


Although the transradial approach has reduced vascular complications, radial artery occlusion is still considered one of its limitations. The aim of this study was to evaluate radial artery patency after transradial cardiac catheterization.
MethodsProspective cohort study of patients undergoing cardiac catheterization using the transradial approach. Procedures were performed with 5F and 6F catheters with the administration of 5,000IU of heparin and 200μg of nitroglycerin through the radial sheath. Radial artery blood flow was assessed by Doppler before, immediately after bandage removal and 7 days after the procedure.
ResultsThe study included 120 patients of which 42.5% were males, with 59.1±10.6years of age, 25.8% were diabetic, weighing 77.4±14.2kg and height of 166±8.1cm. The number of catheters used was 2.3±0.5 per patient, 55.8% using 6F sheaths. The duration of the procedure was 14.8±5.2minutes, the puncture time was 129.7±124.1seconds, and the fluoroscopy time was 4±2.3minutes. Radial spasm and crossover to the femoral technique occurred in 20.8% and 1.7% of the procedures, respectively. Significant hematoma was observed in 2.4% of the patients. At 1 week of follow-up, arterial occlusion was observed in 1.7%, and reduced blood flow in 26.7% of the patients.
ConclusionsRadial artery occlusion following diagnostic procedure using the transradial approach is rare and should not be considered as an important technique limitation.
Avaliação da Patência da Artéria Radialapós Cateterismo Transradial
IntroduçãoEmbora a abordagem transradial tenha reduzido as complicações vasculares, a oclusão da artéria radial ainda é uma de suas limitações. O objetivo deste estudo foi avaliar a patência da artéria radial após cateterismo cardíaco transradial.
MétodosEstudo de coorte prospectivo com pacientes submetidos a cateterismo cardíaco pela via transradial. Os procedimentos foram realizados com cateteres 5F ou 6F, com a administração de 5.000 U de heparina e 200μg de nitroglicerina através do introdutor radial. O fluxo sanguíneo na artéria radial foi avaliado com o uso do Doppler antes, imediatamente após a retirada do curativo e 7 dias depois do procedimento.
ResultadosO estudo incluiu 120 pacientes, dos quais 42,5% eram do sexo masculino, com idade de 59,1±10,6 anos, 25,8% eram diabéticos, com peso de 77,4±14,2kg e altura de 166±8,1cm. O número de cateteres utilizados foi de 2,3±0,5 por paciente, 55,8% usando introdutores 6F. A duração do procedimento foi de 14,8±5,2 minutos, o tempo de punção foi de 129,7±124,1 segundos e o tempo de fluoroscopia, de 4±2,3 minutos. Espasmo e crossover para técnica femoral ocorreram em 20,8% e 1,7% dos procedimentos, respectivamente. Hematoma significativo ocorreu em 2,4% dos pacientes. Em uma semana de acompanhamento, observaram-se oclusões da artéria em 1,7% e redução do fluxo sanguíneo em 26,7% dos pacientes.
ConclusõesA oclusão da artéria radial pós-procedimento diagnóstico utilizando a via de acesso radial é infrequente e não deve ser considerada limitação importante da técnica.
The transradial approach is widely used in percutaneous procedures because it allows for complex interventions with a significant reduction in vascular complication rates. 1-7 Recent studies have demonstrated that this approach results in additional comfort to patients, 8 shorter hospitalization duration, 9 and lower hospital expenses. 10 The radial access route requires a longer learning curve. 11-13
Radial artery occlusion is another potential limitation to this technique, and its occurrence varies between 2% and 9%. 14,15 Ischemic heart disease frequently causes patients to undergo more than one invasive procedure (diagnostic or therapeutic), and an occluded access route prevents a new approach through the vessel.
Considering the insufficiency of data in the Brazilian specialized literature, this study aimed to determine the radial artery patency after transradial cardiac catheterization.
METHODSSample selectionPatients referred for elective cardiac catheterization performed by the transradial approach between May 2009 and December 2010 were included in the study. The inclusion criteria were: age>18 years, positive Allen’s test, and agreement to participate in the study, which included returning one week after the procedure evaluate the blood flow in the radial artery. The exclusion criteria were defined as a history of prior coronary artery bypass graft (CABG) surgery, emergency procedures, or chronic renal failure. All the patients signed an informed consent approved by the ethics committee of the institution.
