



Although rheumatoid arthritis care models consider a symptomatic approach and intervention of disability, it is also important to have a model that integrates advances in the pharmacological management, as well as non-drug treatment strategies.
Materials and methodsA descriptive cross-sectional retrospective study was conducted that included 640 patients diagnosed with rheumatoid arthritis and in an outpatient comprehensive care program. The first assessments made by occupational therapy with a full functional evaluation including the Barthel index, Quick DASH scale, and the Health Assessment Questionnaire. The activity of the disease was calculated using DAS28.
ResultsHigher HAQ scores were observed as the level of disease activity increased. There were no significant differences in the level of activity of the disease among subjects who worked and those who did not. A low correlation was found between the DAS28 and the Quick DASH in 2 evaluation modules (r=0.399 for instrumental and r=0.291 for the work module) (p<0.005). Of the 350 subjects, 66.7% had some degree of disease activity and the percentage of patients shown to have a moderate to severe limitation in the functioning of the upper limb was 66.1% for the work module and 84.75% for the instrumental module, showing a greater functional limitation as the level of disease activity increased.
ConclusionThis study has reassessed the applying of generic scales that deal with generally functionality, within the care program.
Los modelos de atención en artritis reumatoide consideran el abordaje sintomático y la intervención de discapacidad; sin embargo, es importante un modelo que integre los avances en el manejo farmacológico y las estrategias no farmacológicas.
Materiales y métodosEstudio retrospectivo, descriptivo, transversal, en el que incluimos a 640 pacientes con diagnóstico de artritis reumatoide que estaban participando en un programa de atención integral ambulatoria; tomamos las primeras valoraciones realizadas por terapia ocupacional con la evaluación funcional completa que incluían: índice de Barthel, escala Quick DASH y Health Assessment Questionnaire. El nivel de actividad de la enfermedad se calculó a través del DAS28.
ResultadosSe evidenciaron puntuaciones más altas del HAQ a medida que el nivel de actividad de la enfermedad aumenta; no se encontraron diferencias significativas en cuanto al nivel de actividad de la enfermedad entre los sujetos que laboran y los que no. Encontramos una baja asociación entre el DAS28 y el Quick DASH en sus 2módulos de evaluación (r = 0,399 para el instrumental y r = 0,291 para el módulo laboral; p < 0,005). De los 350 sujetos, el 66,7% presentó algún grado de actividad de la enfermedad y el porcentaje de pacientes que calificaron una limitación de moderada a severa en la función de su extremidad superior fue del 66,1% para el módulo laboral y del 84,75% para el módulo instrumental, con mayor limitación funcional a medida que aumenta el nivel de actividad de la enfermedad.
ConclusionesEste estudio ha permitido reevaluar dentro del programa la aplicación de escalas genéricas que abordan de forma general la funcionalidad.
Rheumatoid arthritis (RA) is an inflammatory, systemic, chronic incurable disease, whose main target is the synovial membrane; it generates joint pain, stiffness and inflammation, and it can cause systemic involvement and lead to a significant degree of disability.1–3 A study of Afro-Colombians in Colombia in 2001 reported a hospital incidence of 0.65 per 1000 people-year4 and the study Disease Burden in Colombia of 2005 concluded an overall prevalence of 0.9/100 inhabitants, with a women:men ratio of 4:1.5
It is considered that in 5–20% of cases it has a self-limited course, 60–90% of them have a polycyclic evolution toward progressive deterioration and about 75% do not achieve complete remission despite treatment,1,3,6–8 with functional and structural changes that lead to limitation in activity and restriction in participation, which leads to deterioration in the quality of life, significant disability and loss of roles.5–9 RA is a chronic disease with multiple impacts on the individual, which are reflected in society, and which requires a model of care that incorporates contextual factors dependent on the individual, the environment and the health-disease process.2
The models of care in RA consider the symptomatic approach and the intervention on the disability.2 However, a model like the one that has been developing in Riesgo de Fractura S. A.-CAYRE since 2009 integrates the advances in pharmacological management,3,7 in the context of an interdisciplinary care10 through integral programs, which are more beneficial, since they allow to establish coordinated actions addressed to specific problems, with an individualized management plan according to the functional ability; programs that consider the variable prognosis of the disease and measure the effect of the interventions.3 This integrality, in addition, allows the participation of patients’ organizations.1,3,10
This study seeks to make an approximation to the functional impact in a group of patients with RA, evaluated within a program of comprehensive care for autoimmune diseases in the outpatient setting called PARATI.
