

Recently, several studies have suggested that mindfulness-based training programs are beneficial for well-being and emotional regulation. In this article an assessment is presented on the effects of a Mindfulness-Based Stress Reduction Training Program on the extent of mindfulness, psychological well-being, empathy levels, emotional regulation and neuropsychological functions. Results showed that the trained group significantly increased their observation and non-judgment of inner experience variables. The trained group also improved in subjective psychological wellness, and emotional regulation, but not in attentional performance. The relationships between the results obtained are discussed, and a new method is proposed for assessing the capacity for emotional regulation. Further studies are necessary using larger samples.
En la actualidad disponemos de muchos estudios que demuestran que los programas de entrenamiento basados en Mindfulness producen beneficios sobre el bienestar psicológico y la capacidad de regulación emocional. En este estudio se analizaron los efectos producidos por un entrenamiento breve sobre los niveles de Mindfulness, el bienestar psicológico percibido, los niveles de empatía, la capacidad de regulación emocional y el rendimiento neuropsicológico. Los resultados mostraron que el grupo entrenado incrementó sus puntuaciones en las variables observación y ausencia de juicio. Además, este grupo también incrementó su nivel de bienestar psicológico percibido y su capacidad de regulación emocional, pero no obtuvo mejoras en la evaluación neuropsicológica en comparación con el grupo control. En la discusión se infieren posibles relaciones entre los resultados obtenidos, mientras que se propone un nuevo método para evaluar la capacidad de regulación emocional. Se requieren estudios con mayor tamaño de muestra para corroborar estos resultados preliminares.
Nowadays, there is evidence to suggest that mindfulness-based training programs increase psychological well-being and psychological well-being is related to different health benefits (Diener & Chan, 2011; Huppert, 2009; McConville, McAleer, & Hahne, 2017). However, the concept of psychological well-being is difficult to define. From a philosophical approach, it has been related to both hedonism and eudemonism. On the one hand, hedonism defines well-being as the experience of positive emotional states, the satisfaction of desires and the absence of negative affect. On the other, eudemonism suggests that well-being is not about maximizing positive experiences and minimizing negative ones, but about developing one's potential by performing activities consistent with deeply held values and full commitment If people feel alive and real, and they can reach an optimal state (Disabato, Goodman, Kashdan, Short, & Jarden, 2016). Many philosophical, spiritual and psychological traditions emphasize the importance of achieving an optimal state through being aware of the maintenance and enhancement of psychological well-being (Wilber, 2000). In this regard, mindfulness helps us to explore our conscience more gently, which increases our perception of well-being. Jon Kabat-Zinn (2015) said: “Mindfulness can be thought of as moment-to-moment, non-judgmental awareness, cultivated by paying attention in a specific way, that is, in the present moment, and as non-reactively, as non-judgmentally, and as openheartedly as possible”. This way of understanding mindfulness clearly point to the eudemonic perspective of psychological well-being.
Jon Kabat-Zinn introduced the concept of mindfulness-based training programs and developed his Mindfulness-Based Stress Reduction program (MBSR) (Kabat-Zinn, 1982). Although this program was for chronic pain patients, MBSR has been successfully adapted to other psychopathological disorders such as posttraumatic stress (PTSD), insomnia, depressive relapse or anxiety (Borquist-Conlon, Maynard, Brendel, & Farina, 2017; Gong et al., 2016; Hilton et al., 2016; Kuyken et al., 2016). Moreover, mindfulness-based training programs can improve overall psychological health in non-clinical populations. For example, Robins, Keng, Ekblad, and Brantley (2012) used a standard MBSR program (20 training hours) to compare non-clinical adults with a non-active control group on a waiting list. The results showed a significant increase in both trait mindfulness and self-compassion in the training group. They also observed a significant decrease in absent-mindedness, fear of emotions, suppression of anger, aggressive anger, worry and difficulty in regulating emotions. Another example is the study by Song and Lindquist (2015). They found that anxiety levels decreased in a training group versus a non-active control group on a waiting list after a mindfulness-based stress reduction program (MBSR) in a sample of Korean nursing students. It should be pointed out that long periods of practice are not necessary to achieve these health benefits because briefer meditation programs (with 7 sessions of 30min) can also reduce anxiety levels (Chen, Yang, Wang, & Zhang, 2013).
