



To determine the ability of brown algae (Sargassum sp) extract 15% in dissolving root canal smear layer.
MethodsThis study was an experimental laboratory with post-test only control group design. There were four groups of irrigation material, aquadest (Group 1); EDTA 17% (Group 2), NaOCL 2.5% (Group 3) and brown algae extract (Sargassum sp) 15% (Group 4). Each group consists of 6 samples (n=6). The cleanliness of root canal from the smear layer was checked using Crown Down Pressureless (CDP) technique with Protaper Next files and irrigated with each of irrigation material. The root canal hygiene was checked using Scanning Electron Microscopic (SEM) method and data were analyzed with the Kruskal Wallis test.
ResultsRoot canals that were irrigated using brown algae (Sargassum sp) extract 15% showed a significant decrease of smear layer compared to other groups (p<0.05) either in 1/3 middle portion or 1/3 apical portion.
ConclusionBrown algae (Sargassum sp) extract 15% was more effective to clean smear layer on root canal wall compared to NaOCl 2.5% but did not show a significant difference compared to EDTA 17%.
Root canal disinfection and sterilization is one of the stages in root canal treatment that acts as a lubricant during canal preparation, dissolves the necrotic pulp tissue, removes the smear layer, as well as bacteria and their products.1 Smear layer is a combination of dentine debris, pulp tissue, and bacteria. Smear layer will reduce the attachment of root canal filling material because organic material in smear layer can be a substrate for the growth of microorganisms, hence we need an irrigation solution that has the ability to dissolve the smear layer and clean it from root canal walls.2
Up till now, no irrigation solution has been used as a single agent and can work optimally.3 Therefore, researchers consider that it is necessary to develop alternative irrigation solution derived from natural material to dissolve the smear layer. One of which is brown algae (Sargassum sp). Brown algae Brown algae contain active compounds such as alkaloid, steroids, triterpene, flavonoids, tannins and saponins with various bioactivity so that it has the potential to be developed as a nutritional ingredient. Several studies have proven that brown algae have potential as an antibacterial, anticancer, antioxidant and anti-inflammatory ingredient.4
A study by Sakinah et al.5 that distinguished the cleanliness of irrigated root canals with 0.002% saponin mangosteen peel extract and sodium hypochlorite 2.5% showed that saponins are effective in dissolving smear layers. Hence, the authors were interested in conducting further research to determine the potential of brown algae extract (Sargassum sp) in dissolving root canal smear layer as one of the main requirements for irrigation solutions.
MethodsThis study was an experimental laboratory with post-test only control group design. The study was conducted at Environmental and Marine Sciences Laboratory, Faculty of Mathematics and Natural Sciences, Hasanuddin University, Makassar; Phytochemical Laboratory, Faculty of Pharmacy, Hasanuddin University, Makassar; Nanotechnology Laboratory, Institute of Technology Bandung (ITB), and at Hasanuddin University Dental Hospital, Makassar. Ethics was approved by the Ethical Commission of Dental Hospital Hasanuddin University. Brown algae (Sargassum sp) samples were obtained from Puntondo Island, Takalar Regency, South Sulawesi followed by a determination process in Environmental and Marine Sciences Laboratory, Faculty of Mathematics and Natural Sciences, Hasanuddin University, Makassar. Extracts were made through maceration using ethanol.
Twenty-four (n=24) samples of single root permanent human teeth were cleaned by ultrasonic scalers and then sterilized by autoclave. Work length was measured using K-file # 10 until it appeared at the apex end then reduced by 1mm. The root canal was explored using K-file # 15. All samples were randomly divided into four groups, 6 samples for each group. Root canal was prepared with Protaper Next file. During instrumentation, canals were irrigated using: group I – Aquadest solution, irrigated 2ml of solution for each file change, group II – 17% EDTA solution, irrigated as much as 2ml of solution for each file change, group III – sodium hypochlorite (NaOCl 2, 5%), irrigated as much as 2ml of solution for each file change, group IV – brown algae extract (Sargassum sp), irrigated as much as 2ml of solution for each file change. Each irrigation material was irrigated for 10s. In all groups, the final specimen was rinsed with 3ml distilled water and dried using a sterile absorbent paper point.
