



Mitral valve aneurysm is a rare and uncommon complication of infective endocarditis leading to a weakened mitral tissue. The most feared mitral valve aneurysm's complications are: perforation and severe mitral regurgitation. Multiple mechanisms have been suggested to explain the development of mitral valve aneurysm in aortic infective endocarditis including: local extension of the infection, the mitral kissing vegetation and aortic regurgitation. We report the case of a 29-year-old man who had infective endocarditis of a native aortic valve and the sub-aortic diaphragm complicated by a perforated mitral valve aneurysm diagnosed only by transesophageal echocardiogram. The patient had no sign of heart failure. We hypothesized that all those mechanisms lead to the developing of the mitral valve aneurysm in this case, but also the presence of the diaphragm favored the spread of the infection.
Una de las complicaciones poco comunes e inusuales de la endocarditis infecciosa son los aneurismas de la válvula mitral. Las complicaciones más temidas de estos últimos son la perforación y la insuficiencia mitral severa. Diferentes mecanismos pueden explicar el desarrollo de dicha insuficiencia en el contexto de una endocarditis infecciosa, incluyendo una extensión local, una vegetación sobre la válvula mitral y una insuficiencia aórtica.
Nuestro caso clínico es el de un joven de 29 años diagnosticado de endocarditis infecciosa sobre su válvula aortica nativa con un diafragma subaortico complicado con un aneurisma de la válvula mitral perforado. El paciente no presentaba signos de insuficiencia cardíaca. Hemos supuesto que todos los mecanismos que hemos evocado anteriormente han llevado al desarrollo de dicho aneurisma, junto con la presencia del diafragma, elemento en favor de la diseminación de la infección.
Infective endocarditis is responsible of multiple valve destruction and local extension. Mitral valve aneurysm occurs rarely but with a high incidence of complication leading to urgent surgery. The occurrence of mitral valve aneurysm's complication such as rupture does not always lead to a sever mitral regurgitation like in our case. There is no actual consensus on the management strategy of this entity. It is presented a case of aortic and subaortic diaphragm endocarditis complicated with aneurysm of the anterior mitral leaflet.
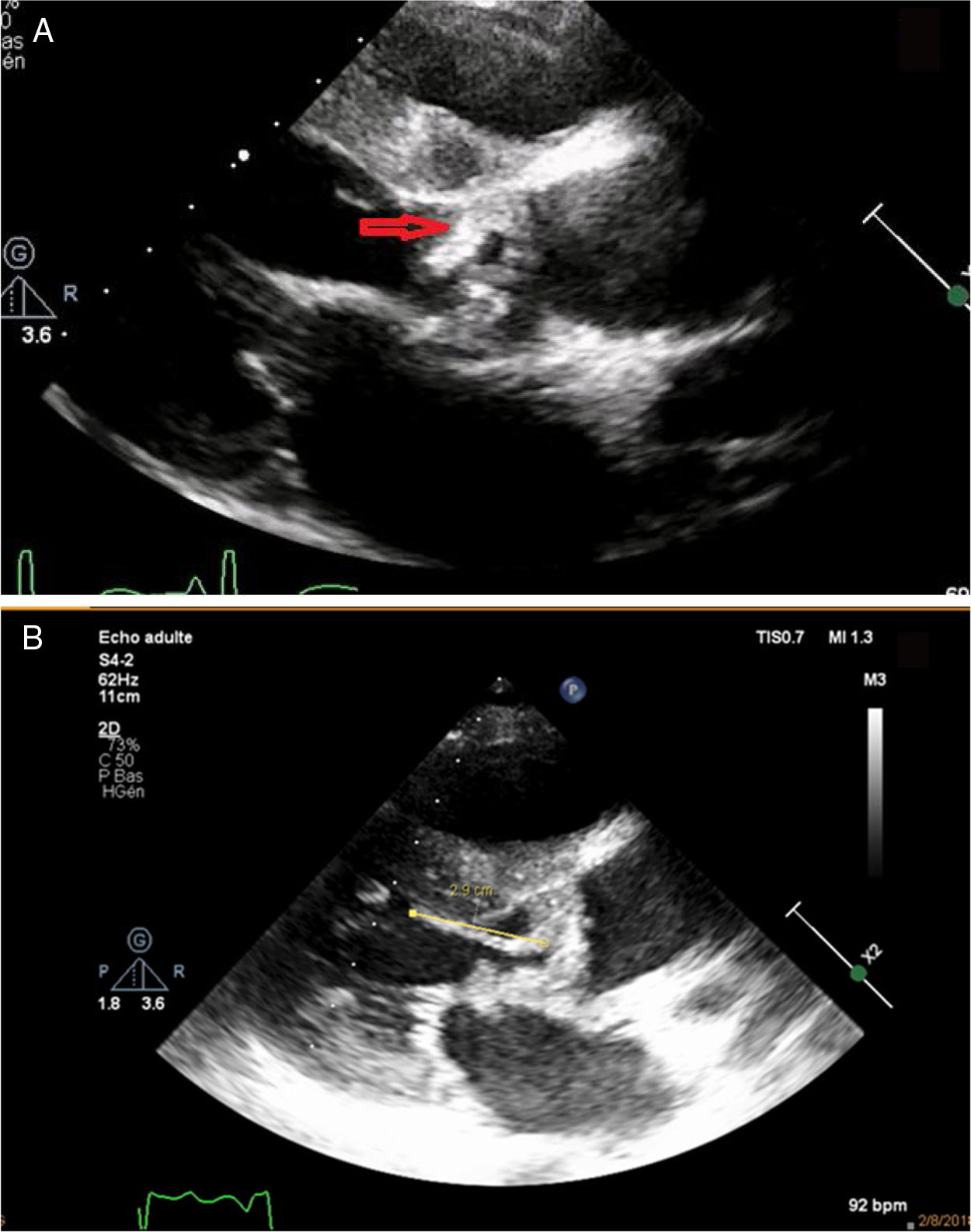
ObjectivesMitral aneurysms are a rare complication of infective endocarditis causing important mitral insufficiency and hemodynamic instability that should be early diagnosed with a close follow up. Transthoracic echocardiogram is not very sensible for the diagnosis. It must be overlooked especially when we have aortic endocarditis or sub aortic membranous which may play a role in the occurrence of the mitral valve aneurysm (fig. 1).
