




To determine the effect of the ``Caring for caregivers®'' program on the care ability of family caregivers of people with rheumatoid arthritis in a health service provider institution in the city of Barranquilla.
MethodologyPre-experimental quantitative study, with pre-test-post-test design with a group. The sample consisted of 40 family caregivers. A characterisation card of the pair caregiver-person with chronic illness was used for the sociodemographic profile of the caregiver, as well as the Care Skill Inventory (CAI) before starting the program and after finishing. An analysis was made from descriptive statistics and measures of central tendency, in order to determine the profile of the caregivers in the dimensions: knowledge, value, and patience, and in the care ability. Inferential tests were used.
ResultsThe family caregivers of people with rheumatoid arthritis are mostly women, married or in free union, home occupation, and of low socioeconomic strata. The implementation of the ``Caring for caregivers®'' program had an effect on the care ability of family caregivers, as reported in different studies. It was identified that knowledge and value increased significantly, while the patience component showed a slight change.
ConclusionsThe ``Caring for caregivers®'' program had an effect on the ability to care. Intervention should be considered as an initiative in the development of care ability in caregivers of people with rheumatoid arthritis.
Determinar el efecto del programa «Cuidando a los cuidadores®» sobre la habilidad de cuidado de los cuidadores familiares de personas con artritis reumatoide en una institución prestadora de servicios de salud de la ciudad de Barranquilla.
MetodologíaEstudio cuantitativo pre-experimental, con diseño pretest-postest con un grupo. La muestra se constituyó con 40 cuidadores familiares. Se usó una ficha de caracterización de la díada cuidador-persona con enfermedad crónica para la caracterización sociodemográfica del cuidador y el Inventario de habilidad de cuidado (Care Skill Inventory [CAI]) antes de iniciar el programa y luego de finalizar. Se realizó un análisis a partir de estadística descriptiva y medidas de tendencia central, con el fin de conocer el perfil de los cuidadores, en las dimensiones: conocimiento, valor y paciencia, y en la habilidad de cuidado. Se usaron pruebas inferenciales.
ResultadosLos cuidadores familiares de personas con artritis reumatoide en su mayoría son mujeres, casadas o en unión libre, ocupación hogar, de estratos socioeconómicos bajos. La realización del programa «Cuidando a los cuidadores®» tuvo un efecto sobre la habilidad de cuidado de los cuidadores familiares, como se ha reportado en diferentes estudios. Se identificó que el conocimiento y el valor aumentaron de manera significativa, mientras que el componente paciencia presentó un ligero cambio.
ConclusionesEl programa «Cuidando a los cuidadores®» tuvo un efecto sobre la habilidad de cuidado; se debe considerar la intervención como una iniciativa en el desarrollo de la habilidad de cuidado en cuidadores de personas con artritis reumatoide.
Chronic noncommunicable diseases (CNCDs) are characterized by long duration and they usually evolve slowly. According to the World Health Organization, the CNCDs continue to increase worldwide and are the leading cause of premature death and disability in the vast majority of countries in Latin America and the Caribbean.1
Rheumatoid arthritis (RA) is a chronic, autoimmune disease, characterized by a strong impact on the functionality of people due to the inflammatory activity it generates on the joints;2 it affects approximately 1% of the adult population worldwide and is more frequent in women, with a 3:1 ratio.3 Some epidemiological studies in Latin America, such as in Argentina and Brazil, report a prevalence of 0.9 and 0.45%, respectively.4,5 Díaz-Rojas et al.6 report 267,628 prevalent cases in the year 2005 in Colombia: the global prevalence or RA corresponded to 0.9/100 inhabitants, the female/male ratio of RA was 4:1 and a progressive increase with age was observed (peak in the group over 80 years of age).
RA is a public health problem across the world due to systemic involvement, its serious functional consequences and the high economic and social impact. The costs associated with this disease can be direct, indirect and even very difficult to determine.7 In Colombia, RA is identified as a high-cost pathology according to resolutions 2565 of 20078 and 3974 of 2009,9 of the Ministry of Health and Social Protection.