Another important component of mindfulness training programs that is related to psychological well-being is the development of empathy and compassion (Neff, 2011; Thomas et al., 2007). Several studies have assessed the effects of mindfulness training programs on empathy and compassion. Research on mindfulness and empathy has found that those who score high on mindfulness also tend to report increased levels of empathy and compassion (Asuero et al., 2014; Dekeyser, Raes, Leijssen, Leysen, & Dewulf, 2008; Shapiro, Brown, Thoresen, & Plante, 2011). The scientific literature also shows that both empathic and compassionate states are related with emotional regulation processes (Farb, Anderson, & Segal, 2012; Jazaieri et al., 2014; Lutz, Brefczynski-Lewis, Johnstone, & Davidson, 2008). One possible explanation for these effects has been put forward by Hayes and Feldman (2004). They suggest that people learn to distance themselves from their own internal and external experiences, which creates a more “offset” relationship that decreases emotional reactivity and facilitates the return to baseline. This hypothesis coincides with the facets of meditation usually included in mindfulness training programs (Nonreactivity to inner experience, Observing thought/feelings/perceptions, Acting with awareness, Describing with words, Nonjudging of experience) (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006; Chambers, Gullone, & Allen, 2009). Moreover, the practice of mindfulness has been shown to increase the activation of medial prefrontal (PFC), orbitofrontal (OFC) and anterior cingulate (ACC) cortices, three cerebral structures related to the processes of emotional regulation (Chambers et al., 2009; Etkin, Egner, & Kalisch, 2011). The prefrontal areas of the brain are well known to be involved in meditation practices and several studies show this strong relation (Fox et al., 2016; Hernández, Suero, Barros, González-Mora, & Rubia, 2016; Jang et al., 2011; Lazar et al., 2005). Since attentional processes play such a central role in meditation practices and there is evidence to suggest that prefrontal functions increase, we might expect to observe an increase in the attentional performance of meditation practitioners (Bichot, Heard, DeGennaro, & Desimone, 2015; Lippelt, Hommel, & Colzato, 2014). However, the results in the literature are contradictory. A systematic review by Lao, Kissane, and Meadows (2016) focused on eight studies on alerting/sustained attention but only one of them found a significant effect on attention performance using an adaptation of Mindfulness-based Cognitive Therapy (MBCT) (Oken et al., 2010). Other studies have reported improvements in selective attention and attentional control after MBSR training (Aherne et al., 2016; Fountain-Zaragoza & Prakash, 2017; Jensen, Vangkilde, Frokjaer, & Hasselbalch, 2012) but not in sustained attention (MacCoon, MacLean, Davidson, Saron, & Lutz, 2014). We can conclude that the effects of training in mindfulness on attention performance are unclear at present.
The aim of this pilot study was to evaluate the ability of rMBTP to improve perception of one's psychological well-being, levels of empathy and attentional performance. We also evaluated the effects of rMBTP on participants’ ability to regulate emotions using a new computerized emotional assessment protocol.
MethodParticipantsTwenty-five university students participated in the present study. The group of participants consisted of 18 women and 7 men between 18 and 30 years old (M=21.16, SD=3.06). Participants were randomly assigned to a non-active control group (n=15) and a training group (n=10). All participants had to be university students and were required to attend all the training sessions. Two subjects missed at least one training session and so were not included in the post-intervention statistical analyses. Students diagnosed with a mental disorder were not included in the study. Informed consents were appropriately obtained.
DesignThe study was a pragmatic controlled trial with pre- and post-intervention measurements. The rMBTP program was the between-subjects factor. At the beginning of the experimental procedure, all the groups were assessed. Then, the training group did the rMBTP for four weeks and the non-active group waited for post training assessment. When the training group had finished the rMBTP all the groups were assessed again.