Diagnostic procedure via radial approachAfter Allen’s test 16 was performed for hand movement evaluation, the patients were positioned in a supine position with the right arm extended along the body. Local antisepsis with chlorhexidine was performed, sterile drapes were placed, and the wrist (approximately 1cm above the styloid process of the radius) was anesthetized with 2% lidocaine (3 to 5mL). Using a 21G sheath, the radial artery was punctured and cannulated, and a 0.021-inch guide wire was inserted. A 5F or 6F radial sheath was inserted under the guide wire (Terumo Glidesheath, Terumo Corporation – Tokyo, Japan/Cordis Transradial System, Cordis Corp. – Miami Lakes, United States). The use of precast catheters to perform the catheterization of the coronary ostia was at the surgeon’s discretion. A dose of 5,000 U of heparin was routinely administered intravenously, as well as 200mg of nitroglycerine through the radial sheath.
At the end of the procedure, a compression dressing with gauze and Tensoplast® was retained for four hours. The dressing was reassessed every hour, and in the case of inadequate hemostasis after the fourth hour, the dressing was redone.
Clinical follow-up and assessment of blood flow in the radial arteryThe blood flow in the radial artery was routinely assessed prior to the start of the examination, immediately after removing the dressing and on the seventh day of follow-up using, a portable vascular Doppler echocardiograph with a 10MHz transducer. The presence of radial artery flow was measured above and below the puncture site.
Study definitionsThe puncture time was measured between the start of anaesthesia and insertion of the sheath. The procedure time was described as the time between the local anaesthesia and removal of the last catheter. Fluoroscopy time was obtained directly from the haemodynamic equipment.
The presence of spasm was defined as the coexistence of pain reported by the patient and difficulty of catheter manipulation by the surgeon.
Major vascular complications were defined as hand ischemia, vascular perforation, radial artery pseudoaneurysm formation or arteriovenous fistula, and need for surgery. Minor complications included local hematomas, classified according to the “Early Discharge after Transradial Stenting of Coronary Arteries (EASY)” study: 9 type I, < 5cm in diameter; type II, < 10cm diameter; type III, > 10cm, without reaching the elbow; type IV, hematoma extending beyond the elbow; and type V, any haematoma resulting in ischemic injury to the hand. Local pain was subjectively classified as absent, mild, moderate, and intolerable.
Arterial occlusion was defined as the absence of radial flow, measured by Doppler echocardiography, distal to the puncture site on the seventh day after the procedure. In cases of preserved blood flow in the radial artery, it was further classified as normal or reduced, compared with the blood flow proximal to the puncture site.
Statistical analysisThe data were prospectively collected and stored in a specific database. The analysis was performed using SPSS software program, release 17.0 for Windows. Continuous variables were shown as the mean and standard deviation, and categorical variables were shown as absolute numbers and percentages.
RESULTSClinical variablesA total of 122 patients was included in the study. Of these, two did not return on the seventh day after the procedure to have the blood flow in the radial artery assessed, and were, therefore, excluded.
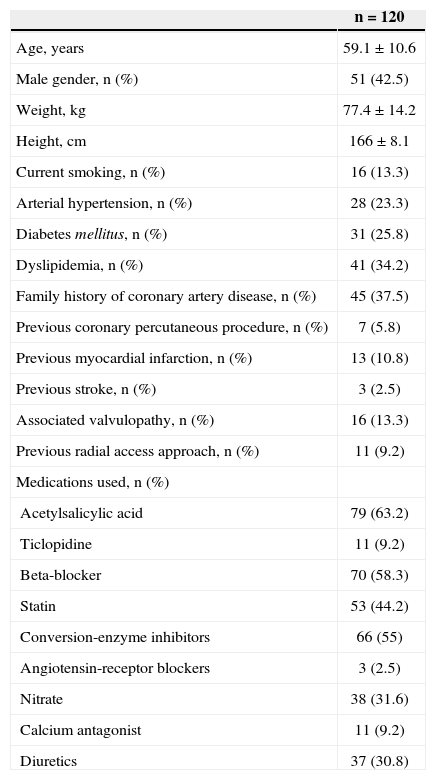
The patients were predominantly female (57.5%), aged 59.1±10.6years, with mean weight of 77.4±14.2kg and mean height of 166±8.1cm, and 25.8% were diabetics. Among the patients enrolled, 11 (9.2%) had undergone previous cardiac catheterization through the radial approach (Table 1).
