



Ultrasound (US) abnormalities have often been described in the joints of asymptomatic subjects, which may lead to uncertainty in the evaluation and treatment of inflammatory joint disease. Despite this, the available evidence is scarce, with few participants, and in the vast majority with transducers less than 18 Mhz. In Colombia there are currently no published studies about this topic.
ObjectivesTo describe the ultrasound findings in hand and foot joints in asymptomatic volunteers, their association with sociodemographic characteristics, and intra- and interobserver concordance of the measurements.
Materials and methodsDescriptive and analytical study within 182 asymptomatic volunteers. Two physicians with musculoskeletal ultrasound experience evaluated the dorsal aspect of 5460 articular recesses using the semi-quantitative scale of Szkudlarek using an 18 MHz linear transducer.
ResultsThe median age of the participants was 42 years, including 60.4% women. A total of 232 abnormal findings were identified in 87% of the volunteers, with 68.1% corresponding to joint effusion, 29.3% synovial hypertrophy, 2.1% erosions, and 0.4% positive power Doppler. The feet evaluation showed more findings than the hands (70.7 vs. 29.3%). The joints in which most abnormalities were identified were the first metatarsophalangeal joint (52%), third metatarsophalangeal joint (15%), and radiocarpal joint (9.5%). A positive association was found between joint effusion and synovial hypertrophy with age, exclusive manual activity, and occupation for more than ten years. The intra-observer concordance was moderate (Kappa = .4591) and the inter-observer was low (Kappa = .2155).
ConclusionsThe absence of power Doppler signal, the absence of abnormalities in distal radioulnar, the absence of synovitis accompanied by erosion, and a greater predominance of mild alterations in the hand joints, added to the absence of findings in the fifth metatarsal joint, can be potential specific findings of asymptomatic subjects and might be confirmed in future studies.
Anormalidades ultrasonográficas se describen con cierta frecuencia en articulaciones de sujetos asintomáticos, las cuales generan incertidumbre en el contexto de evaluación y tratamiento de la enfermedad articular inflamatoria; a pesar de ello, en Colombia no existen estudios al respecto y la evidencia disponible es escasa, hecha en un bajo número de participantes y con transductores menores a 18 MHz en su gran mayoría.
ObjetivosDescribir los hallazgos ultrasonográficos articulares en manos y pies de un grupo de voluntarios asintomáticos, su asociación con las características sociodemográficas y la concordancia intra e interobservador de sus mediciones.
Materiales y métodosEstudio descriptivo y analítico en el que se incluyeron 182 voluntarios asintomáticos. Dos médicos con experiencia en ecografía musculoesquelética evaluaron el aspecto dorsal de 5.460 recesos articulares mediante la escala semicuantitativa de Szkudlarek y la utilización de un transductor lineal de 18 MHz.
ResultadosLa mediana de edad de los participantes fue de 42 años, 60,4% de ellos mujeres. En 87% de los voluntarios se identificaron en total 232 hallazgos, el 68,1% correspondió a derrame articular, 29,3% a hipertrofia sinovial, 2,1% a erosiones y 0,4% a Doppler de poder. Los pies mostraron mayores hallazgos que las manos (70,7% vs. 29,3%). Las articulaciones en las que más se identificaron anormalidades fueron la primera articulación metatarsofalángica (52%), la tercera metatarsofalángica (15%) y la radiocarpiana (9,5%). Se halló relación positiva entre el derrame articular y la hipertrofia sinovial con la edad, ocupación manual exclusiva y tiempo laboral mayor de 10 años. La concordancia intraobservador fue moderada (Kappa = 0,4591) y la interobservador fue leve (Kappa = 0,2155).
ConclusionesLa ausencia de señal Doppler de poder, el no compromiso radioulnar distal, la ausencia de sinovitis acompañada de erosión y una mayor predominancia de alteraciones leves al nivel de las manos, sumado a la ausencia de hallazgos al nivel de la quinta articulación metatarsiana, constituyen hallazgos potencialmente específicos de sujetos asintomáticos que merecen ser confirmados como tal en futuros estudios.
In the field of rheumatology, musculoskeletal ultrasound continues gaining a growing interest not only because it is a non-invasive, low-cost exam, without contraindications and without exposure to radiation, but also because it has proven to be more sensitive than clinical evaluation to detect synovitis and predict relapses and structural damage.1–3 In addition, its better performance in the early detection of bone erosions compared with conventional radiography, and its equivalence in the identification of synovitis with respect to magnetic resonance, further ratify at the patient's bedside its importance in the diagnosis, treatment and follow-up of the different rheumatic diseases.4,5
There are multiple studies to date, especially with regard to the early diagnosis and monitoring of the response to treatment in rheumatoid arthritis, and for this it has been imperative a correct characterization and standardization of the different ultrasonographic abnormalities.6–10 This is how the Outcomes Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) working group, in 2005, defined and standardized in detail these findings in rheumatoid arthritis, and since then, after periodic updates is the reference standard in the different clinical studies.11,12
After the advent of new equipment with better image resolution, ultrasonographic abnormalities such as synovial hypertrophy, power Doppler signal, bone erosions and joint effusion have also been documented in 9%, 11%, 18% and 52%, respectively, of subjects without a diagnosis of joint disease,13–16 thus putting at risk of classifying these findings as "pathological", and generating doubts when implementing the most appropriate therapeutic scheme, its adjustment and the interpretation of its response over time.