Intervention designThe rMBTP consisted of four 2-h training sessions over four weeks (1 session/week). The training program included activities that were formal (audio-guided meditation exercises) and informal (like mindfulness in everyday activities). The content of each session was the following:
Session 1. What is mindfulness? How do you practice?
- •
Introducing ourselves, introduction of what we are going to do during rMBTP, theoretical introduction to meditation and mindfulness concepts, attitudes in mindfulness and anchorage practices: mindful breathing and mindful stop.
Session 2. How it reduces stress. Mindfulness and the body.
- •
Discussion about practice at home, how the mind functions during stress, the management of emotions and body meditation practices: body scan, mindful breathing and mindful walking.
Session 3. Meditation for loving kindness.
- •
Discussion about practice at home, theoretical introduction to “compassion and loving-kindness”, suffering as a human reality, generative meditation and contemplative meditation: contemplative meditation, Tonglen meditation and Metta meditation.
Session 4. Interpersonal mindfulness and maintenance of the practice.
- •
Discussion about practice at home, introduction to interpersonal mindfulness, offsetting up a personal meditation path, meditative practice in pairs, review of the meditation practice learned, group conclusions and farewell.
Self-administered psychological questionnaires, emotional assessment and neuropsychological tests were randomly administered to all participants in the study. The following standardized instruments of assessment were used:
Mindfulness assessment: Five Facets of Mindfulness Questionnaire (FFMQ) validated Spanish version (Aguado et al., 2015) containing five subscales: observing, describing, acting aware, non-judging and non-reacting.
Well-being assessment: Psychological Wellness Scale (EBP) (Cánovas, 1998). The following subscales were applied: subjective psychological wellness, material wellness and workplace wellness.
Anxiety assessment: Inventory of Situations and Responses of Anxiety (ISRA) Spanish adaptation (Miguel-Tobal & Cano-Vindel, 1988). This test assesses anxiety through four subscales: anxiety about the evaluation, interpersonal anxiety, phobic anxiety and anxiety about daily situations.
Empathy assessment: the four subscales of the Cognitive and Affective Empathy Test (TECA) (López-Pérez, Fernández-Pinto, & Abad, 2008): perspective taking, emphatic understanding, emphatic stress and emphatic joy.
Neuropsychological assessment: Trail Making Test (TMT A and TMT B) to evaluate visual and processing speed, attention, cognitive flexibility and motor function (Tamayo et al., 2012; Tombaugh, 2004). Attention Test D2 that measures attention, mental concentration, effort and attention control (Brickenkamp, 1972; González et al., 2012). Categorical evocation and verbal fluency subtests, from the Test Barcelona Reviewed (TBR) to assess semantic and phonological fluency related to executive functions (Peña-Casanova, 2005).
Emotional assessment: FaceReader® Software v.5 (Noldus Information Technologies, The Netherlands). FaceReader software is a tool that automatically analyzes facial expression and distinguishes the six basic emotions proposed by Ekman and Keltner (1970) (happiness, sadness, anger, fear, surprise, disgust and a neutral facial state). The system includes a computer with a built-in image capture system that locates the face. Then, an artificial neural network trained to categorize information and assign an emotional label analyzes the data obtained (Bishop, 1995). This software gives real time information on which emotion is being expressed on a continuous scale ranging from 0 (no expression) to 1 (maximum expression). We also calculated the time that each emotion was expressed. Because film clips had different durations, we calculated the time percentages of emotional expression.