Clinical characteristics of the patients undergoing diagnostic cardiac catheterization via the radial approach
| n=120 | |
|---|---|
| Age, years | 59.1±10.6 |
| Male gender, n (%) | 51 (42.5) |
| Weight, kg | 77.4±14.2 |
| Height, cm | 166±8.1 |
| Current smoking, n (%) | 16 (13.3) |
| Arterial hypertension, n (%) | 28 (23.3) |
| Diabetes mellitus, n (%) | 31 (25.8) |
| Dyslipidemia, n (%) | 41 (34.2) |
| Family history of coronary artery disease, n (%) | 45 (37.5) |
| Previous coronary percutaneous procedure, n (%) | 7 (5.8) |
| Previous myocardial infarction, n (%) | 13 (10.8) |
| Previous stroke, n (%) | 3 (2.5) |
| Associated valvulopathy, n (%) | 16 (13.3) |
| Previous radial access approach, n (%) | 11 (9.2) |
| Medications used, n (%) | |
| Acetylsalicylic acid | 79 (63.2) |
| Ticlopidine | 11 (9.2) |
| Beta-blocker | 70 (58.3) |
| Statin | 53 (44.2) |
| Conversion-enzyme inhibitors | 66 (55) |
| Angiotensin-receptor blockers | 3 (2.5) |
| Nitrate | 38 (31.6) |
| Calcium antagonist | 11 (9.2) |
| Diuretics | 37 (30.8) |
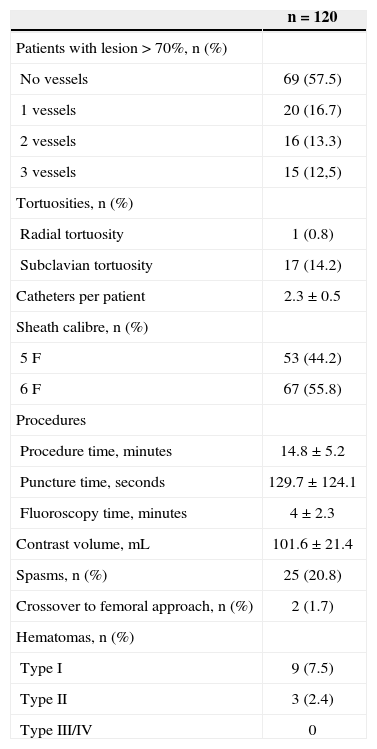
The number of catheters used for coronary catheterization was 2.3±0.5 per patient; 5F (53/120, 44.2%) and 6F (67/120, 55.8%) sheaths were used. The mean procedure duration was 14.8±5.2minutes, the duration of puncture was 129.7±124.1seconds, and the fluoroscopy time was 4±2.3minutes. The contrast volume used was 101.6±21.4mL (Table 2).
Angiographic and procedural characteristics
| n=120 | |
|---|---|
| Patients with lesion>70%, n (%) | |
| No vessels | 69 (57.5) |
| 1 vessels | 20 (16.7) |
| 2 vessels | 16 (13.3) |
| 3 vessels | 15 (12,5) |
| Tortuosities, n (%) | |
| Radial tortuosity | 1 (0.8) |
| Subclavian tortuosity | 17 (14.2) |
| Catheters per patient | 2.3±0.5 |
| Sheath calibre, n (%) | |
| 5F | 53 (44.2) |
| 6F | 67 (55.8) |
| Procedures | |
| Procedure time, minutes | 14.8±5.2 |
| Puncture time, seconds | 129.7±124.1 |
| Fluoroscopy time, minutes | 4±2.3 |
| Contrast volume, mL | 101.6±21.4 |
| Spasms, n (%) | 25 (20.8) |
| Crossover to femoral approach, n (%) | 2 (1.7) |
| Hematomas, n (%) | |
| Type I | 9 (7.5) |
| Type II | 3 (2.4) |
| Type III/IV | 0 |
There were no major complications such as radial artery pseudoaneurysm formation, arteriovenous fistula, or compartment syndrome. Among the minor complications (Table 2), there were type-I hematomas in nine patients (7.5%) and type-II hematomas in three patients (2.4%). Type-III and IV hematomas were not observed in this sample. Regarding pain after the procedure, nine patients (7.5%) complained of mild discomfort, one (0.8%) of moderate pain, two (1.7%) of intolerable pain, and 108 patients (90%) denied any discomfort. Spasms occurred in 25 cases (20.8%), but the crossover to the femoral technique occurred in only two patients (1.7%).