All this affectation causes in the individual work disability and deterioration of quality of life, requiring a family caregiver who also is subjected to modify his/her social and family lifestyle, abandoning part of his/her life because of the commitment he/she acquires and his/her life revolves around the care of the sick person.10 It is for this reason that Barrera et al.11 study the care ability to highlight the importance that the labor of caring at home represents, especially when is carried out by family caregivers. This phenomenon of the ability to care of family caregivers of people with chronic diseases such as RA has been little studied.
The results obtained in previous research motivated Barrera, Pinto and Sánchez12 to develop and validate the «Caring for caregivers®» program under the conceptual guidelines of Ngozy Nkongho,13 with the purpose of strengthening the care skills of the family caregivers of relatives with chronic illnesses.
The effectiveness of the program has been evaluated in several cities in Colombia and in some Latin American countries, where it was shown that the sample group of family caregivers who participated in the program improved their care ability significantly, with an increase in all dimensions that make up this ability (knowledge, value and patience) compared to the control group.14,15
MethodologyThe study was conducted in the Hospital Universidad del Norte, in the city of Barranquilla, in the year 2017 with 40 family caregivers of people with RA treated in this institution. The design was pre-experimental of pre-test-post-test with one group.
It was taken a convenience «subject type» sample of 40 caregivers. Once the results preliminary to the intervention in these caregivers were obtained, the final sample size was calculated using the following expressions, resulting in 40 caregivers, so the complete sample was allowed with the initial 40 caregivers:
Where the pre-test and post-test variation was 12.5%.



The participants in the rheumatology consultation that accompanied their relative with RA were located for the application of the instruments and the intervention, the objective of the research was explained to them, the informed consent process was carried out and the participation was voluntary.
The intervention was done in one day with an intensity of 8 h to ensure that the participants receive it without loss of follow-up. Likewise, financial support was provided for transportation, lunch and snacks during the day, taking into account that not all caregivers were located in the urban area. The following inclusion criteria were taking into account: a) caregiver of a person with RA who attends rheumatological consultations with a level of dependence; b) older than 18 years; c) person with a family bond of kinship or closeness with the person being cared for; d) level of functionality of the person being cared for with a score ≥ 9 in the PULSES profile; e) family caregiver affiliated to a Health Care Promoting Office ("EPS" - Entidad Prestadora de Salud), and f) knowing how to read and write or guaranteeing the self-completion of the instruments.
As exclusion criteria were considered: a) family caregivers with cognitive deficit or previously diagnosed neurological or mental disorders, and b) caregivers who during the interview were under the effect of drugs or substances that would limit their communication skills.
For the measurement of the dependent variable of the study, the care skill, an initial (pre-test) and final (post-test) tests were applied using the Care Skill Inventory (CAI) (Annex), with permission of the author, before and after the «Caring for caregivers®» program. The Inventory proposes the need for care for human survival through its 37 points with a Likert-type graduation rated from 1 to 7 and consists of 3 subscales: knowledge, value and patience. The responses to the items are added for each subscale, giving a total score for each one. The highest scores indicate a greater degree of care if the item is presented positively; the score is the opposite if the item is presented negatively. The knowledge subscale consists of 14 items; the one of value, of 13 items, and that of patience, of 10 items. The reliability reported by the author for the instrument is 0.84 and the validity is 0.80.13 It has an official Spanish translation and semantic tuning for the Colombian context. The Spanish version reported a Cronbach's alpha of 0.86 and a Pearson correlation coefficient of 0.66, showing a considerable correlation between its dimensions.16
In addition, the first dimension (identification of the conditions and the demographic profile of the caregiver) of the Characterization Card of the Dyad Caregiver-Person with Chronic Illness GCPC-UN-D of the National University of Colombia was applied.17