Emotional assessment procedureTo induce emotional states with FaceReader, participants sat on a chair in front of a computer with a webcam (Microsoft life cam studio 1425 1080 pHD) on top (distance 60cm). In a different room, the examiner prepared various film clips and controlled the process. The videos in the pre-test phase were administered in the following order: Instructions (a written text explaining that they have to look at the screen, pay attention and not touch their face), “Misery” (to elicit fear), “The Lover” (to elicit neutral state), “Schindler's List” (to elicit sadness), “Something about Mary” (to elicit happiness), “Amputation” (to elicit disgust), and “Sleepers” (to elicit anger). After the rMBTP, the videos in the post-test phase were administered in the following order: Instructions (a written text explaining that they have to look at the screen, pay attention and not touch their face), “Seven” (to elicit fear), “Blue” (to elicit a neutral state), “Death penalty” (to elicit sadness), “When Harry met Sally” (to elicit happiness), “Pink Flamingos” (to elicit disgust), and “American History X” (to elicit anger). These videos (without “instructions”) were obtained from a Spanish validated battery of films to induce emotions (Megías, Mateos, Ribaudi, & Fernández-Abascal, 2011). None of the videos lasted for more than 3min.
Statistical analysisIndependent samples t-tests were used to analyze differences between control and trained groups. The statistical significance for all tests was set at 0.05. Cohen's d was used to calculate and to interpret the effect sizes (Cohen, 1992). All statistical analyses were performed using the statistics package IBM SPSS® v.22.