The specimens were then cut on the CEJ area of the crown using a diamond disc to obtain a root length of 10mm. One longitudinal groove was made on buccal and lingual surfaces of each tooth using a diamond disc, to avoid penetration into the canals. Then cut into two equal parts using a chisel and hammerhead.
The coded specimens were then placed on a metal beam with a carbon strip behind it and then observed using a Scanning Electron Microscope (SEM). Root canal wall was evaluated using SEM photomicrograph at 1500× magnification. Cleanliness of root canal wall from the smear layer was then evaluated using a scoring system according to Giovannone, et al.6
Score 1: None or no more than 25% of the smear layer, or more than 75% of open dentinal tubules.
Score 2: There is a smear layer between 25–50%, or 50–75% of open dentinal tubules.
Score 3: There is a smear layer between 50–75%, or less than 50% of open dentinal tubules.
Score 4: There is smear layer homogeneously in a dentinal surface; there is no open dentinal tubule.
The data were statistically analyzed using the Kruskal Wallis test and then continued to be analyzed using Mann Whitney Post Hoc test.
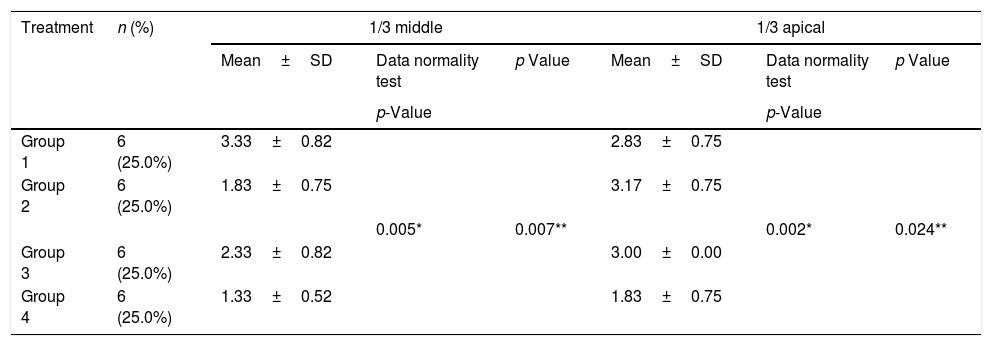
ResultsThe result showed a significant difference of root canal wall on the group IV (Sargassum sp) 15% compared with other groups (p<0.05) either in the middle third or apical third (Table 1).
Mean difference of root canal wall hygiene from smear layer among four groups of irrigation materials.
| Treatment | n (%) | 1/3 middle | 1/3 apical | ||||
|---|---|---|---|---|---|---|---|
| Mean±SD | Data normality test | p Value | Mean±SD | Data normality test | p Value | ||
| p-Value | p-Value | ||||||
| Group 1 | 6 (25.0%) | 3.33±0.82 | 2.83±0.75 | ||||
| Group 2 | 6 (25.0%) | 1.83±0.75 | 3.17±0.75 | ||||
| 0.005* | 0.007** | 0.002* | 0.024** | ||||
| Group 3 | 6 (25.0%) | 2.33±0.82 | 3.00±0.00 | ||||
| Group 4 | 6 (25.0%) | 1.33±0.52 | 1.83±0.75 | ||||
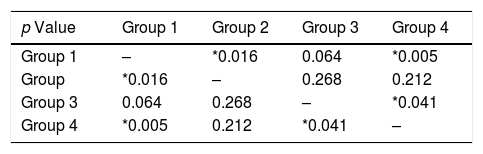
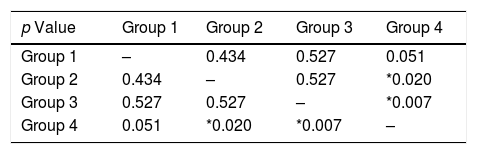
The analysis was then continued using Post Hoc with Mann Whitney. The results of the evaluation in middle third of group 4 (the brown algae), and group 3 (NaOCl) 2.5% showed a significant difference (p<0.05) and there was no significant difference on wall hygiene compared with group 2 (EDTA 17%) (p>0.05) as shown on Table 2. In the meantime, the evaluation in the apical third of group 4 (Sargassum sp) 15% showed there was a significant difference compared with group 3 (EDTA 17%) and group 2 (NaOCl 2.5%) (p<0.05) as shown in Table 3.