In our environment we do not have studies to date that have described the different ultrasound findings in joints of asymptomatic subjects and those conducted in Latin American population are scarce, with a low number of participants and mostly with transducers of frequencies lower than 18 MHz.13,17–21 In addition to this, the high prevalence of joint pain as a reason for consultation in rheumatology, and taking into account that rheumatoid arthritis is the most frequent autoimmune joint disease, reaffirms the importance of knowing that gap between joint normality and abnormality.
The objective of this study is to make a detailed description of the semi-quantitative ultrasound findings in the hand and foot joints of a group of asymptomatic volunteers, in order to determine the location and frequency of the different inflammatory and chronic lesions, and the possible association with their sociodemographic characteristics.
Materials and methodsParticipantsDescriptive, prospective and analytical study in which 182 volunteers without known joint disease, or abnormalities on the physical examination at the time of evaluation by a rheumatologist were included. The ages of the participants ranged between 20 and 80 years, and were stratified into 6 groups (20–30, 31–40, 41–50, 51–60, 61–70 and 71–80 years). In order to minimize the inclusion in the study of subjects with musculoskeletal disease, the potential participant was also interrogated in search of signs or symptoms indicative of "red flag", contemplated by the American College of Rheumatology.22 The participants were patients without a diagnosis of rheumatic disease or their accompanying relatives, administrative or healthcare staff, professors and students of the National University Hospital of Colombia and the National University of Colombia. Those with the presence of some "red flag", pregnancy, degenerative or inflammatory joint disease, autoimmune disease, history of septic arthritis, trauma or joint surgery and use of anti-inflammatory drugs in the last 24 h were excluded. Data on their age, height, weight, body mass index, occupation, cigarette smoking, working time, comorbidities, physical activity and dominant hand were collected. The regular physical activity was defined as that aerobic activity of moderate intensity for at least 150 min per week, or at least 75 min per week of intense physical activity. Regarding the occupation, the participants were grouped into 4 categories: a) exclusive manual: volunteers with significant manual handling of loads, such as those dedicated to the home (housewives), farmers, gardening, maintenance, plumbing, mechanic and general service workers; b) administrative: office and typing work mainly, such as secretaries, administrative, financial and accounting staff; c) intellectual: volunteers with very little manual handling of loads, such is the case of teaching and student staff; and, finally, d) a combination thereof.
Ultrasonographic assessmentThe sonographic evaluations were performed in the Department of Radiology and Diagnostic Imaging of the National University Hospital of Colombia by a radiologist with 25 years of experience in musculoskeletal ultrasonography. A B-mode and power Doppler articular ultrasonography was performed with a Toshiba Aplio 300 ultrasound system and using a high frequency linear transducer (18 MHz) in a room at constant temperature (20–23 °C) in the afternoon hours. The same equipment with the same configuration was used in all subjects. The joints considered by our service as the most relevant in daily clinical practice were selected and the joint spaces were evaluated in their dorsal aspects using standardized protocols.9,23 The carpal (distal radioulnar and radiocarpal joints), metacarpophalangeal (MCP) and 1–5 proximal interphalangeal (PIP) joints of the hands were studied. Likewise, the metatarsophalangeal (MTP) joints of the first, third and fifth toes were assessed. The volunteers were seated in a comfortable position, keeping their hands and feet resting in a neutral position. Warm water was used in sufficient amount as a medium of sound transmission, and the pressure exerted on the linear transducer for each evaluation was sufficient not to cause visible deformities of the intra-articular structures, avoiding to reduce the sensitivity for the detection of the blood flow or intraarticular fluid.
The presence of joint effusion, synovial hypertrophy, power Doppler signal and bone erosions was evaluated in each of the identified recesses, being categorized by the semi-quantitative scale of Szkudlarek.8 The referred system was used, since it clearly defines all the grades, it has an excellent interobserver variability, it has been correlated with other imaging modalities (MRI and conventional radiology) and accepted by the OMERACT expert consensus.11,12 The findings of the Szkudlarek scale are defined as follows: joint effusion—compressible anechoic intracapsular area (0: without effusion, 1: minimal amount of joint effusion, 2: moderate amount of joint effusion, without distension of the joint capsule and 3: extensive amount of joint effusion, with distension of the joint capsule)—; synovial hypertrophy: non-compressible hypoechoic intracapsular area (0: without synovial thickening, 1: minimal synovial thickening that fills the angle between the periarticular bones, without bulging on the line that links the upper parts of the bones, 2: synovial thickening with bulging in the line that links the upper parts of the periarticular bones, but without extension along the bone diaphysis and 3: synovial thickening that goes beyond the line that links the upper parts of the periarticular bones and with extension at least to one of the bone diaphysis); power Doppler signal: blood flow signal in the synovial membrane related to synovial hypertrophy (0: without flow, 1: single vessel signals, 2: confluent vessel signals in less than half of the area of the membrane and 3: vessel signals in more than half of the area of the membrane assessed), and finally, bone erosions were defined as changes in the bone surface of the area adjacent to the joint (0: regular bone surface, 1: irregularity of the bone surface without formation of a defect seen in 2 planes, 2: formation of a defect in the bone surface seen in 2 planes, and 3: bone defect that creates an extensive bone destruction). The definitions of normal joint and synovitis were finally made based on the EULAR-OMERACT combined scoring system recently obtained using the Delphi methodology.11,12
Complementarily, the incidental ultrasonographic findings at the level of the articular cartilage and the periarticular soft tissues other than those related to the Szkudlarek semi-quantitative system were recorded, and their potential association with the sociodemographic characteristics of the participating volunteers was also evaluated.