ResultsParticipants did not show significant statistical differences in the baseline scores (pre-test assessment) of the FFMQ test, the psychological and neuropsychological outcome measures, or the emotional expression time and emotional intensity measured by the software (data not shown).
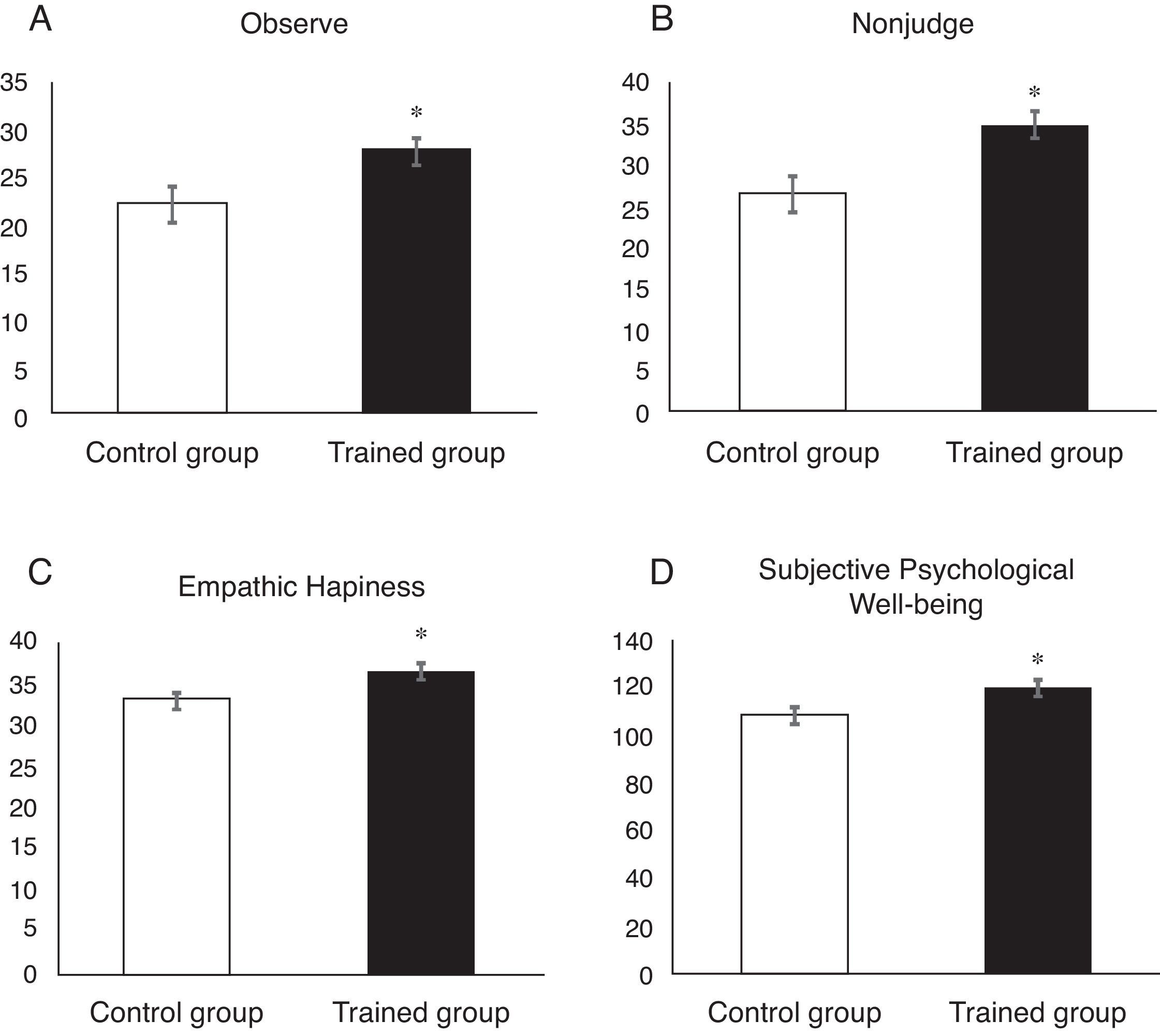
After training (post-test assessment), the trained group showed higher scores than the non-active control group on two FFMQ subscales: observing (t (22.95)=2.35, p=0.043) and non-judging (t (23)=2.86, p=0.009). The effect sizes (ES) were 0.981 (large effect) and 1.192 (large effect) respectively. Moreover, the trained group significantly improved in subjective psychological wellness according to the EBP (t (23)=2.22, p=0.037; ES=0.925 (large effect)), and emphatic happiness according to the TECA (t (23)=2.60, p=0.16; ES=1.084 (large effect)) (Fig. 1).
, TECA (Panel C) and EBP (Panel D) questionnaires. Data expressed as means (±SEM). An asterisk indicates significant differences between groups (p<0.05).")
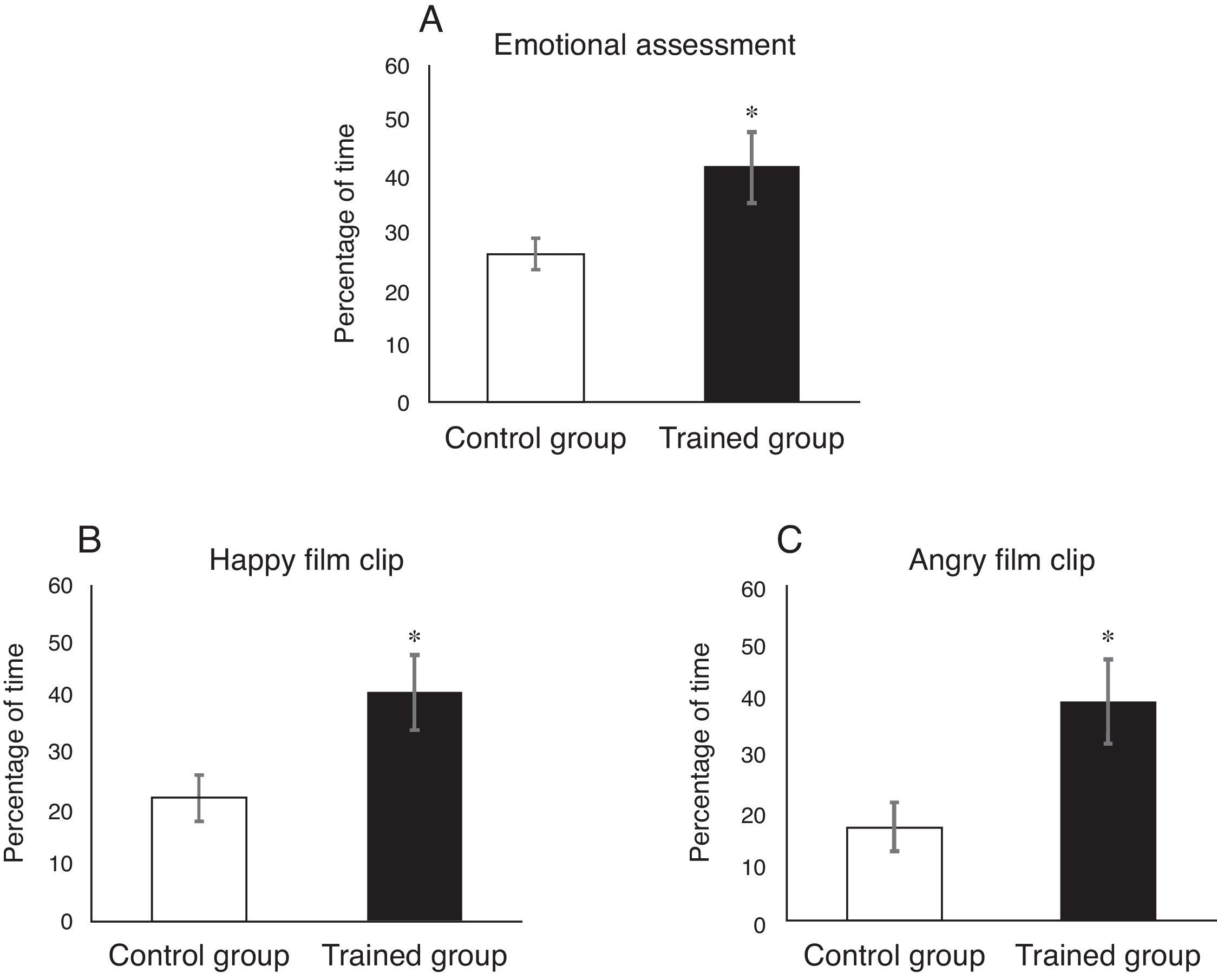
The results of emotional expression time showed that the trained group had a neutral facial expression for longer than the non-active control group throughout the emotional assessment (t (23)=2.5, p=0.02; ES=1.04 (large effect)). These differences were greater in the happy and angry film clips (t (23)=2.539, p=0.018; ES=1.05 (large effect) and t (23)=2.742, p=0.012; ES=1.14 (large effect) respectively) (Fig. 2).
 of percentage of time spent on neutral facial expression across the emotional assessment procedure (Panel A), Happy film clip (Panel B) and Angry film clip (Panel C). An asterisk indicated significant differences between groups (p<0.05).")