Patients and methodsPatientsThe study included 640 patients, older than 18 years of age, of both sexes, with a diagnosis of RA according to the 1987 criteria of the American College of Rheumatology, who were in a comprehensive ambulatory care program for patients with inflammatory and autoimmune rheumatic diseases and who received biological therapy. The first assessments carried out by an occupational therapist trained in the application of functional scales, between January 2014 and December 2015 were taken, without the need for standardization of their application, since there was only a single evaluator. Of the 640 subjects, a sample of 350 patients was taken for the analysis of correlations between the functionality scales and the level of disease activity (DAS28). The subjects with incomplete information within the database were excluded, as well as those who did not have the simultaneous application of the evaluation instruments.
The PARATI program is carried out in the healthcare provider institution, Riesgo de Fractura S. A.-CAYRE, and it includes the interdisciplinary evaluation by Rheumatology and healthcare professionals with experience in RA (physiatrists, general practitioners, professional nurse, pharmaceutical chemists, psychologist, occupational therapist, social worker and nursing assistants).
EvaluationsWithin the functional assessment in the program, 2 of the 4 functional scales applied by the occupational therapist were analyzed: the Barthel index,11 which evaluates the individual's ability to perform basic activities of daily living (eating, bathing, getting dressed, getting ready, bowel movement, urination, going to the toilet, transfers chair/bed, ambulation and use of stairs), and assesses the degree of independence. It is not a continuous scale, since the assignation of the scoring is made counting by fives (between 0, 5, 10 and 15 points), the total sum varies from 0 to 100: being 100 the maximum independence and 0 the maximum dependence.12
The other scale used is the Quick DASH,13 which allows to evaluate the function of the upper limb for instrumental activities. It consists of one module that evaluates the percentage of disability/symptoms through a questionnaire of 11 questions that inquires about the functional limitations in daily activities and a second work module with 4 questions about the functional limitation in the performance of work activities.14
The measurement scales were applied to the patient through a face-to-face interview during the functional assessment; and are validated to the Spanish language,11,15 without studies of socio-cultural validation in our country.
The functional assessment also includes the filling-out by the patient of the self-applied Health Assessment Questionnaire (HAQ),16 which is provided and calculated by the nurses of the program; it is a generic questionnaire that evaluates the function of the patient related to the daily life activities. All scales used are validated for their use in the Spanish language.
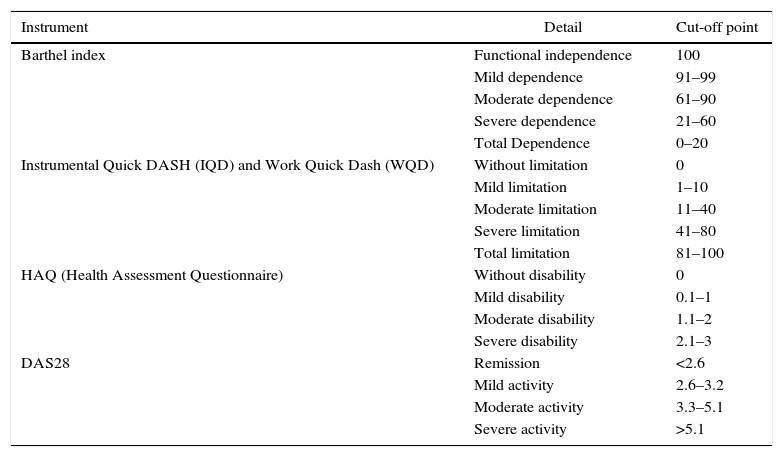
The level of disease activity is calculated through the disease activity score DAS28,17 applied by the rheumatologist, using the erythrocyte sedimentation rate (ESR by the Westergreen method), which is calculated on the day of the medical care in order to find this index. The cut-off points, the interpretation of the scales and the questionnaire on functionality, as well as the DAS28 are shown in Table 1.