Case report a mobile mass on the sub-aortic diaphragm (arrow) (B) leading to a direct contact with the anterior mitral valve “kissing vegetation”.")
29-year-old male with a history of sub-aortic diaphragm resection and patent arterial duct ligation in 1992. He was admitted to cardiology department with a two-month history of intermittent fever, dry cough, weight loss and fatigue. On physical examination, the patient was febrile (37.8°C), blood pressure was 112/63mm Hg, pulse was 112 bpm, with no sign of heart failure. Cardiac auscultation found a grade 3/6 holosystolic murmur and a grade 2/6 protodiastolic murmur at the aortic area with a normal S2. Blood analysis showed elevated C-reactive protein (CRP) and normal white blood cells (WBC) count. Blood cultures were positive for Streptococcus bovis (fig. 2).
.")
An electrocardiogram revealed a left ventricular hypertrophy and the chest X-rays did not show any abnormalities. A transthoracic echocardiogram (TTE) was performed and showed good left and right ventricular function with left ventricular (LV) slight dilatation, recurrence of the sub-valvular diaphragm with multiple mobile echodensities on the diaphragm and aortic valve prolapsing into the left ventricular outflow (the largest one: 2.8cm). There was also evidence of aortic peri-annular abscess communicating with the aorta, and we suspected the presence of vegetation on the atrial side of anterior mitral valve leaflet. The mean aortic gradient was 29mm Hg and aortic surface area was 0.7cm2/m2, which indicated a moderate aortic stenosis with a sever aortic regurgitation. A transesophageal echocardiogram (TEE) was subsequently performed, which confirmed the previous findings, but also identified a perforated saccular bulging (mitral valve aneurysm) on the anterior mitral valve. The colour flow Doppler demonstrated two moderate regurgitations jets: first one through the coaptation of mitral valve and second one through the perforated aneurysm. TEE showed also a second peri aortic abscess communicating with the LV; an extension along the mitral-aortic intervalvular fibrosa and vegetations on the aortic root. Patient received antibiotic therapy(ATB) with ceftriaxone and gentamicin. A body computed tomography scan showed multiple subclinical complications: spleen and kidneys infarction and a small intra cranial mycotic aneurysm. After one week of antibiotic therapy, it was noted an abolition of the femoral, popliteal and distal pulse on the left, without clinical symptoms. The duplex examination showed an occlusion of the superficial femoral artery with resumption on the popliteal artery with a downstream demodulated flow. A clinical and biological stabilization were obtained and surgery was delayed after 4 weeks of ATB. Patient underwent aortic valve replacement with diaphragm resection and mitral repair and died second day after surgery of refractory arrhythmia (fig. 3).