Finally, intra- and interobserver concordance was performed through a second review by an independent rheumatologist with 12 years of experience in musculoskeletal ultrasound and Professor of Professors EULAR 2015, to 10% of the static images stored in DICOM format.
Statistical analysisFor the descriptive analysis of the sociodemographic aspects and the ultrasonographic findings of the patients, absolute distributions, relative distributions and summary indicators such as quartiles, interquartile range, maximum values and minimum values were used. The criterion for normality of some sociodemographic and clinical variables was established by means of the Kolmogorov–Smirnov test.
The Chi square test of independence or Fisher's Exact test were applied to establish the relationship between the sociodemographic factors and the ultrasonographic findings. The Pearson correlation coefficient was used for the correlation between the sociodemographic aspects and the Szkudlarek semi-quantitative scores. The Mann-Whitney U test and the Kruskal-Wallis test were applied for the relationship between the sums of the semi-quantitative Szkudlarek scores and the sociodemographic aspects.
The intra- and interobserver agreement (concordance) for semi-quantitative measurements between the different evaluators was calculated using Cohen's Kappa index with their respective confidence intervals; a Kappa value from 0 to 0.20 was considered very poor, from 0.21 to 0.40 poor, from 0.41 to 0.61 moderate, from 0.61 to 0.80 good and a value greater than 0.81 excellent. A p-value < 0.05 was considered statistically significant. The systematization of the data was carried out using the RedCap software, a secure Web-based application designed for data capture in research studies. The data processing and analysis was performed using the Stata statistical software, version 15.
Ethical considerationsIn accordance with article 11 of Resolution 8430 of 1993 of the Ministry of Health, this study is classified as research with minimal risk, and was approved by the Ethics Committee of the National University Hospital of Colombia and the National University of Colombia (012-218-15).
ResultsCharacteristics of the patientsA total of 239 subjects were evaluated and 182 volunteers were finally included. 46 subjects were excluded from the study due to joint pain at the time of the examination and antecedent of osteoarthrosis (older than 55 years), gout (n = 2), psoriasis vulgaris (n = 2), amputation of fingers of the hand (n = 2), erythema nodosum (n = 1), monoarthritis of the knee under study (n = 1), articular surgery (n = 1), juvenile idiopathic arthritis (n = 1) and vitiligo associated with antiphospholipid syndrome (n = 1). Of the 182 volunteers there was loss of information in 2 cases; the first one was a patient who does not register data of manual dominance and a second case in which 2 patients do not register information about smoking. The median age of the participants was 42 years (interquartile range = 25), 60.4% of them were women (n = 110); no significant differences were found between the age and gender of the participants (p = 0.923). In total, 5460 joint recesses were evaluated. Table 1 shows the summary of the sociodemographic characteristics of the participating volunteers.
Distribution of the sociodemographic aspects of the participants (n = 182).