Instruments for functional assessment and level of disease activity.
| Instrument | Detail | Cut-off point |
|---|---|---|
| Barthel index | Functional independence | 100 |
| Mild dependence | 91–99 | |
| Moderate dependence | 61–90 | |
| Severe dependence | 21–60 | |
| Total Dependence | 0–20 | |
| Instrumental Quick DASH (IQD) and Work Quick Dash (WQD) | Without limitation | 0 |
| Mild limitation | 1–10 | |
| Moderate limitation | 11–40 | |
| Severe limitation | 41–80 | |
| Total limitation | 81–100 | |
| HAQ (Health Assessment Questionnaire) | Without disability | 0 |
| Mild disability | 0.1–1 | |
| Moderate disability | 1.1–2 | |
| Severe disability | 2.1–3 | |
| DAS28 | Remission | <2.6 |
| Mild activity | 2.6–3.2 | |
| Moderate activity | 3.3–5.1 | |
| Severe activity | >5.1 |
The type of design is a retrospective, descriptive, cross sectional study, of a cohort of patients belonging to a comprehensive healthcare program. According to the Colombian legislation, this study is included into the category of studies without risk, in accordance with the guidelines established in resolution 008430/93.
Statistical analysisThe sample size in the present study was established by convenience. The existence of correlation between the level of disease activity (DAS28) and the result of the scales of functionality was evaluated for the analysis. The Pearson correlation coefficient was used in the bivariate analysis of non-parametric variables and a descriptive analysis of frequencies and percentages of the results of the scales and their relationship with socio-demographic and labor variables.
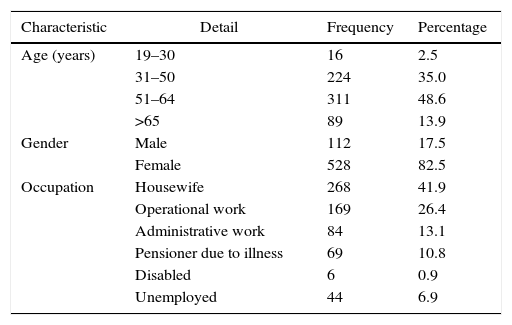
ResultsThere were found 640 subjects with a diagnosis of RA, with an age range between 19 and 93 years, and an average age of 53 years. In the evaluated population, it was evidenced a higher frequency in the female gender, in a percentage 4 times higher than for the male gender. Likewise, it was identified that the greatest number of subjects affected by the disease is found in the productive age group (30–65 years). The majority of the evaluated subjects are housewives, followed in frequency by workers of operational and administrative labors. 18.6% of the evaluated subjects are not working, because they are unemployed, are disabled or a condition of disability to work is already defined. The characteristics of the study subjects, as well as their occupation are presented in Table 2.
Characteristics of the population (n=640).
| Characteristic | Detail | Frequency | Percentage |
|---|---|---|---|
| Age (years) | 19–30 | 16 | 2.5 |
| 31–50 | 224 | 35.0 | |
| 51–64 | 311 | 48.6 | |
| >65 | 89 | 13.9 | |
| Gender | Male | 112 | 17.5 |
| Female | 528 | 82.5 | |
| Occupation | Housewife | 268 | 41.9 |
| Operational work | 169 | 26.4 | |
| Administrative work | 84 | 13.1 | |
| Pensioner due to illness | 69 | 10.8 | |
| Disabled | 6 | 0.9 | |
| Unemployed | 44 | 6.9 |
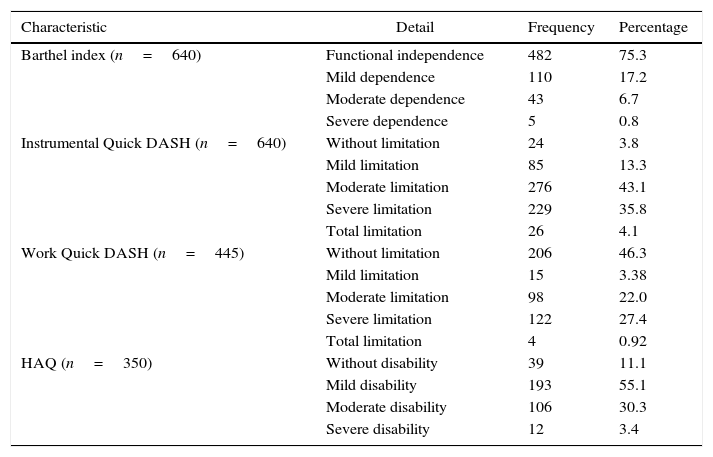
The result of the functional evaluation (Barthel index, Quick DASH and HAQ) of the population under study is presented in Table 3 with frequencies and percentages of presentation.