The PULSES profile was used to perform the functional assessment of the recipient. This profile allows to measure the degree of dependence of a person, and consists of a nominal measurement scale of 6 parameters with possible values of 1–4 for each parameter, where 1 represents the absence of functional limitation and 4 the greatest functional limitation. Each parameter measures a particular aspect of functionality; Thus, the parameter P (Physical condition) assesses the degree of stability of the pathology examined by the amount of supervision by health professionals that the patient requires on a regular basis; the parameter U (Upper limb function) assesses the function of the upper limbs and reflects the need for assistance for the self-care actions, such as eating, drinking, dressing, grooming, etc.; the parameter L (Lower limb function) assesses the functionality of the lower limbs and is related to mobility and displacement; the parameter S (Sensory components) assesses the sensory function, sight, hearing and the communication skills; the parameter E (Excretory functions) assesses the sphincter control and points out the need for assistance in these functions; finally, the parameter S (Support) examines the psychological, social, family, etc. factors of support the patient has, and therefore indicates the need to provide assistance related to social and psychological difficulties. The instrument establishes that a score of 6 indicates the presence of total independence; an increase in the score corresponds to an increase in dependence of the patient, and a score of 24 indicates total dependence. The interpretation by ranges establishes that a final score between 6 and 8 indicates a preserved functional level, between 9 and 11 indicates a slight commitment of functionality, and scores equal to or greater than 12 identify cases of severe commitment of functionality with a high degree of dependence.18 It has been documented that the less functionality, the greater the burden and feelings of depression in the caregivers.19 Therefore, knowing the level of functionality is having a clear picture of the difficulties or opportunities that caregivers have in care.20
The independent variable, intervention to modify the care ability of family caregivers for the study group, was cognitive behavioral and guided by principles of care; it consisted in the development of the "Caring for caregivers®" program, abbreviated version.21
The program has 3 modules: the module I, to strengthen knowledge, recognizes the experience of giving and receiving care and identifies potentialities and weaknesses in the care work; the module II, to strengthen the value, recognizes the process of decision making in care, the social ability, the social support and the empowerment of the caregiver; the module III, of patience, begins with the identification of what makes the caregiver impatient and what reassures him/her; then reviews how to work patience through the meaning that characterizes each caregiver, setting goals for the care of him/herself and his/her relative.21
As a strategy to avoid bias in the administration of tests, it was controlled through previous training in the «Caring for caregivers®» program, at the National Cancer Institute (INC, Instituto Nacional de Cancerología) for the development of the ability to manage the program and the instruments and to interview the individuals who voluntarily wished to participate in the study. It is possible that several sources of internal invalidation act, which have been described by Campbell as the history and the maturation22; and for this reason the applications of the pre-test and the post-test to the family caregivers of individuals with RA were conducted on the same day.
Taking into account the ethical aspects contemplated in Resolution 8430 of 1993,23 this research applied within the category of minimum risk, since the proposed intervention was educational and, therefore, it did not represent a risk for the integrity of the people who participated in the research. The principle of autonomy was respected, using the written informed consent and the wish to withdraw at any time during the course of the study. The research had the endorsement number 054-16 of the Ethics Committee of the Faculty of Nursing of the National University of Colombia, the endorsement of the institution in Barranquilla where the data was collected and the authorization for the application of the instruments chosen for the study.
The completed forms were filed listed by family caregiver along with the informed consent, and were digitized in a database in Excel for greater ease during the analysis.
The data analysis started from the delimitation of the sample by the Stein’s sampling principle in two stages. Then the analysis was performed in two phases:
- a)
Descriptive analysis. A description of the family caregivers was made in the intervention group and in the dimensions: knowledge, value and patience, and in the ability to care, taking into account quantitative variables (proportions, percentage, frequency distributions and measures of central tendency, dispersion and concentration).
- b)
b) Inferential analysis. In order to evaluate the changes generated through the intervention, inferential tests were used depending on the management of the data. These tests allowed us to contrast the hypothesis between the variances and the means of the groups.
The probability of type I error of 0.05 was assumed for all purposes of decision-making. All these calculations were performed using the SPSS program version 22.
ResultsSociodemographic profileIt was found that 87.5% of caregivers were women. The average age was 46.4 years, with a standard deviation of 12.1; the minimum age was 19 years, and the maximum age was 80 years. Those of 41–60 years prevail in the age range. As for the level of schooling, most of them have incomplete and complete high school, and the existence of the university level is notorious. For the department of origin, stands out the Atlantico, with 80%, and the place of residence of the caregivers is Barranquilla, with 77%; regarding the dwelling area, the majority is urban, with 92.5% (Table 1).