| Absolute frequency | Relative frequency | |
|---|---|---|
| [0,1–3]Gender | ||
| Man | 72 | 39.56% |
| Woman | 110 | 60.44% |
| [0,1–3] | ||
| [0,1–3]Age groups | ||
| 20 to 30 years | 50 | 27.47% |
| 31 to 40 years | 34 | 18.68% |
| 41 to 50 years | 38 | 20.88% |
| 51 to 60 years | 34 | 18.68% |
| 61 to 70 years | 16 | 8.79% |
| 71 to 80 years | 10 | 5.49% |
| [0,1–3] | ||
| [0,1–3]Ethnicity | ||
| Mestizo | 180 | 98.90% |
| Caucasian | 1 | 0.55% |
| Afro-Latin | 1 | 0.55% |
| [0,1–3] | ||
| [0,1–3]Occupation | ||
| Exclusively manual | 97 | 53.30% |
| Administrative | 27 | 14.84% |
| Intellectual | 43 | 23.63% |
| Combination | 15 | 8.24% |
| [0,1–3] | ||
| [0,1–3]Working time | ||
| < 5 years | 42 | 23.08% |
| 5 and 10 years | 38 | 20.88% |
| > 10 years | 102 | 56.04% |
| [0,1–3] | ||
| [0,1–3]Cigarette smoking | ||
| Yes | 20 | 11.11% |
| No | 160 | 88.89% |
| [0,1–3] | ||
| [0,1–3]High blood pressure | ||
| Yes | 24 | 13.19% |
| No | 158 | 86.81% |
| [0,1–3] | ||
| [0,1–3]Diabetes mellitus | ||
| Yes | 11 | 6.04% |
| No | 171 | 93.96 |
| [0,1–3] | ||
| [0,1–3]Hypothyroidism | ||
| Yes | 18 | 9.89% |
| No | 164 | 90.11% |
| [0,1–3] | ||
| [0,1–3]Lung disease | ||
| Yes | 2 | 1.10% |
| No | 180 | 98.90% |
| [0,1–3] | ||
| [0,1–3]None | ||
| Yes | 126 | 69.23% |
| No | 56 | 30.77% |
| [0,1–3] | ||
| [0,1–3]Other | ||
| Yes | 38 | 20.88% |
| No | 144 | 79.12% |
| [0,1–3] | ||
| [0,1–3]Physical activity | ||
| Sedentary lifestyle | 138 | 75.82% |
| Regular physical activity | 44 | 24.18% |
| [0,1–3] | ||
| [0,1–3]Hand dominance | ||
| Left | 8 | 4.42% |
| Right | 173 | 95.58% |
| Agea | [0,2–3]43 (25) | |
| Weighta | [0,2–3]69 (18) | |
| Heighta | [0,2–3]1.61 (0.13) | |
| BMIa | [0,2–3]26.3 (5.5) | |
Through dorsal scanning and semi-quantitative evaluation of the joints of hands and foot it was possible to identify 232 ultrasonographic findings in 87% of the participating volunteers. The percentage of these findings for joint effusion, synovial hypertrophy, erosions and power Doppler was 68.1%, 29.3%, 2.1% and 0.4%, respectively. The feet had greater alterations compared with the hands (70.7% vs. 29.3%), being the first MTP joint (52%), followed by the third MTP joint (15%) and the radiocarpal joint (9.5%) the joints in which the greatest number of abnormalities were identified in general. By laterality, the right side was more compromised (55.17%) compared with the left side (44.83%). There were no differences in the identification of the power Doppler signal of those volunteers with synovial hypertrophy and ultrasound scanning performed in water at room temperature and cold water alternately. The most frequently documented semi-quantitative score was the grade 1 in 65% of joint effusions, 82% of synovial hypertrophy, 60% of erosions and in one case of power Doppler (Table 2).
Distribution of the semi-quantitative ultrasonographic findings (n = 232).
| Absolute frequency | Relative frequency | |
| [0,1-3]Joint effusion | ||
| Yes | 158 | 68.10% |
| [0,1-3]Severity | ||
| Grade 1 | 102 | 64.56% |
| Grade 2 | 47 | 29.75 |
| Grade 3 | 9 | 5.70% |
| [0,1-3] | ||
| [0,1-3]Synovial hypertrophy | ||
| Yes | 68 | 29.31% |
| [0,1-3]Severity | ||
| Grade 1 | 56 | 82.35% |
| Grade 2 | 8 | 11.76% |
| Grade 3 | 4 | 5.88% |
| [0,1-3] | ||
| [0,1-3]Erosions | ||
| Yes | 5 | 2.16% |
| [0,1-3]Severity | ||
| Grade 1 | 3 | 60.00% |
| Grade 2 | 1 | 20.00% |
| Grade 3 | 1 | 20.00% |
| [0,1-3] | ||
| [0,1-3]Power Doppler | ||
| Yes | 1 | 0.43% |
| [0,1-3]Severity | ||
| Grade 1 | [0,2-3] Left MTP5 | |
In the feet, joint effusion was the most frequent abnormality in 71% of cases, being compromised in this order of frequency, the MTP1 (78.6%), MTP3 (18%) and MTP5 (3.4%) joints. Synovial hypertrophy is the second in frequency (26%), being located in 63% of cases in the MTP1 joint and in 32.56% in the MTP2 joint. Erosions were documented in 1.8% of cases (2.8% of the volunteers), 2 in the MTP1 joint (grade 2 and grade 3) and one in the MTP5 joint (grade 1). Only in one volunteer (0.9%), a grade 1 power Doppler signal was found in the fifth left metatarsal, associated with synovial hypertrophy and mild effusion (grade 1). Finally, 66% of the findings in the feet were mild, 24% moderate and 8.5% severe (Tables 3 and 4).