General description of the functional assessment.
| Characteristic | Detail | Frequency | Percentage |
|---|---|---|---|
| Barthel index (n=640) | Functional independence | 482 | 75.3 |
| Mild dependence | 110 | 17.2 | |
| Moderate dependence | 43 | 6.7 | |
| Severe dependence | 5 | 0.8 | |
| Instrumental Quick DASH (n=640) | Without limitation | 24 | 3.8 |
| Mild limitation | 85 | 13.3 | |
| Moderate limitation | 276 | 43.1 | |
| Severe limitation | 229 | 35.8 | |
| Total limitation | 26 | 4.1 | |
| Work Quick DASH (n=445) | Without limitation | 206 | 46.3 |
| Mild limitation | 15 | 3.38 | |
| Moderate limitation | 98 | 22.0 | |
| Severe limitation | 122 | 27.4 | |
| Total limitation | 4 | 0.92 | |
| HAQ (n=350) | Without disability | 39 | 11.1 |
| Mild disability | 193 | 55.1 | |
| Moderate disability | 106 | 30.3 | |
| Severe disability | 12 | 3.4 |
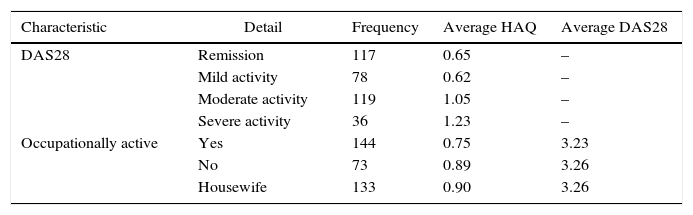
Regarding the level of disease activity it was found that, of the 350 subjects, 33.3% were in remission; 22.2% showed a mild level of disease activity; 34.2% a moderated level of activity and 10.3% presented a severe level of activity. Higher HAQ scores were evidenced as the level of disease activity increases; no significant differences in the level of disease activity were found between the subjects who work and those who do not, but the average of the HAQ score is slightly higher in the groups of those who do not work and in the housewives (Table 4).
Relationship between the level of disease activity (DAS28) and HAQ.
| Characteristic | Detail | Frequency | Average HAQ | Average DAS28 |
|---|---|---|---|---|
| DAS28 | Remission | 117 | 0.65 | – |
| Mild activity | 78 | 0.62 | – | |
| Moderate activity | 119 | 1.05 | – | |
| Severe activity | 36 | 1.23 | – | |
| Occupationally active | Yes | 144 | 0.75 | 3.23 |
| No | 73 | 0.89 | 3.26 | |
| Housewife | 133 | 0.90 | 3.26 |
It was found a low association between the DAS28 and the HAQ (r=0.364), as well as with the Quick DASH in its 2 evaluation modules (r=0.397 for the instrumental and r=0.285 for the work module; p<0.005). Of the 350 subjects with evaluation of the DAS28, 66.7% showed some degree of disease activity and the percentage of patients who rated a moderate to severe limitation in the function of their upper limb was 66.1% for the work module and 84.75% for the instrumental module, with greater functional limitation as the level of disease activity increases. There were evidenced subjects with low activity level or in remission with high scores in the Quick DASH.
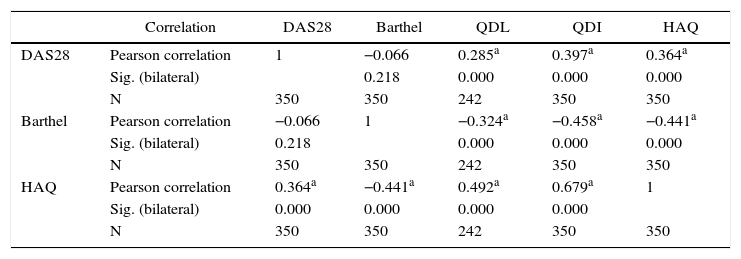
The analysis of bivariate correlation between the level of disease activity and its relationship with the functionality scales is shown in Table 5.