No differences in emotional expression intensities were observed between groups (data not shown). Finally, no significant differences in neuropsychological outcome measures were observed during the post-intervention evaluation (data not shown).
DiscussionIn the present study, we evaluated the effectiveness of a reduced mindfulness-based training program (rMBTP) at increasing the extent of mindfulness, psychological well-being, empathy and emotional regulation ability. Our results showed significant increases in two subscales of mindfulness (observing and non-judging of inner experience) for the trained group. These are noteworthy results since more extended mindfulness training programs lead to high scores in both observing and non-judging of inner experience (Lilja, Lundh, Josefsson, & Falkenström, 2013). At present, observing is considered to be the main variable required to achieve results on the other four subscales (observing, describing, acting aware, non-judging and non-reacting). Lilja et al. (2013) indicated that long experiences in mindfulness typically have a coupled effect on the observing and non-judging facets of mindfulness. Increases in observing with a low score on non-judging would indicate very early stages of training and a reduction in the tendency to ruminative observation and excessive self-criticism. Our results seem to suggest that our reduced training program is sufficient to improve the mindfulness of the sample. This is also important because significant improvements in other variables without increases in mindfulness could be related to non-specific variables that are not controlled in the experimental design (Gu, Strauss, Bond, & Cavanagh, 2015).