Sociodemographic characterization of the family caregivers of people with rheumatoid arthritis.
| Variable, n = 40 | Frequency | Proportion |
|---|---|---|
| [0,1–3]Gender | ||
| Male | 5 | 12,5% |
| Female | 35 | 87,5% |
| [0,1–3] | ||
| [0,1–3]Agea | ||
| 18 to 30 years | 4 | 10% |
| 31 to 40 years | 9 | 22.5% |
| 41 to 50 years | 11 | 27.5% |
| 51 to 60 years | 12 | 30% |
| 61 or more years | 4 | 10% |
| [0,1–3] | ||
| [0,1–3]Level of schooling | ||
| Complete primary | 6 | 15% |
| Incomplete secondary | 12 | 30% |
| Complete secondary | 11 | 27.5% |
| Technician - technologist | 2 | 5% |
| University | 9 | 22.5% |
| [0,1–3] | ||
| [0,1–3]Departament of origin | ||
| Atlántico | 32 | 80% |
| Bolívar | 3 | 7.5% |
| Guajira | 1 | 2.5% |
| Magdalena | 2 | 5.0% |
| Sucre | 1 | 2.5% |
| Córdoba | 1 | 2.5% |
| [0,1–3] | ||
| [0,1–3]Place of residence | ||
| Barranquilla | 31 | 77.5% |
| Soledad | 6 | 15.0% |
| Malambo | 2 | 5.0% |
| Santo Tomás | 1 | 2.5% |
| [0,1–3] | ||
| [0,1–3]Dwelling area | ||
| Rural | 3 | 7.5% |
| Urban | 37 | 92.5% |
| [0,1–3] | ||
| [0,1–3]Marital status | ||
| Single | 8 | 20% |
| Married | 17 | 42.5% |
| Separated | 3 | 7.5% |
| Widower | 3 | 7.5% |
| Free union | 9 | 22.5% |
| [0,1–3] | ||
| [0,1–3]Occupation | ||
| Housekeeping | 17 | 42.5% |
| Employee | 9 | 22.5% |
| Independent work | 8 | 20% |
| Student | 3 | 7.5% |
| Pensioner | 3 | 7.5% |
| [0,1–3] | ||
| [0,1–3]Socioeconomic strata | ||
| One | 11 | 27.5% |
| Two | 21 | 52.5% |
| Three | 6 | 15% |
| Four | 2 | 5% |
| [0,1–3] | ||
| [0,1–3]Caregiver since diagnosis | ||
| Yes | 33 | 82.5% |
| No | 7 | 17.5% |
| [0,1–3] | ||
| [0,1–3]Religion | ||
| Catholic | 25 | 62.5% |
| Christian | 13 | 32.5% |
| Atheist | 2 | 5% |
| [0,1–3] | ||
| [0,1–3]Level of religious commitment | ||
| High | 20 | 50% |
| Medium | 17 | 42.5% |
| Low | 3 | 7.5% |
Source: research data.
In terms of marital status, a high percentage has a stable partner (married and free union), with 65%, which shows a close support. Within the occupation, most caregivers respond to housekeeping, with 42.5%, employee, with 22.5%, and independent work, with 20%. The majority of caregivers respond that their home is located in a low socioeconomic stratum (stratum 1 and 2), with percentages around 80%. 82.5% of caregivers are in charge of their relative from the time of diagnosis. In the findings, the predominant religions are Catholic, with 62.5%, and a high-medium level of commitment, with percentages of 92.5% (Table 1).
Ability to careIn the ability to care, values between 137 and 250 points were obtained at the beginning of the intervention, with a mean of 195.20 and a standard deviation of 29.93. The frequency distribution of the initial ability showed a marked symmetry, since the asymmetry coefficient is very close to zero (−0.064). After the intervention, the ability to care was present in values between 187 and 251, with a mean of 215.02 and a standard deviation of 19.40; it also showed a symmetry (0.197) (Table 2).
