders to create a culture of continuous quality improvement. Training is another integral factor leaders has to focus on since resource development is possible only through training. Performance is based on upskilling and learning. However, most training fail to look at the Kirkpatrick training evaluation model of reaction, learning, behaviors and results and also the revision by James and Wendy (2016) to include relevancy of everyday jobs in training with regard to continuing health education involving activities, events, and efforts resulting in recognized and unrecognized knowledge (Ledlow and Coppola, 2014). Critical thinking for leaders evolve through empirical thinking and evaluative thinking. Thus leadership development has to be a part of the learning culture.
Health Sector is a contingent organization and totally resource dependent. Therefore leaders have to be aware of all providers, beneficiaries, referrals, and practices (Ledlow and Coppola, 2014). Leaders who try to maintain operations often fail to achieve economies of scale. Schein (1993) wrote that culture and its essence is driven by the learned, shared tacit assumptions on which people base their daily behaviors. Schein (1985) suggested that organizational climate is the pattern of basic assumptions that a group invents and deals with the challenges taught to new employees to perceive. Schein suggested that the invisible artifacts of visible patterns and the climate form the values and assumption levels. Leaders in Health sector should be wary of the day to day challenges to change the health organization culture.6 Leadership gap for operational excellence has to be filled through understanding the ultimate decisions through ethics and spirituality since it has to be patient centered whether it is survival or end-of-life decisions. Health Executives constantly face such issues and complex decision making aspects and leaders need to have an understanding about patients from different background and culture and sensitivity. Thus a positive correlation between leadership support and operational excellence was expected and that the patient centered operations will have a highest correlation.
Operations effectiveness has to be both efficient and optimal which is an amalgamation of degree of qualitative and quantitative factors based on outcome variables and outcome measures (Coppola, 2013). Performance in the health sector for patient centered operations has to be based on efficiency ratios and effectiveness criteria (Coppola, 2013). To avoid maleficence and produce efficacy, organizations should maintain, restore and improve health and provide required patient care (Ledlow and Coppola, 2014). Leadership in health care has different roles of that of a physician leader, nurse leader, administrative leader, department heads, medical functionality leader, operations leader, quality assurance leader, paramedics leader etc. The parity of Health care model speaks about the Iron triangle of cost, access and quality (Ledlow and Coppola, 2014). The word patient is from the Latin word meaning suffer and is to explain the people who receive care. Health Leaders need to understand patients since they pay for the access and quality (Smeltzer and Bare, 2004) and is supposed to give managed care. Leadership in power has to dissipate power to empower the subordinates. Health leaders who are transformational, can change and influence behaviors, attitudes, beliefs and values in the health care sector.
Therefore, based on these premises, the correlation of leadership factor with patient centeredness was expected to be positive and highest. The aim of this study was to examine the relationship between leadership support and operational excellence in the health care sector among a selected group of healthcare managers.
MethodThe hypotheses tested were as below:H1 Operational excellence (Patient Centered Operations, Effective Resource Management, Excellence framework, Eliminating Challenges or Constraints, Team Work, Value Stream Mapping) and the perceived leadership support for operational excellence will be positively correlated. The relationship between patient centered operations as a factor of leadership support will be strongest for operational excellence.
A selection of 80 Health care managers (or so called as Executives in the health care sector) in South India (Kerala) were surveyed. The selection of this group of executives was from NABH accredited hospitals from districts with a minimum of four NABH accredited hospital. The hospitals were selected from the capital city and commercial city. The mean age of the respondents was 31.1 years-old (standard deviation of 6.42) and the mean experience level was 10.43 years-old (standard deviation of 8.51). The respondents were cooperative and provided responses on the perceived leadership support for operational excellence.
Statistical analysisA bivariate correlations among each factors of leadership support with the perceived operational excellence has been used. Scoring of measures were such that high score will indicate that more leadership support for operational excellence. A positive correlation has been considered a support for the proposed hypothesis (leadership support increases according to operational excellence). As an ad hoc methodology, for Scoring used a Likert scale grading from 1 representing strongly disagree to 4 representing strongly agree.
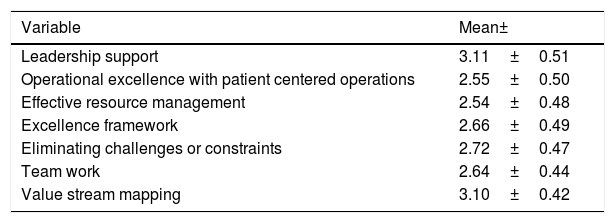
ResultsThe values of mean and standard deviation is given in Table 1. The correlation between leadership support and perceived operational excellence are given in Table 2
Characteristics of study sample.
| Variable | Mean± |
|---|---|
| Leadership support | 3.11±0.51 |
| Operational excellence with patient centered operations | 2.55±0.50 |
| Effective resource management | 2.54±0.48 |
| Excellence framework | 2.66±0.49 |
| Eliminating challenges or constraints | 2.72±0.47 |
| Team work | 2.64±0.44 |
| Value stream mapping | 3.10±0.42 |
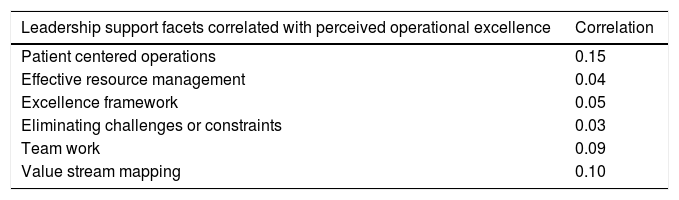
Results of correlation study.
| Leadership support facets correlated with perceived operational excellence | Correlation |
|---|---|
| Patient centered operations | 0.15 |
| Effective resource management | 0.04 |
| Excellence framework | 0.05 |
| Eliminating challenges or constraints | 0.03 |
| Team work | 0.09 |
| Value stream mapping | 0.10 |
n=80, *p<0.10, **p<0.01; two-tailed.