Pangestu et al.7 conducted a study on the effectiveness of phytochemical compounds of brown algae (Sargassum sp) and its activities as an antibacterial towards S. Aureus and E. Coli on concentration 5%, 10%, and 15%. The results showed that the biggest inhibition zone was obtained on concentration 15%.
As a preliminary study, there was a saponin test towards brown algae and it showed that the saponin within the extract used was shown in purple spots. In the treatment group of brown algae (Sargassum sp) extract 15%, there was plenty of open dentinal tubules and little or even none of smear layer on the root canal wall either in the middle third or the apical third. This was due to the fact that the extract contains saponin that has the ability of surfactant to tie up both organic and non-organic materials. Surfactant is able to reduce surface pressure in root canal covered by smear layer so the saponin particles can penetrate through dentinal tubules and bind with smear layer to form emulsion within the water, hence smear layer will be lifted and the dentine will be open.5
Meanwhile, a study by Giovannone et al.6 stated that a combination of NaOCl and EDTA did not result in smear layer – free root canal wall in the apical third. However, the study proved that the extract of brown algae was able to clean smear layer better than the positive control groups containing NaOCl 2.5% and EDTA 17% and the negative control group consisting of aquadest in the middle third and apical third. This was most likely to be caused by saponin content within Sargassum sp which is categorized into surfactant.6 The surfactant in the field of endodontic is commonly used to increase the efficacy of bactericide from disinfectant solution by combining different detergents as a surficial active compound to help decrease the surface pressure and increase the wettability of irrigation solution. High wettability enables a disinfectant solution to have more adaptability with dentine and penetration to dentinal tubules. It has been shown that the antibacterial agents different from detergents have lower surface pressure value and eliminate bacteria faster than agents without bacteria when contacting directly.8,9
Both the SEM and statistical analyses showed that in both the middle third and apical third, the highest hygiene level of root canal wall from the smear layer acquired by the brown algae (Sargassum sp) extract. This is in line with a study by Sakinah et al., suggested that it is due to saponin, a content of algae with surfactant characteristics.5
Based on a statistical analysis using Post Hoc with Mann Whitney test, this study found that there was a significant difference between brown algae (Sargassum sp) extract 15% and EDTA 17% in the middle third. However, in the apical third, brown algae extract was proven to clean the root canal better than EDTA 17% and NaOCl 2.5%. This was in agreement with a study by da Silva et al.,10 comparing the efficacy of EDTA 17% and EDTAC 15% in removing smear layer on root wall in coronal third, middle third, and apical third in vitro. The results showed that there was no significant difference in the wall hygiene from the smear layer in the coronal third; however, there was a significant difference in the middle third and apical third.
ConclusionThere was a significant difference between brown algae (Sargassum sp) extract 15% and EDTA 17% in the middle third of the root canal. However, in the apical third, brown algae extract was proven to clean the root canal better than EDTA 17% and NaOCl 2.5%. Brown algae (Sargassum sp) extract 15% was more useful to clean smear layer on root canal wall compared to NaOCl 2.5% but did not show a significant difference compared to EDTA 17%.
Conflict of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the International Conference on Women and Societal Perspective on Quality of Life (WOSQUAL-2019). Full-text and the content of it is under responsibility of authors of the article.