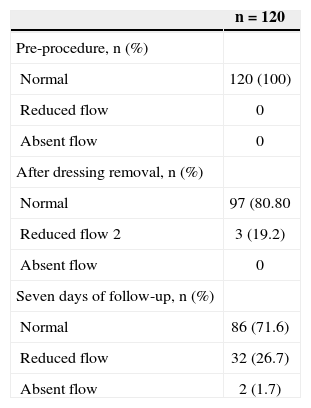
Clinical follow-up and blood flow assessment in the radial arteryOn the seventh day after the procedure, the radial artery flow was normal in 86 (71.6%), reduced in 32 (26.7%), and absent in two (1.7%) patients (Table 3).
Evaluation of radial arterial blood flow by Doppler echocardiography
| n=120 | |
|---|---|
| Pre-procedure, n (%) | |
| Normal | 120 (100) |
| Reduced flow | 0 |
| Absent flow | 0 |
| After dressing removal, n (%) | |
| Normal | 97 (80.80 |
| Reduced flow 2 | 3 (19.2) |
| Absent flow | 0 |
| Seven days of follow-up, n (%) | |
| Normal | 86 (71.6) |
| Reduced flow | 32 (26.7) |
| Absent flow | 2 (1.7) |
The radial access approach was introduced by Campeau 17 and is currently used in interventional cardiology. The frequency of its use varies in catheterization laboratories. 18
The prevalence of radial artery occlusion after cannulation varies between 2% and 9%. 14,15 In the majority of cases, with Allen’s test preservation, the occlusion is asymptomatic. Several factors have been associated with vessel occlusion, such as the type of compression used, the introducer sheath/vessel diameter ratio, 19 the administered heparin dose, 15 and the maintenance of flow distal to the puncture site during compression. 20 Occlusion is most likely determined by a combination of several factors.
In this study population, the incidence of blood flow occlusion was lower than that in previous studies, occurring in two patients (1.7%). Although a logical explanation is not yet available, the authors hypothesize that the systematic use of heparin at a dose of 5,000 U may have had a role in the lower incidence. It is known that inadequate anticoagulation is an important factor in the rate of blood flow occlusion and, in the present study; the mean dose was 66 U/kg per patient. With this dose, full anticoagulation with heparin is attained, and the dosage may be one of the factors that contributed to the maintenance of arterial patency. Although bivalirudin 21 was not tested in the present study, it has been described as an anticoagulation regimen. Despite having lower rates of post-procedural blood flow occlusion, the cost remains a limiting factor in its usage.
Although the occlusion rate was low, it was observed that approximately 25% of the population had decreased flow between the dressing removal and the seventh day of follow-up. Although the reduction in blood flow is clinically irrelevant, Burstein et al. 22 demonstrated that significant radial arterial flow alterations occur after cannulation. The Doppler echocardiography assessment demonstrated that the measurement of flow-mediated dilation was altered after using the radial access route. In addition to the physiological alterations, endothelial modifications have been reported. 23 Considering that the radial artery is a good vascular graft to be used in CABG, 23,24 these alterations in vessel physiology should be considered regarding the use of the radial approach. 25
Study limitationsThis study had certain limitations. The radial occlusion rate was extremely low, perhaps due to the routine use of Doppler echocardiography. Assessment by Doppler is more sensitive than manual palpation to detect vascular flow, and Doppler could identify blood flow in cases in which palpation could not. It was not possible to determine possible predictors of radial occlusion due to the small number of events in the study.
CONCLUSIONSRadial artery occlusion following a diagnostic procedure is a rare event, and should not be considered as an important limitation to the technique.
CONFLICT OF INTERESTThe authors declare no conflicts of interest.