It is evident that none of the factors of leadership support correlated, were significant at the statistical significance level of 0.01(two tailed). Hence hypothesis 1 is not supported. At the same time, it is to be noticed that the correlation was highest with the leader ship factor for patient centered operations. This supports the second hypothesis.
DiscussionThe study tried to analyze empirically the relationship between factors of leadership support and operational excellence among executives in the health care sector in Kerala. Executives who perceive Leadership support will be more motivated to bring in operational excellence in terms of patient centered operations. The employees who perceive that leadership support is for patient centered operations will strive for operational excellence through patient centered operations. There was no significance for correlations among factors of leadership support, though patient centered operations showed a higher value of correlation. Perceptual differences and leadership styles may have contributed for this findings. Spurious correlation may be attributed to hidden factors. Study limitations include that it is also possible that executives perception of leadership support is passive and further research is required to examine the leadership support factors to patient centered operations and individual outcomes. The study may not be generalized across countries (Boyacigiller and Adler 1991; Hofstede (1991); Doktor et al. (1991; Wiersema and Bantel (1992)). Higher power distance exists in India and especially Kerala which leads to passive acceptance of leadership. Future research is probably required in this area for more clarification.
Further research will help to examine correlation between the leadership factors with individual operational excellence factors and outcomes, lean management, activity based costing and process improvements of six sigma and kaizen, accreditation processes and sustainability in hospitals. With aging population, increase in chronic diseases, life expectancy, lack of good hospitals and less number of competent doctors, commercialization of private hospitals with low leadership capabilities, arises the urgent need for research on empirical data on these lines to help practitioners and policy makers.
Additional research may help in assessing the process mechanisms by which leaders support for operational excellence. The perceived support from leaders will help to enhance operational excellence. This enhanced operational excellence in health care sector will benefit both the society and community of sick population at large, thereby increasing the trust in hospitals which will benefit the hospitals in the long run.
FundingWe received no funding for this study.
Conflict of interestThere is no conflict of interest.
Leader ship support:
- 1.
Leaders in my organization are always supportive in all operational processes.
- 2.
More involvement and support from Leaders in my organization are expected.
- 3.
Leaders in my organization need to motivate subordinates for better performance.
- 4.
Autonomy, rewards and recognition are given to subordinates by leaders in my organization.
Patient centered operations:
- 1.
Patients are the main focus in all operations in my organization.
- 2.
Cost is affordable and access and quality are ensured to all patients.
- 3.
Financial considerations are given to patients who are poor.
- 4.
Care quality is adequate and patients are satisfied.
Effective resource management:
- 1.
Resource development is part of management processes.
- 2.
Resource allocation and flexibility exists in my organization.
- 3.
Job burn-out is not their due to adequate staff and job rotation.
Excellence framework:
- 1.
Each department has pilot unit created to create role model units.
- 2.
Successful operational processes are benchmarked, standardized and used as framework.
- 3.
Excellence framework building is a continuous process in my organization.
Eliminating challenges or constraints:
- 1.
Challenges or constraints are constantly eliminated in my organization.
- 2.
Managers are equally responsible for identifying and eliminating challenges.
- 3.
Identifying challenges and solutions are considered as an accomplishment among executives.
Team work:
- 1.
The group I work with gives good support.
- 2.
Team leaders are cooperative and encouraging.
- 3.
Teams have common goals and accomplishments.
Value stream mapping:
- 1.
Organizational values are given utmost importance.
- 2.
Values are communicated constantly in my organization.
- 3.
Each department and unit have value streams mapped with organizational values.
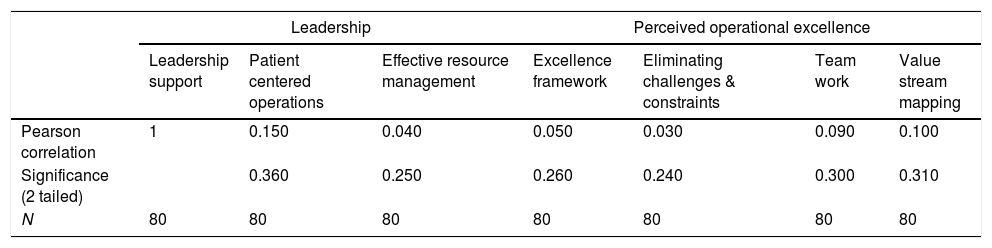
Correlation between leadership support and perceived operational excellence
| Leadership | Perceived operational excellence | ||||||
|---|---|---|---|---|---|---|---|
| Leadership support | Patient centered operations | Effective resource management | Excellence framework | Eliminating challenges & constraints | Team work | Value stream mapping | |
| Pearson correlation | 1 | 0.150 | 0.040 | 0.050 | 0.030 | 0.090 | 0.100 |
| Significance (2 tailed) | 0.360 | 0.250 | 0.260 | 0.240 | 0.300 | 0.310 | |
| N | 80 | 80 | 80 | 80 | 80 | 80 | 80 |