Distribution of the semi-quantitative ultrasonographic findings according to the type of joint.
| Joint | Total patients | Total of findings (cases) | Joint effusion | Synovial hypertrophy | Erosion | Power Doppler |
|---|---|---|---|---|---|---|
| Radiocarpal | 15 | 22 | 9 | 13 | 0 | 0 |
| Distal radioulnar | 2 | 2 | 0 | 2 | 0 | 0 |
| MCP1 | 2 | 2 | 2 | 0 | 0 | 0 |
| MCP2 | 6 | 8 | 6 | 1 | 1 | 0 |
| MCP3 | 5 | 6 | 6 | 0 | 0 | 0 |
| MCP4 | 9 | 9 | 7 | 2 | 0 | 0 |
| MCP5 | 2 | 2 | 1 | 1 | 0 | 0 |
| PIP1 | 2 | 3 | 2 | 1 | 0 | 0 |
| PIP2 | 1 | 4 | 2 | 2 | 0 | 0 |
| PIP3 | 3 | 5 | 3 | 2 | 0 | 0 |
| PIP4 | 1 | 3 | 2 | 1 | 0 | 0 |
| PIP5 | 2 | 2 | 1 | 0 | 1 | 0 |
| MTP1 | 77 | 121 | 92 | 27 | 2 | 0 |
| MTP3 | 25 | 35 | 21 | 14 | 0 | 0 |
| MTP5 | 7 | 8 | 4 | 2 | 1 | 1 |
| Total | 159 | 232 | 158 | 68 | 5 | 1 |
Distribution of the semi-quantitative ultrasonographic findings according to their severity.
| Joint | [0,2–4]Joint effusion | [0,5–7]Synovial hypertrophy | [0,8–10]Erosion | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Severity | G1 | G2 | G3 | G1 | G2 | G3 | G1 | G2 | G3 |
| Radiocarpal | 7 | 2 | --- | 12 | 1 | --- | --- | --- | --- |
| Distal radioulnar | --- | --- | --- | 2 | --- | --- | --- | --- | --- |
| MCP1 | 2 | --- | --- | --- | --- | --- | --- | --- | --- |
| MCP2 | 4 | 2 | --- | 1 | --- | --- | 1 | --- | --- |
| MCP3 | 6 | --- | --- | --- | --- | --- | --- | --- | --- |
| MCP4 | 6 | 1 | --- | 2 | --- | --- | --- | --- | --- |
| MCP5 | 1 | --- | --- | 1 | --- | --- | --- | --- | --- |
| PIP1 | 1 | 1 | --- | 1 | --- | --- | --- | --- | --- |
| PIP2 | --- | 2 | --- | 1 | 1 | --- | --- | --- | --- |
| PIP3 | 1 | 2 | --- | 1 | 1 | --- | --- | --- | --- |
| PIP4 | --- | 2 | --- | 1 | --- | --- | --- | --- | --- |
| PIP5 | --- | 1 | --- | --- | --- | --- | 1 | --- | --- |
| MTP1 | 59 | 27 | 6 | 24 | 3 | --- | --- | 1 | 1 |
| MTP3 | 11 | 7 | 3 | 8 | 2 | 4 | --- | --- | --- |
| MTP5 | 4 | --- | --- | 2 | --- | --- | 1 | --- | --- |
31% of volunteers showed abnormalities in their hands. Overall, the most constant ultrasonographic alteration was joint effusion in 60% of the findings (68% grade 1), and synovial hypertrophy in 37% of them (88% grade 1). Only one subject presented 2 erosions, one in the PIP5 joint and the other in the MCP 2 joint, both of grade 1. No power Doppler signal was found, nor was any joint effusion or severe synovial hypertrophy (grade 3). In this group of joints the major findings in order of frequency appeared in the MCP joints (40%), followed by the carpus (35%) and the PIP joints (25%). In the MCP joints the abnormalities were more frequent in the MCP4 (7 with joint effusion and 2 with synovial hypertrophy), and in the MCP2 (6 with joint effusion, one with synovial hypertrophy and one with erosion) joints. Abnormalities in the PIP joints were the less prevalent in general, they were only documented there in 5.6% of the participants (7.3% of the total of ultrasonographic findings), being effusion (59%) and synovial hypertrophy (35%) the most prevalent findings at this level (Tables 3 and 4).