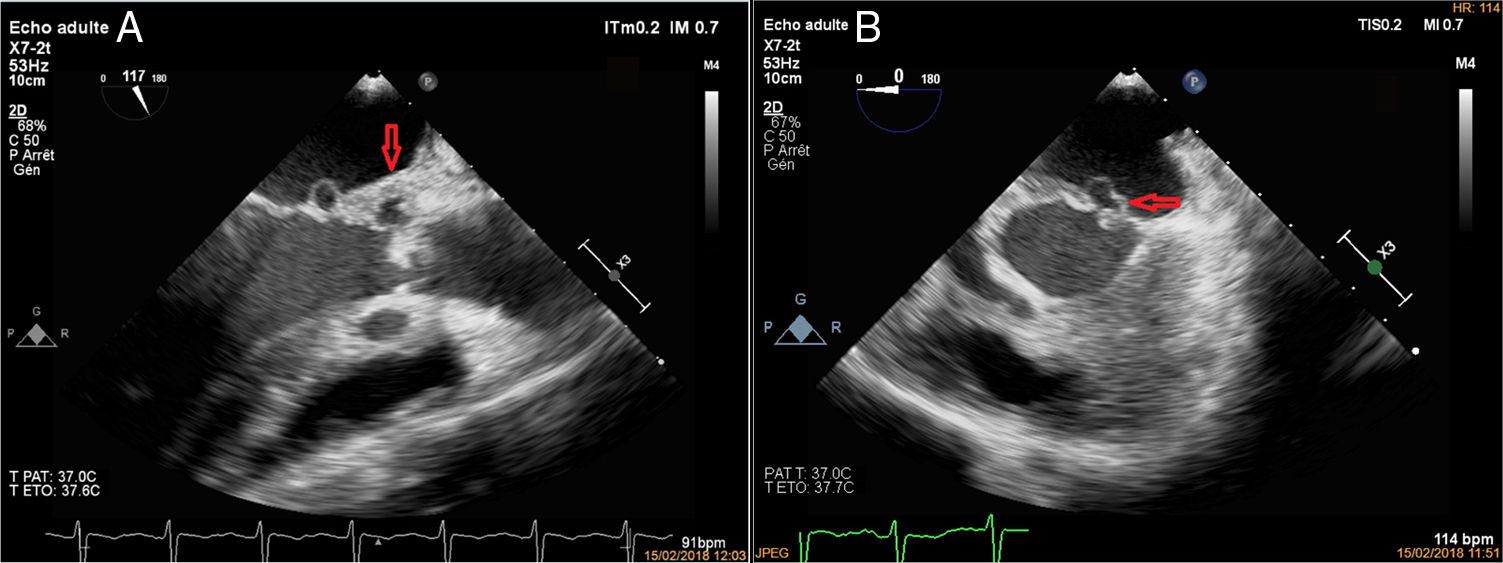
 three chamber view revealing an anterior mitral leaflet aneurysm and an abscess in the aortic mitral intervalvular fibrosa (arrow) suggesting the local extension of infection and (B) four chamber view showing the saccular bulging on the anterior mitral valve (arrow).")
Transesophageal echocardiography (A) three chamber view revealing an anterior mitral leaflet aneurysm and an abscess in the aortic mitral intervalvular fibrosa (arrow) suggesting the local extension of infection and (B) four chamber view showing the saccular bulging on the anterior mitral valve (arrow).
Infective endocarditis is a life-threaten cardiovascular disease with a high mortality despite all the advances in the medical fields. Mitral valve aneurysm are rare and yet very serious complication of infective endocarditis. However, other non-infectious disorders causing connective tissue degeneration have been associated with mitral valve aneurysm. The incidence reported is 0.2-0.29%.1 The anterior mitral valve aneurysm is more commonly observed than the posterior mitral valve aneurysm. This finding has been well-described by Seratnahaei et al.2 highlighting the role of neo-vessels in the formation of aneurysm which are more prominent in the anterior MV. Mitral valve aneurysm are usually misdiagnosed as myxomatous degeneration, mitral prolapse, papillary fibroelastoma or vegetation as in the case presented.3 Mitral valve aneurysm appears to be a saccular bulging on the left atrium side of the mitral valve with systolic expansion and diastolic collapse, a diastolic expansion occurs when ruptured mitral valve aneurysm or severe aortic regurgitation.1 Multiple mechanisms through different cases have been reported for the development of mitral valve aneurysm including infected eccentric aortic regurgitant jet that strikes the ventricular surface of the anterior mitral leaflet “jet lesion” causing seeding and physical trauma (vulnerable scar tissue), the extension of infection through the mitral aortic intervalvular fibrosa results in abscess on the anterior mital valve with drainage eventually, and also the direct contact of a large aortic vegetation with the mitral valve.4,5 In this case, all those mechanisms are possibly involved in the weakening of underlying tissue and the development of mitral valve aneurysm at the same time. We think that the presence in this case of a sub-aortic membranous reduces the distance between the infected tissue (aortic) and the supposed healthy tissue (mitral) resulting in a faster spread of the infection, and accentuates the eccentricity of the aortic jet and turbulence. Mitral valve aneurysm is often ruptured causing a severe mitral regurgitation, heart failure and deterioration in the hemodynamic status, which will indicate an urgent surgery. Though the complexity of mechanisms involved and the rupture on the mitral valve aneurysm, our patient was stable and had elective conservative surgery. The management strategy for mitral valve aneurysm remains unclear, and it depends on the size and complications of the aneurysm, the anatomic disorders and valve destruction.6,7 Mitral repair has been shown to have better clinical in hospital and long-term results than mitral valve replacement.8,9
ConclusionGiven the rarity of this entity, there is not enough studies to determine whether the size, the morphologic features of mitral valve aneurysm and the mechanisms leading to its formation have an impact on the therapeutic strategy and the prognosis.
Conflict of interestNone.
The authors wish to thank the physicians in cardiology B department of CHU Ibn Sina Rabat, for their assistance and intellectual discussion.