Correlation between the level of activity (DAS28) and functionality scales (n=350).
| Correlation | DAS28 | Barthel | QDL | QDI | HAQ | |
|---|---|---|---|---|---|---|
| DAS28 | Pearson correlation | 1 | −0.066 | 0.285a | 0.397a | 0.364a |
| Sig. (bilateral) | 0.218 | 0.000 | 0.000 | 0.000 | ||
| N | 350 | 350 | 242 | 350 | 350 | |
| Barthel | Pearson correlation | −0.066 | 1 | −0.324a | −0.458a | −0.441a |
| Sig. (bilateral) | 0.218 | 0.000 | 0.000 | 0.000 | ||
| N | 350 | 350 | 242 | 350 | 350 | |
| HAQ | Pearson correlation | 0.364a | −0.441a | 0.492a | 0.679a | 1 |
| Sig. (bilateral) | 0.000 | 0.000 | 0.000 | 0.000 | ||
| N | 350 | 350 | 242 | 350 | 350 |
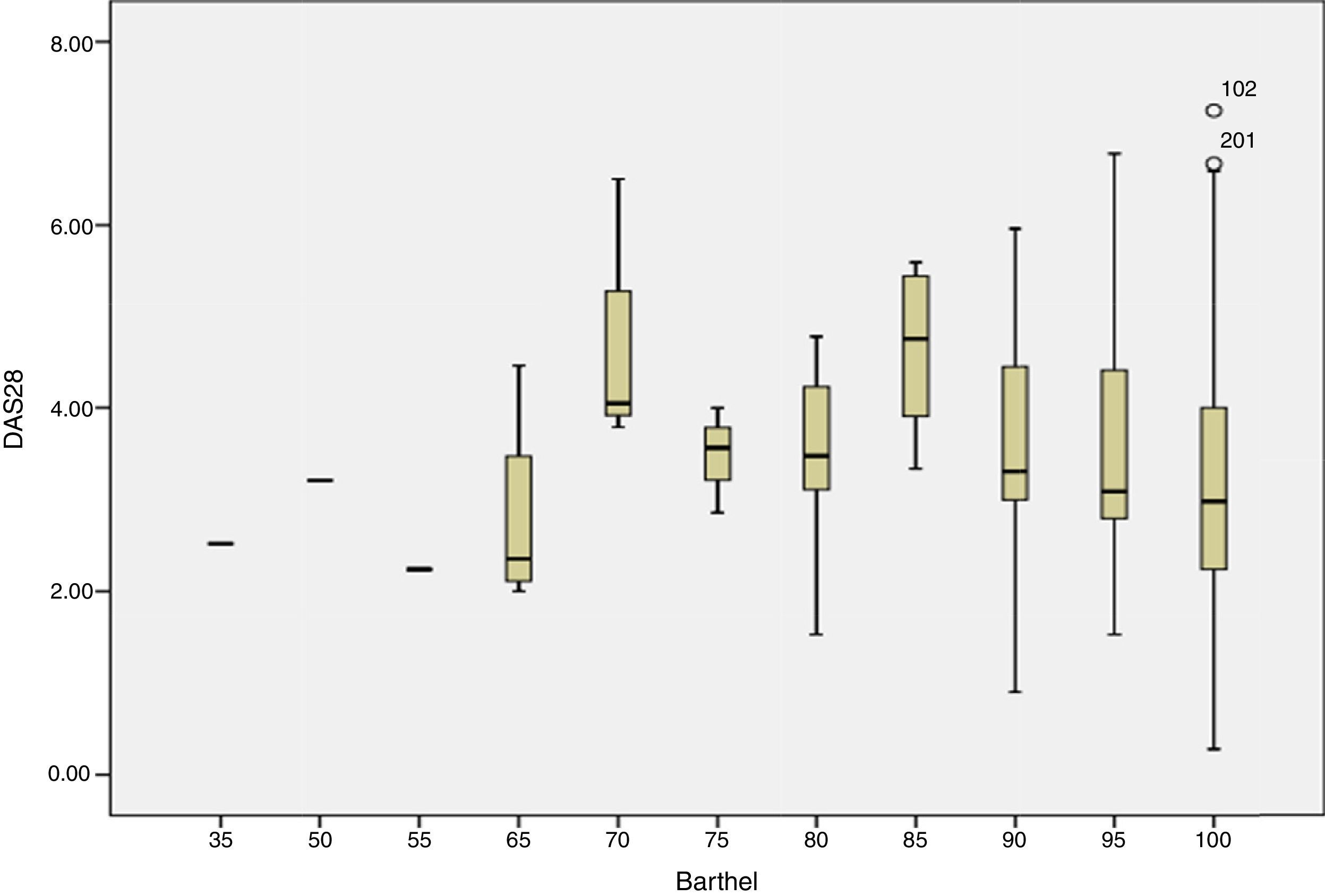
The Barthel index did not show a statistically significant association with the level of disease activity (Fig. 1).
Discussion and the Barthel index.")