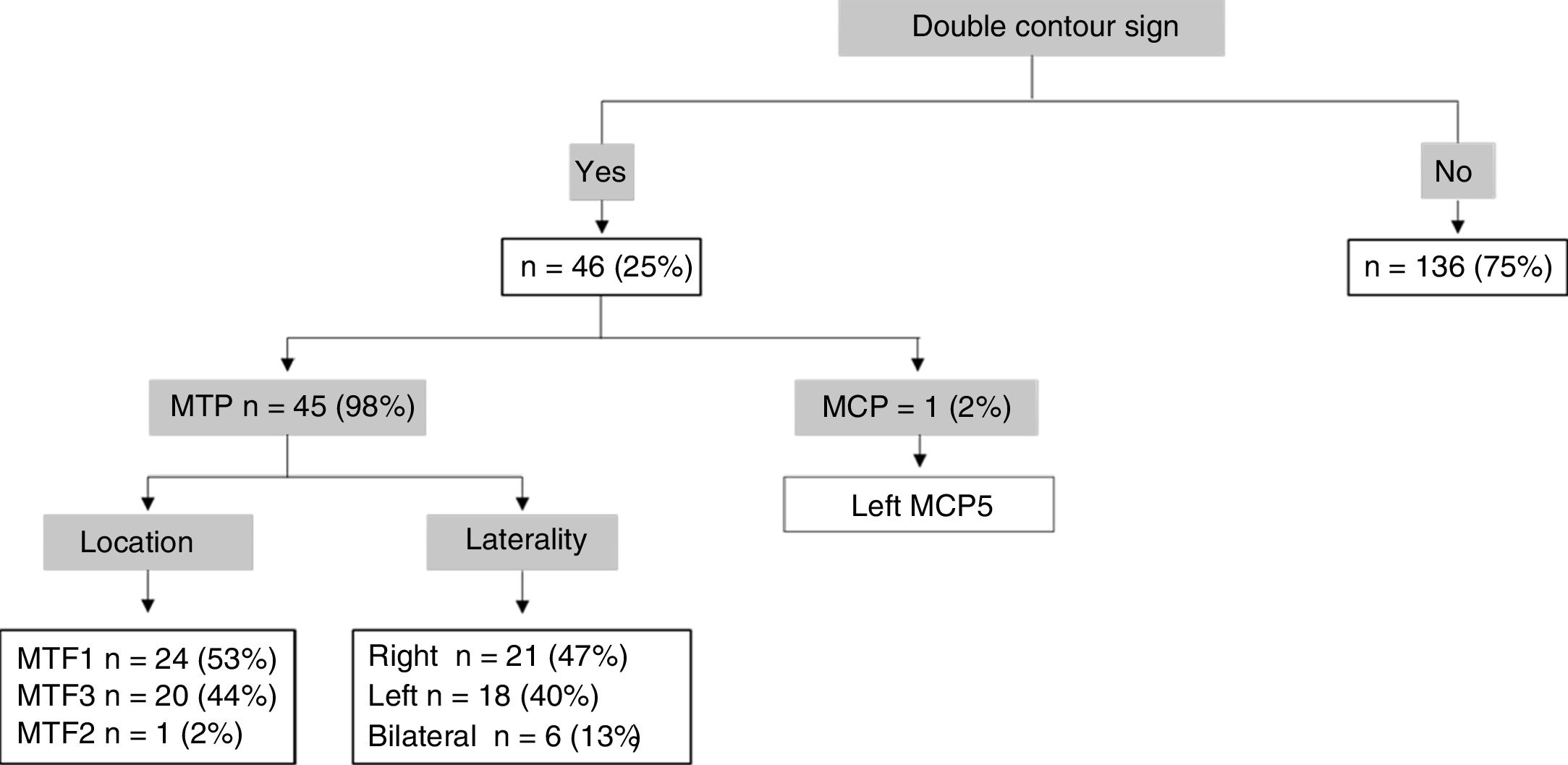
Regarding the ultrasonographic findings at the level of articular cartilage and periarticular soft tissues (not related to the semi-quantitative Szkudlarek system), the presence of hyperechogenic images floating in the synovial fluid type «snowstorm» was documented in 7% of the volunteers (80% located in the MTP1 joint) and synovial cysts (carpal dorsum) in 2.7% of them. Strikingly, 25.27% of the volunteers had the sign of the double contour, which in almost all cases was located at the level of the MTP joints with right predominance (Fig. 1).
Relationship between ultrasonographic findings and sociodemographic characteristics
Regarding the relationship of joint effusion and synovial hypertrophy with some sociodemographic aspects, it was found that the age group which presented more findings was the group of 51–60 years, with significant differences with the other age groups (p < 0.00001). The occupations of manual exclusivity were those that presented the highest percentage of joint effusion and synovial hypertrophy, with significant differences compared with the other occupations (p < 0.005). In relation to the working time, individuals with more than 10 years presented greater findings of joint effusion and synovial hypertrophy with significant differences. The patients with high blood pressure, diabetes mellitus and hypothyroidism had a higher frequency of joint effusion and synovial hypertrophy (Table 5).
Sociodemographic data according to findings of joint effusion and synovial hypertrophy.
