



In recent years, growing evidence has been reported on the presence of non-motor symptoms in amyotrophic lateral sclerosis (ALS), such as those affecting cognition. Between 30% and 50% of patients with ALS may present cognitive disorders1,2, and approximately 15% meet diagnostic criteria for frontotemporal dementia3. These patients’ cognitive profile is characterised by deficits in executive function (especially in fluency), language, social cognition, and verbal memory1. The Edinburgh Cognitive and Behavioural ALS Screen (ECAS)4 is a screening tool designed to asses behavioural alterations and cognitive performance in multiple domains in patients with ALS. The ECAS has been validated in a Spanish population and cut-off scores have been established5; however, age- and education-adjusted cut-off scores are yet to be published. Sociodemographic variables should be considered due to their impact on ECAS scores. This study aims to analyse the association between these sociodemographic factors and ECAS scores in a cohort of patients with ALS.
MethodsWe collected clinical and sociodemographic data and ECAS scores from a cohort of patients with ALS (probable/definite ALS according to the El Escorial criteria) from our centre. We gathered total ECAS scores, ALS-specific ECAS scores (including the cognitive domains of language, fluency, and executive functions), ALS-nonspecific ECAS scores (including memory and visuospatial functions), and individual ECAS domain scores. We calculated the Spearman correlation coefficient to analyse the association between education level and ECAS scores, and the Mann-Whitney U test and effect sizes (Hedges’ g) were used to compare groups in terms of age (< 65 vs ≥ 65 years, based on the established age limit of onset of neurodegenerative diseases) and education (< 10 vs ≥ 10 years of schooling).
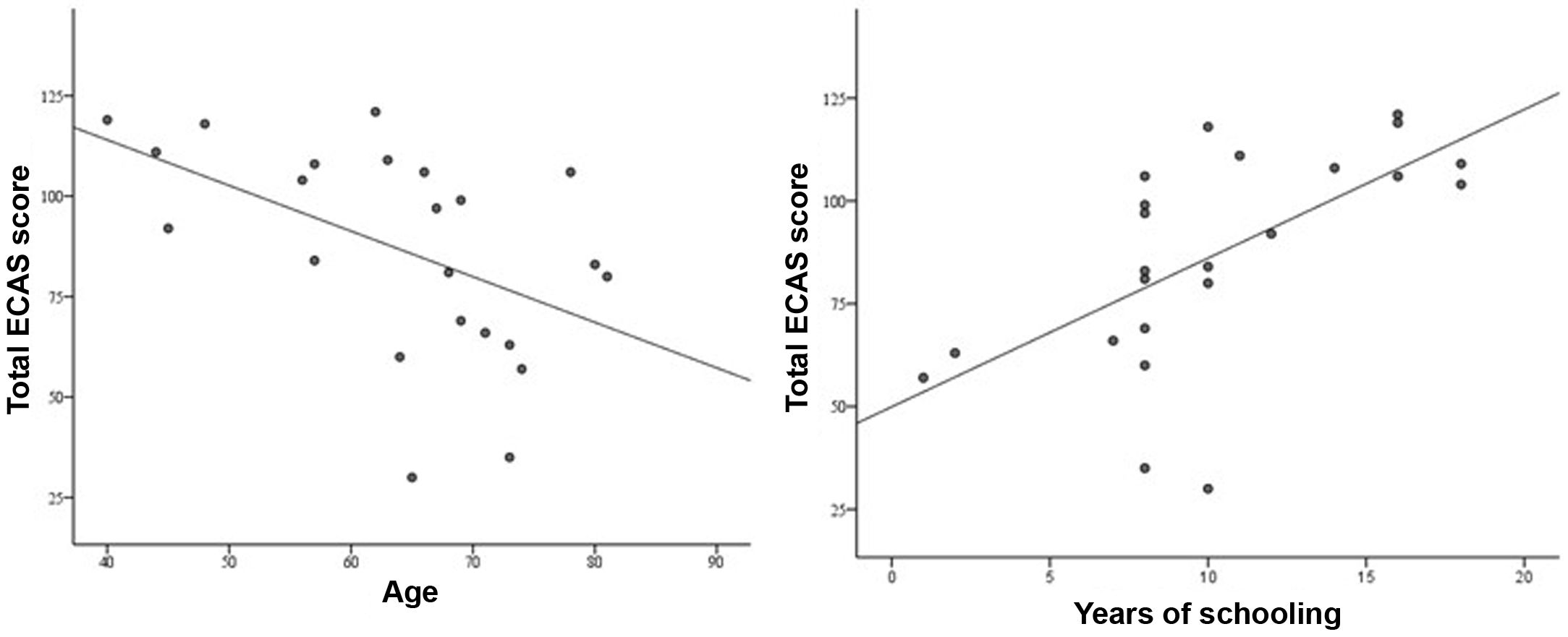
ResultsOur sample included 23 patients (60.9% men; mean age, 63.9 ± 11.46 years; mean years of schooling, 10.2 ± 4.48); 20 (86.96%) had spinal-onset ALS and 3 (13.04%) had bulbar-onset ALS. Age and education level were significantly correlated with total ECAS score (Spearman rho = –0.593; P = .003 and rho = 0.691; P < .001, respectively) (Fig. 1), ALS-specific ECAS score (rho = –0.610; P = .002 and rho = 0.681; P < .001, respectively), and ALS-nonspecific ECAS score (rho = –0.436; P = .037 and rho = 0.519; P = .011, respectively), as well as with individual ECAS domain scores (age: rho = –0.521 to –0.608; P ≤ .05; education level: rho = 0.428 to 0.674; P ≤ .05). Table 1 compares ECAS scores between age and education groups, providing effect sizes. We found significant differences (P ≤ .05) in ECAS scores between patients younger than and older than 65 years (except for ALS-nonspecific ECAS scores: P = .201) and between patients with less than or more than 10 years of schooling (except for ECAS fluency score: P = .092). The effect size was moderate for differences between age groups in ALS-nonspecific ECAS score and ECAS visuospatial score (g = 0.61 and g = 0.56, respectively) and for differences between education groups for ALS-nonspecific ECAS score and ECAS fluency score (g = 0.65). We found a large size effect in the remaining comparisions. No correlation was observed between Revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R) scores and ECAS scores in the total sample, nor did we find differences in ALSFRS-R scores between age groups.