Ability to care of the family caregivers of people with rheumatoid arthritis before and after intervention. Data by dimensions.
| Dimensions | Time of measurement | Mean | Standard deviation | Median | Asymmetry | Asymmetry standard error | Minimum | Maximum | p-valuea |
|---|---|---|---|---|---|---|---|---|---|
| Total abilty | Before | 195.20 | 29.93 | 190 | −0.064 | .374 | 137 | 250 | .066 |
| n = 40 | After | 215.02 | 19.40 | 212 | 197 | .374 | 182 | 251 | |
| Knowledge | Before | 77.12 | 12.88 | 79 | −593 | .374 | 46 | 98 | .202 |
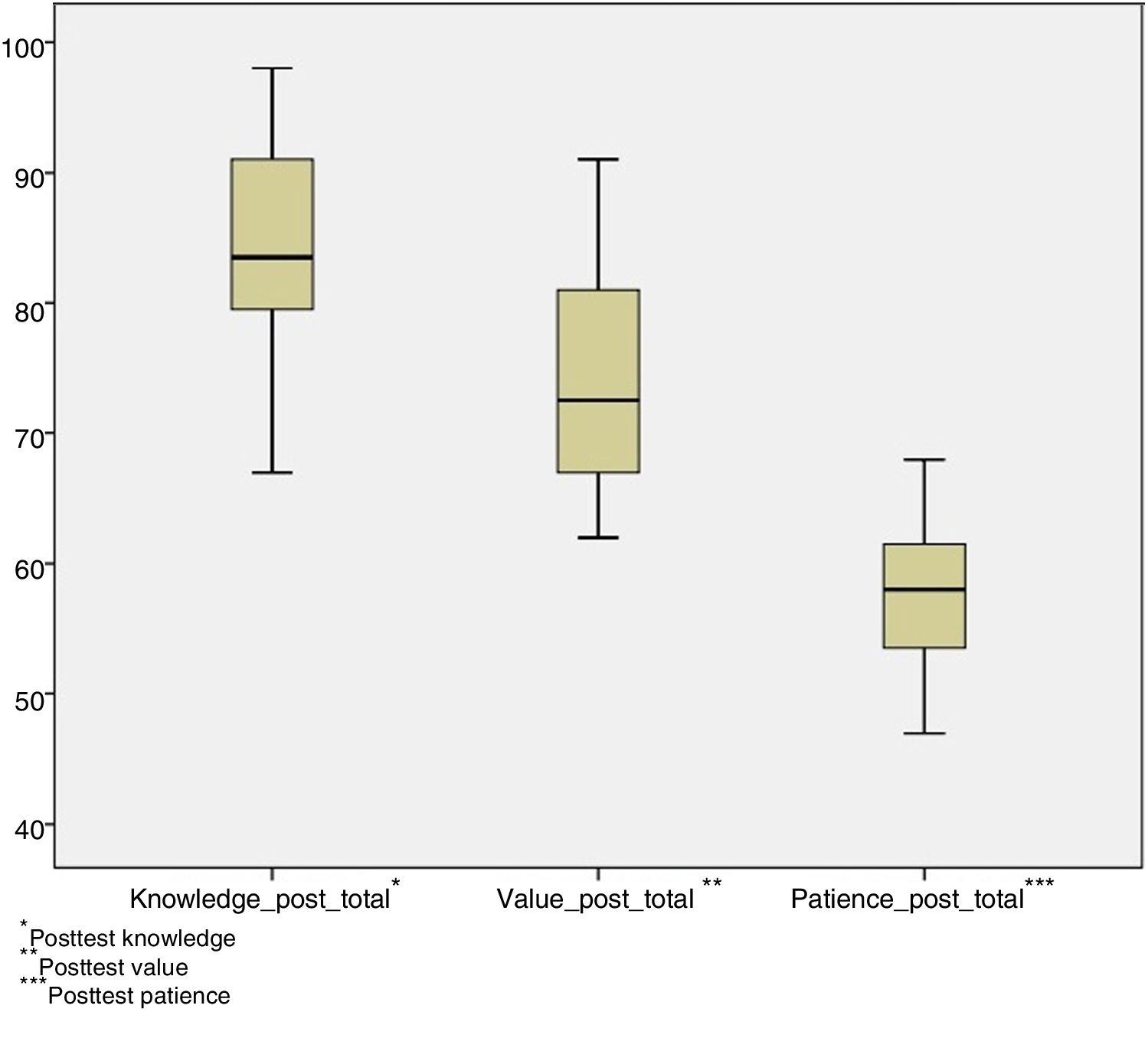
| n = 40 | After | 83.97 | 7.54 | 83 | −196 | .374 | 67 | 98 | |
| Value | Before | 63.27 | 14.13 | 64 | −097 | .374 | 38 | 91 | .092 |
| n = 40 | After | 73.62 | 8.09 | 72 | −196 | .374 | 62 | 91 | |
| Patience | Before | 54.80 | 7.42 | 56 | −643 | .374 | 38 | 68 | .034 |
| n = 40 | After | 57.42 | 5.45 | 58 | −115 | .374 | 47 | 68 |
Source: research data.