| [0,2–3]Joint effusion n = 158 | [0,4–5]Synovial hypertrophy n = 68 | |||
|---|---|---|---|---|
| N (%) | p-Value | N (%) | p-Value | |
| [0,1–5]Gender | ||||
| Man | 71 (4.94) | 0.179 | 31 (45.59) | 0.325 |
| Woman | 87 (55.06) | 37 (54.41) | ||
| [0,1–5] | ||||
| [0,1–5]Age groups | ||||
| 20 to 30 years | 24 (15.19) | < 0.00001 | 11 (16.18) | < 0.00001 |
| 31 to 40 years | 22 (13.92) | 8 (11.76) | ||
| 41 to 50 years | 28 (17.72) | 6 (8.82) | ||
| 51 to 60 years | 61 (38.61) | 29 (42.65) | ||
| 61 to 70 years | 10 (6.33) | 6 (8.82) | ||
| 71 to 80 years | 13 (8.23) | 8 (11.76) | ||
| [0,1–5] | ||||
| [0,1–5]Occupation | ||||
| Exclusively manual | 109 (68.99) | < 0,00001 | 51 (75,0) | 0,003 |
| Administrative | 11 (6.96) | 3 (4.41) | ||
| Intellectual | 26 (16.46) | 10 (14.71) | ||
| Combination | 12 (7.59) | 4 (5.88) | ||
| [0,1–5] | ||||
| [0,1–5]Working time | ||||
| < 5 years | 26 (16.46) | 0.007 | 5 (7.35) | 0.001 |
| 5 y 10 years | 24 (15.19) | 10 (14.71) | ||
| > 10 years | 108 (68.35) | 53 (77.94) | ||
| [0,1–5] | ||||
| [0,1–5]Cigarette smoking | ||||
| Yes | 12 (7.64) | 0.161 | 6 (8.82) | 0.546 |
| No | 145 (92.36) | 62 (91.18) | ||
| [0,1–5] | ||||
| [0,1–5]Comorbidities | ||||
| High blood pressure | 30 (18.99) | 0.029 | 19 (27.94) | < 0.001 |
| Diabetes Mellitus | 17 (10.76) | 0.012 | 6 (8.82) | 0.333 |
| Hypothyroidism | 27 (17.09) | 0.002 | 12 (17.65) | 0.031 |
| [0,1–5] | ||||
| [0,1–5]Physical activity | ||||
| Sedentary lifestyle | 126 (79.75) | 0.243 | 58 (85.29) | 0.066 |
| Regular physical activity | 32 (20.25) | 10 (14.71) | ||
| [0,1–5] | ||||
| [0,1–5]Hand dominance | ||||
| Left | 4 (2.55) | 0.247 | 2 (2.94) | 0.550 |
| Right | 153 (97.45) | 66 (97.06) | ||
When assessing the joints with the highest number of abnormalities, no statistically significant differences were found between the age groups and the presence of ultrasonographic abnormalities at the level of the radiocarpal joints (p = 0.203), but there were differences with the MTP1 (p = 0.033) and MTP3 (p ≤ 0.001) joints. Regarding the compromised laterality, significant differences were found with the age groups both in the right MTP3 joint (p = 0.002) and the left MTP3 joint (p = 0.007). When assessing the occupation (manual vs. administrative) against the abnormalities in the radiocarpal joints, no significant differences in right (p = 0.204) or left (p = 0.950) laterality were found. No statistically significant difference was found between the gender and the cases of ultrasonographic findings by laterality (p = 0.688). Likewise, their association with the age group (p = 0.164), type of occupation (p = 0.166), working time (p = 0.930), cigarette smoking (p = 0.075), comorbidities (p > 0.5) and physical activity (p = 0.667) was not documented.
When evaluating the sum of scores of the Szkudlarek semi-quantitative scale by age ranges of the patients, significant differences were found (p = 0.0028). Similarly, there were statistically significant differences between the sum of the semi-quantitative Szkudlarek scale with some compromised joints, such as the PIP3 (p = 0.045), MTP1 (p = 0.033) and MTP3 (p < 0.0001). The other sociodemographic aspects did not show significant differences.
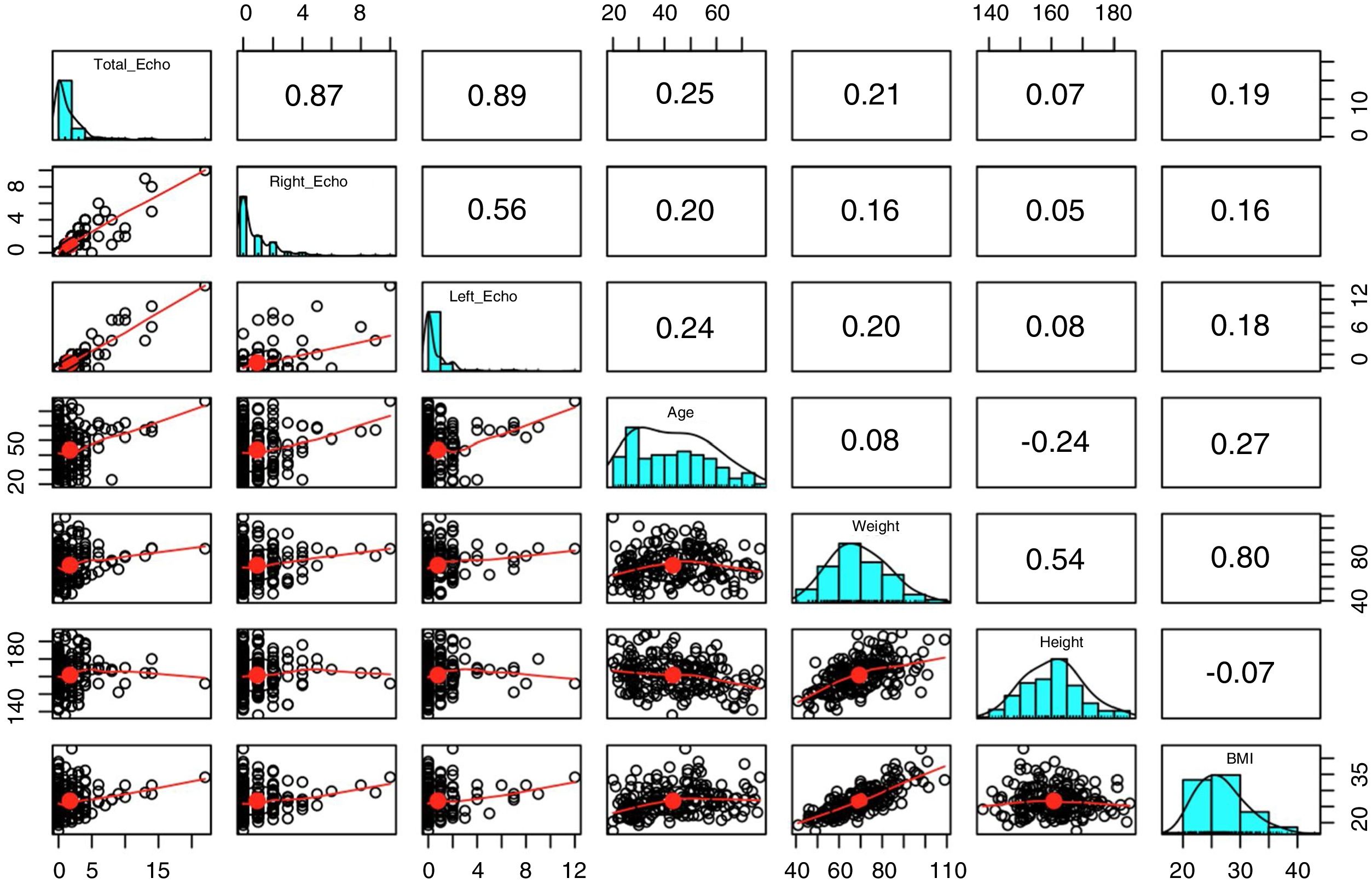