This study is a first approximation to the functional impact of a group of patients, treated in a reference center specialized in rheumatologic diseases in Colombia (Riesgo de Fractura S. A.-CAYRE), under treatment with different biological therapies. The analysis of the data about the level of disease activity and the scales used for the evaluation of the functional impact allowed to establish statistically significant correlations.
The inclusion of patients under treatment with biological therapy, without differentiating the use of other therapies, as well as the non-differentiation of patients with disability secondary to sequelae states of the disease or derived from other diseases are limitations of the present study.
The results of the present study are comparable to those presented in 2009 by Radner et al., in Austria,18 in which is reported an average level of disease activity by DAS28 of 3.2±1.2 and an average of the functional assessment measured with HAQ of 0.81±0.76, compared with those reported in this study which were of 3.2 and 0.83, respectively. The population evaluated showed similar characteristics in the sample size and the type of therapy received was not considered. Similar values are presented in a study that evaluated the labor productivity,19 with an average HAQ of 0.87 and DAS28 of 4.
In relation to the disease activity and the impact that it generates on functionality, the study of the remission in rheumatoid arthritis conducted by Radner et al.18 identifies a behavior directly proportional between the 2 variables, similar to that found in the present study for the subjects with high and moderate disease activity. It is not like this for the cases of low activity (0.62) and in remission (0.65), which differ from what was reported in other studies.
The average value of the HAQ in this study was 0.83, lower than the reported in other studies. One of them, conducted in Colombia in 2004, was focused on the evaluation of sociodemographic variables, disability and pain, and it did not consider the type of pharmacological management. This study reported an average HAQ of 2.08 without taking into consideration the time of evolution or the type of therapy received.20 The subjects included in the present study, under treatment with biological therapy, have a lower impact on their functionality (HAQ 0.83), if compared with the reported in studies of patients refractory to treatment with modifying drugs, previous to the start of anti-TNF biological therapy (like the one developed in CAYRE between 2009 and 2011, with an average HAQ of 1.07,21 and the one developed in the Military Hospital in 2009, with an average HAQ of 1.2).22 It can be inferred that the advent of biological therapy and the approach in comprehensive programs allow to limit the impact of the disease on functionality.
When estimating the impact of the disease on labor productivity, it was found that in the working population with formal link and remunerated work (operational and administrative) the average HAQ was 0.75, with a level of disease activity of 3.23, similar to the reported in the study of prediction of the work disability developed in the Institute of Psychophysical Rehabilitation of Buenos Aires (Argentina), which reported an HAQ of 0.73, with a level of disease activity of 2.3±1.2.23
The use of instruments that allow the objective quantification of the degree of disease activity, the impact on the functionality and the quality of life is widely accepted; however, they should be specific and sensitive to the parameters monitored in the follow-up of the disease and in the response to treatment.
This study has allowed to re-evaluate the application within the program of generic scales that address in a general manner the functionality, as is the case of the Barthel index, which showed poor correlation with the disease activity, indicating an independent behavior between the activity found and the level of functional independence reported with this scale.
Likewise, although the Quick DASH scale addresses the gross motor function of the upper limb, it does not contemplate specific alterations in patients with rheumatic hand. In addition, it was found that subjects with a low activity level or in remission exhibited high scores in the Quick DASH, which may be related to uncontrolled variables, such as sequelae of the disease, comorbidities, increased perception of the limitation or secondary gain.
This study allowed to make an approximation for the evaluation of the general functionality of a population with RA and to assess its correlation, complying in this way its objective, results that are not generalizable to all patients with RA. In second phase of this project, and after the implementation of the changes in the scales suggested by this evaluation, we aim to create association or prediction models that include all demographic and clinical variables that could affect the outcome variable.
Undoubtedly, the care of the patients with RA requires an interdisciplinary approach that allows to integrate the advances in the pharmacological control of the disease, with the evaluation and management in a context of rehabilitation aimed to anticipate, limit and address the disability, through actions planned by a team of healthcare professionals experts in this disease.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingRiesgo de Fractura S. A.-CAYRE.
Conflict of interestNone for this work by any of the researchers.
To all members of the PARATI team for making possible this work.
Please cite this article as: Castro SM, Moya AM, Mora LM, Cardona C, Cuartas EA, Urrego YA. Aproximación de discapacidad en artritis reumatoide. Resultados de un programa de atención integral. Rev Colomb Reumatol. 2017;24:138–144.