The knowledge dimension, before the intervention, showed a mean of 77.12, a standard deviation of 12.88, a minimum value of 46 and a maximum value of 98 and its asymmetry coefficient was −0.593. Once the intervention was developed, this dimension showed a mean of 83.97, a standard deviation of 7.54, a minimum value of 67 and a maximum value of 98 and its asymmetry coefficient was −0.196 (Table 2).
The value, as the second dimension of the instrument of ability to care, initially reports values between 38 and 91 points, with a mean of 63.27, a standard deviation of 14.13, and its asymmetry coefficient is −0.097. After the program, values between 62 and 91 were obtained, with a mean of 73.62, a standard deviation of 8.09, and its asymmetry coefficient was −0.196 (Table 2).
The third dimension, which is patience, previously had a mean of 54.80, with a median of 56, a minimum value of 38 and a maximum value of 68 and its symmetry marks −0.643. After the intervention, it obtains a mean of 57.42, with a median of 58, a minimum value of 47 and a maximum value of 68; and its symmetry marks −0.115 (Table 2).
In the analysis by dimensions of the care ability of family caregivers before and after the intervention, it was identified that the knowledge and value increased significantly, while the patience component presented a slight representative change between the initial and final measurements (Figs. 1 and 2).
Results of the effect of the intervention

According to the Wilcoxon signed test, the results of total ability to care, in the dimensions of knowledge, value and patience, have a p-value of zero (<0.001), which allows us to reject the null hypothesis that considers: the application of the «Caring for caregivers ®» program has no effect on the ability to care of the family caregivers of individuals with RA, which allows to state that the program has an effect on the ability to care according to the perception of the family caregivers.
DiscussionIn the sociodemographic characteristics of the family caregivers of people with RA it was found a greater proportion of women, which can be explained because in the Colombian context, the woman usually assumes the role of caregiver of the chronic patients in the family and due to the historical delegation of the tasks of care to the women.24–27
As for the age, the range that prevailed was between 41 and 60 years, unlike what was found by Carreño et al.,28 where the age ranged between 18 and 59 years, evidencing caregivers in the productive age as a characteristic.
The levels of schooling were found between the complete and incomplete secondary education, not higher than high school, which responds to what was evidenced by Carrillo et al.29 compared with the medium and low levels of schooling in the family caregivers of individuals with chronic disease.
It is evident that the majority of family caregivers were married or in free union, similar to what was reported by Ávila et al.30 This could be a factor that influences the caregivers over 41 years, being an emotional support, coping and relief in some care situations.
In relation to the occupation, the majority of caregivers are devoted to housekeeping, similarly to what was found by Chaparro et al.,31 which implies an increase in the requests to the health and social welfare regimes, by reducing productivity and thus having a negative effect on the economy of the families.
The participating family caregivers are characterized by having a low socioeconomic situation, analogous to what was evidenced by Carrillo et al.26; the caregivers in the Caribbean region belong to socioeconomic strata 1 and 2, which shows the condition of social vulnerability in the northern region of the country. According to the study conducted by Gómez and Gómez32 it can be inferred that people with RA with a low socioeconomic status may present a situation that worsens the disease, the physical health, the mental health and the quality of life, which can represent a change in the care ability of caregivers.