 and level of education (right).")
ECAS scores by age and education group.
| Total ECAS | ALS-specific ECAS | ALS-nonspecific ECAS | ECASLanguage | ECASFluency | ECASExecutive | ECASMemory | ECAS Visuospatial | |
|---|---|---|---|---|---|---|---|---|
| Age | ||||||||
| < 65 years(n = 9) | 108 (88−118.5) | 84 (61.5−88.5) | 28 (22.5−31.5) | 25.5 (20−26.5) | 20 (14−20) | 39 (25−41) | 19 (15.5−19.5) | 12 (11−12) |
| ≥ 65 years (n = 14) | 80.5 (61.5−100.7) | 57.5 (38.5−74) | 24.5 (16−29.2) | 20.5 (15−24) | 10 (8−16) | 26 (11.7−32.7) | 14.5 (11−18) | 10 (9−11.2) |
| Pa | .016* | .007* | .210 | .009* | .011* | .046 | .039* | .039* |
| g | 1.05 | 1.16 | 0.61 | 1.24 | 0.92 | 1.02 | 0.93 | 0.56 |
| Schooling | ||||||||
| < 10 years(n = 11) | 69 (60−97) | 50 (39−67) | 23 (20−27) | 20 (15−24) | 10 (10−16) | 20 (10−29) | 14 (11−17) | 10 (9−11) |
| ≥ 10 years (n = 12) | 107 (86−116.2) | 80 (58.7−87.5) | 29.5 (25−32) | 25.5 (20.7−26) | 17 (9.5−20) | 39 (27.2−41.7) | 19 (15.2−20) | 12 (11−12) |
| Pa | .007* | .011* | .027* | .023* | .091 | .019* | .006* | .007* |
| g | 1.04 | 1.02 | 0.65 | 0.94 | 0.65 | 1.07 | 1.21 | 1.04 |
Data are expressed as medians (p25–p75).
ECAS: Edinburgh Cognitive and Behavioural ALS Screen; ALS: amyotrophic lateral sclerosis; g: Hedges’ g.
Age and education level were found to have an impact on ECAS scores. Overall, patients with higher education levels scored better, while older patients performed worse. The effect size of the difference between age and education groups was large for most cognitive scores. Non-significant differences may be due to the small size of the groups; however, most differences did show statistical significance. These results were not correlated with ALSFRS-R scores, which were similar in both age groups, suggesting that age does not have an impact on disease progression.
The main limitation of our study is its small sample size, which limits the possibility of drawing general conclusions. However, our results are in line with those of studies reporting an association between age and education in the English and Swiss-German versions of the ECAS in control populations,6,7 which provides age- and education-adjusted cut-off scores.
ConclusionsAge and education level were found to have an impact on cognitive performance in our sample. Our results underscore the need to analyse these sociodemographic variables in a control population to obtain more sensitive age- and education-adjusted cut-off scores for the Spanish version of the ECAS, with the aim to improve the detection of cognitive impairment in ALS patients.
FundingThe data presented in this study are drawn from the project “Study of cognitive and neuropsychiatric characteristics of patients with amyotrophic lateral sclerosis,” funded by Fundació Catalana d’ELA Miquel Valls.
