



A 40-year-old woman presented to the Emergency Room with cough and hemoptysis for the past 2 weeks. There was no history of fever, dyspnoea or chest pain. Personal history of smoking consumption and hormonal contraceptive implant carrier.
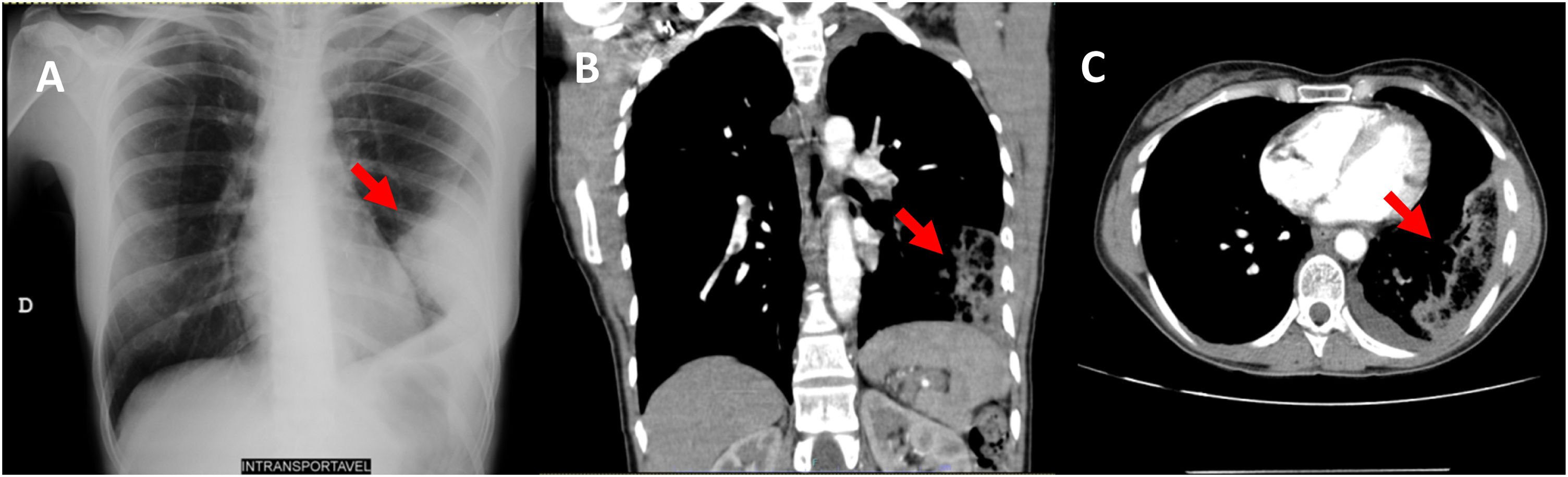
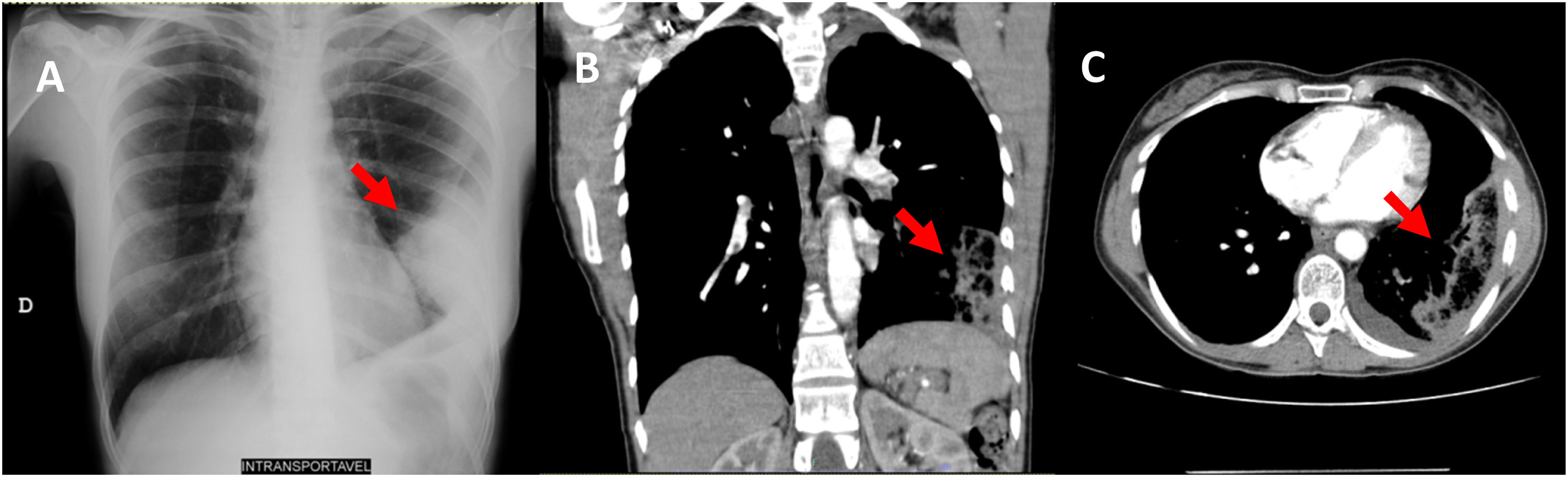
Physical examination was unremarkable: blood pressure 136/78mmHg, rhythmic pulse, heart rate of 80bpm, SpO2 of 99% while breathing air, normal pulmonary auscultation, revealing a symmetric vesicular murmur without adventitious sounds. Routine chemistry tests showed elevated d-dimer (2275ng/mL). The chest radiograph (CXR) revealed a wedge-shaped juxtapleural opacification (Hampton's Hump sign) (Fig. 1A). CT angiography of the chest showed signs of left acute pulmonary embolism (PE) with thrombus in the lower lobar artery, and extensive subpleural densification, suggesting infarction (Fig. 1B and C).
The patient was admitted with the diagnosis of PE and started anticoagulation.
The CXR is still the first line investigation for all cardiorespiratory symptoms suggestive of PE. However, a significant percentage of patients with acute PE present with minor and unspecific CXR alterations. Even though the Hampton's hump has a high specificity (82%), it has a low sensitivity (22%), hence importance should be placed in the ability to accurately recognise this sign on CXR,1 to promptly start treatment.