The family has always been the first agent of care for the individuals with chronic disease, and this causes a change in the family dynamics, where a family member will take the role of caregiver at the onset of the disease or will be replaced by another member. In this study the majority of caregivers have been the first caregivers since the diagnosis, something similar to what was found by Chaparro.33 Therefore, it can be stated that the caregiver can get to know the person he/she cares because he/she has more continuity of the process; in addition, he/she will be able to discover his/her care experience, strengthening his/her caregiver role, ability to care and quality of life.
The ability to care with the approach of Ngozi O. Nkongho13 shows that the dimensions knowledge, value and patience are central axes to understand the meaning of ability to care with the perspective of caregivers.
With respect to the ability to care, this study shows an increase. These findings are similar to those found in other studies34–37 with a formal intervention, but no studies have been found yet in family caregivers of people with RA.
In the dimensions of knowledge, value and patience there is an increase, unlike what was reported by Carrillo et al.,38 where the components of knowledge and patience showed an increase, while the dimension of value remained the same in the groups, with a slight increase in the control group, although not statistically significant.
It should be considered that the deterioration characteristic of the chronicity experienced by the individuals cared for can affect the total ability to care of their caregivers; the dimension of patience presented a slight increase with respect to the baseline condition, which could suggest the need to continue studying psychosocial aspects that influence the experience of the caregiver. Taking into account that the phenomenon of ability to care is multidimensional, maintaining it can also be understood as an achievement.
In summary, the results presented in this research allowed the fulfillment of the proposed objectives, and after proven the hypotheses raised on the effect of the «Caring for caregivers ®» program with a significance level of p = 0.000, the null hypothesis is rejected and is established that the «Caring for caregivers ®» program has an effect on the ability to care of the family caregivers.
The results found in this study evidenced the effectiveness of the «Caring for caregivers ®» program, similar to the studies conducted by Barrera et al.,14,15 in which a significant increase in the ability to care was reported. Unlike the dimensions, in the research carried out by Barrera et al.14 only the study group increased the level of the knowledge component. With respect to the patience component, it was found a decrease in the control group and an increase in the study group. At the end of the intervention, the total ability and the patience component had a statistically significant difference between the groups, being better the result of the study group. The other study conducted by Barrera et al.15 shows a strengthening or the ability to care of the caregivers in general and in each of its components favorable to the program. In contrast with a research conducted by Díaz et al.,39 it evidenced the effectiveness of the program for the dimensions of knowledge and patience in the experimental group, while the dimension of value remained unmodifiable both in the control and the experimental groups.
LimitationsAlthough the final sample was determined from statistical data where the pre-test and post-test variation was 12.5%, the sample could have been increased to perform other types of inferential tests such as Cohen's; however, difficulties were encountered at the time of the search for patients with RA who had a compromised level of functionality, and therefore, there was a decrease in family caregivers in the institution where the study was conducted.
ConclusionsThe ability to care of family caregivers of people with RA in a health service provider institution in the city of Barranquilla is a phenomenon that should continue to be studied in order to prove the effectiveness of the program not only in the shortened version but also in the complete program to benefit a larger population. In this way, the study of the ability to care constitutes a contribution to the implementation of programs that promote the health and well-being of caregivers.
It is recommended to continue and strengthen the work as part of the Latin American Network of the patient with CNCD in the follow-up of the long-term effect of the «Caring for caregivers ®» program and to continue the validation process of the Care Skill Inventory (CAI) (Annex), defining its psychometric properties, for our Colombian population, Also, to propose the creation of the Program in the healthcare institutions as a social and research commitment in nursing.
FundingOwn resources.
Conflict of interestThe authors declare they have not any conflict of interest.
To the Hospital Universidad del Norte and all the family caregivers who accepted to participate in this study.
The following are Supplementary data to this article:
Please cite this article as: Agudelo DD, Ramírez OJG. Efecto del programa «Cuidando a los cuidadores®» en cuidadores familiares de personas con artritis reumatoide. Rev Colomb Reumatol. 2019;26:177–184.