Our results also indicated a higher level of empathic joy after rMBTP training. This improvement facilitates the feeling of joy caused by positive events that happen to other people and the ability to share positive emotions. This ability is related to a better quality of social networks since empathic behaviors in positive emotional contexts relax people's threat detection system and allow a secure and receptive relationship between individuals (Eisenberg, Davidson, & Harrington, 2002; Simón, 2007). No other TECA subscales reached statistical significance probably because levels of empathy were already high before the rMBTP training in all groups. The percentiles obtained in the pre-training assessment ranged from 70 to 90 in both groups except for emphatic stress, which ranged from 45 to 55 in the control and trained groups. These high values might be related to high percentage of women in this study because they systematically score higher than men on this variable (Hojat et al., 2002).
We did not observe a reduction in anxiety levels after the mindfulness training even though standard MBSR programs seem to produce small to moderate improvements in anxiety (Goyal et al., 2014; Khoury, Sharma, Rush, & Fournier, 2015). Song and Lindquist (2015) proposed that the scientific literature shows that the health benefits on anxiety and depression of MBSR programs are dose-dependent. Therefore, they are highly sensitive to reductions in the number of sessions. Chen et al. (2013) observed reductions in the anxiety levels of participants after a program with seven sessions of 30min. Our initial hypothesis was that 8h of training will reduce the anxiety levels of participants. This discrepancy between results may be related to the program design because, in the study by Chen et al. (2013), participants were trained on seven consecutive days whereas in our training program participants were only trained one day per week.
Our results showed no improvements in attentional performance after the mindfulness training either. Previous studies suggest there are two possible reasons for our results. On the one hand, training probably needs to be intensive if improvements in neuropsychological functions are to be significant. Several studies have shown that programs need to be longer (for example, training retreats) to obtain significant improvements in any neuropsychological function (Anderson, Lau, Segal, & Bishop, 2007; Jacobs et al., 2011; Lao et al., 2016; Semple, 2010). On the other hand, this discrepancy could be related to the tests used for assessing attentional performance because there are several differences across the studies (Chambers, Lo, & Allen, 2008; Oken et al., 2010).
As far as emotional time expression is concerned, the trained group spent more time with a neutral facial expression throughout the emotional assessment period than the non-active control group during post-training evaluation. These differences were greater for the happy (positive valence) and angry (negative valence) film clips. In this regard, our results coincide with those of Hayes and Feldman (2004) and suggest that mindfulness helps to decrease emotional reactivity and facilitates the return to baseline after the emotional reaction. Ives-Deliperi, Solms, and Meintjes (2011) used brain functional magnetic resonance to compare brain activation during meditation with brain activation during a control task. They found that the insula and the prefrontal cortex were less active during meditation, and concluded that lower activity in the insula during meditation leads to a lower probability of reacting. Our data showed that the emotional recovery of participants in the trained group is the same for positive and negative valence stimuli. This finding supports the hypothesis that the relationship established with emotions through mindfulness practice is eudemonic (Disabato et al., 2016). However, no significant differences were observed in emotional intensity after training. Mindfulness has a set of attitudes that can be regarded as emotional regulation strategies: not judging, patience, beginner's mind, trust, non-striving, acceptance, release and constancy (Kabat-Zinn, 2003). These attitudes do not promote an active struggle against emotional expression but they do help us to manage emotion more efficiently. Thus, we do not expect to observe significant reductions in emotional intensity but we do expect more efficient regulation in trained participants. Finally, our results confirm that reduced training programs in mindfulness can improve the self-assessment of psychological well-being (McConville et al., 2017). This is by no means the least important of our findings because psychological well-being is a basic and necessary mental state for achieving a sense of internal coherence and self-satisfaction.
To sum up, reduced training programs in mindfulness can improve psychological well-being, levels of empathy and the ability of emotional regulation in the short term. However, longer periods of training are necessary to improve attentional performance or to reduce anxiety levels. Although this was a randomized controlled trial study, the number of participants is insufficient for our results to be generalized. Neither have we made any assessment of whether these improvements are maintained over time. Finally, emotional assessment using film clips and facial recognition software could be a suitable method for continuing the research in the field of mindfulness training programs and emotional regulation.
The authors wish to thank Jose Ignacio Fraile for their technical support.