








Dos tercios de los pacientes infectados por SARS-CoV-2 presentan síntomas persistentes después de la infección.
ObjetivosEstudiar los beneficios de un programa de rehabilitación respiratoria (PRR) en pacientes con COVID persistente, y comparar los resultados en función del tiempo de evolución y la forma de presentación.
MétodosAnálisis post hoc de una cohorte prospectiva de pacientes con COVID persistente. Se evaluaron los cambios en la escala modificada de disnea del Medical Research Council (mMRC), prueba de marcha de 6minutos (PM6M), presiones inspiratoria y espiratoria máximas (PImax y PEmax) y fuerza muscular periférica. Pruebas estadísticas utilizadas: chi-cuadrado, t de Student para muestras apareadas e independientes, análisis de la varianza de un factor y modelo lineal general.
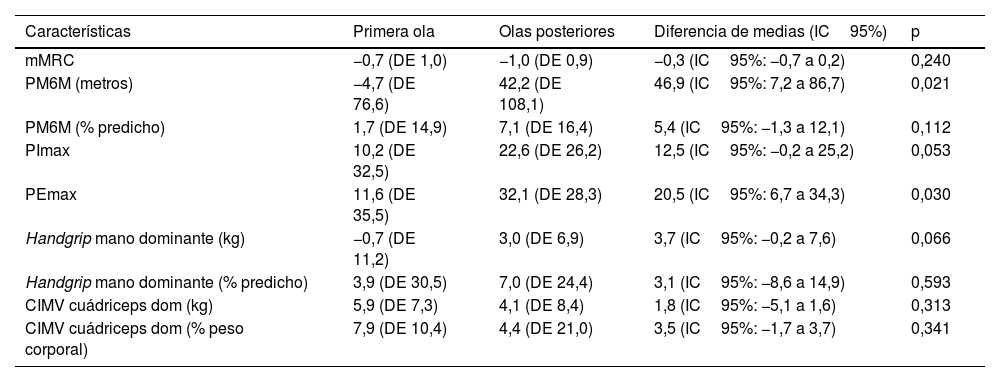
ResultadosDe 158 derivados a Rehabilitación, hubo 110 pacientes (edad 58,1años; 57,3% mujeres) que iniciaron el PRR. Tras la intervención, se encontraron mejoras significativas de 0,8 puntos (IC95%: −1,1 a −0,6) en la escala mMRC de disnea, de 19,6m (IC95%: −0,8 a 39,9) en la PM6M, de 16,8cmH2O (IC95%: 10,3 a 23,2) en la PImax, de 22,5cmH2O (IC95%: 15,3 a 29,7) en la PEmax, y de 5,0kg (IC95%: 3,3 a 6,7) en la fuerza del cuádriceps. Aunque estas mejoras se produjeron independientemente del momento de la infección y el tiempo de evolución, los pacientes de la primera ola mostraron mejoras más discretas.
ConclusionesEl PRR muestra beneficios clínicos y funcionales en los pacientes con COVID persistente, independientemente del tiempo de evolución y de la gravedad inicial de la infección.
Two-thirds of patients infected with SARS-CoV-2 experience persistent symptoms after infection.
ObjectivesTo study the benefits of a respiratory rehabilitation program (RRP) in patients with long COVID and compare the results based on the time of evolution and clinical presentation.
MethodsPost-hoc analysis of a prospective cohort of patients with long COVID. Changes were evaluated using the modified Medical Research Council (mMRC) dyspnea scale, the 6-minute walk test (6MWT), maximal inspiratory and expiratory pressures (maxIP and maxEP), and peripheral muscle strength. Statistical tests used: Chi-square, paired and independent t-Student tests, one-way ANOVA, and a general linear model.
ResultsOut of 158 patients referred to rehabilitation, 110 (mean age 58.1years; 57.3% women) started the RRP. After the intervention, significant improvements were observed: a reduction of 0.8 points (95%CI: −1.1 to −0.6) on the mMRC dyspnea scale, an increase of 19.6m (95%CI: −0.8 to 39.9) in the 6MWT, 16.8cmH2O (95%CI: 10.3 to 23.2) in maxIP, 22.5cmH2O (95%CI: 15.3 to 29.7) in maxEP, and 5.0kg (95%CI: 3.3 to 6.7) in quadriceps strength. Although these improvements were independent of infection onset and disease duration, patients from the first wave showed more modest improvements.
ConclusionsThe RRP provides clinical and functional benefits for patients with long COVID, regardless of disease duration and initial severity of infection.