A weak linear correlation strength was identified between the scale scores and the age of the volunteers. The relationship between the scale scores and the anthropometric indicators showed a linear lack of correlation, where a degree of joint variation between these variables was not observed (r < 0.2) (Fig. 2).

When evaluating the double contour with respect to the sociodemographic aspects, no relationship was found with the age group (p = 0.200), nor with the occupation (p = 0.393), nor with the years of work (p = 0.435); this same fact occurred with the other sociodemographic aspects, except for the gender, where it was more frequent in men than in women (p = 0.043). Significant differences were found between the double contour and ultrasonographic findings of effusion and synovial hypertrophy (p < 0.0001).
Reproducibility of Szkudlarek semi-quantitative measurementsThe concordance for the semi-quantitative measurements was determined in 10% of the stored static images. 50 representative images of all the studied recesses (DICOM format) were selected and reassessed independently by the 2 experts in musculoskeletal ultrasound. The intraobserver concordance was moderate and significant (Kappa = 0.4591; 95% CI: 0.253 to 0.655; p < 0.0001) and the interobserver concordance was mild and lower than the intraobserver (Kappa = 0.2155; 95% CI: 0.066 to 0.402; p = 0.0017).
DiscussionIn recent years, musculoskeletal ultrasound has been becoming a very valuable tool in the daily practice of rheumatology, being considered by many as a complement to the physical examination. However, for its proper interpretation and adoption of specific behaviors it is essential to know the limit between normal and pathological in the different anatomical regions evaluated, information which is little available due to the lack of local studies carried out to date.
Our study demonstrates that 87% of the asymptomatic volunteers presented at least one abnormality at the level of the hands and feet, being the MTP (70%: 74% MTP1, 21% MTP3), MCP (11.6%) and radiocarpal (9.5%) joints the recesses most frequently involved. Regarding the totality of semi-quantitative ultrasonographic findings, the most common alterations were joint effusion (68%) and synovial hypertrophy or synovitis (29%), affecting in order of frequency at the level of the feet, the MFT1 (joint effusion 56.1%, synovitis 16.5%) and MTP3 (joint effusion 13%, synovitis 8.5%) joints. Works conducted in other latitudes reveal that in asymptomatic individuals is frequent to find these abnormalities.13–21,24–28 Padovano et al., in France, evaluated the peripheral joints of 207 healthy volunteers similarly demonstrating that 88% of them had at least one finding.16 In this group of participants the MTP1 (36.5%) and MTP2 (30.5%) joints were the most compromised. Kitchen and Kane also documented that 68.4% of the healthy subjects evaluated (n = 30) had some degree of synovitis at the level of the MTP1 joint (56.7% grade 1 and 26.7% grade 2).24 Other works coincide in the same way in highlighting the high involvement of MTP joints by joint effusion and synovitis, possibly in the context of biomechanical stress or asymptomatic incipient degenerative changes.13,17,18
In rheumatoid arthritis, disease that is most commonly associated with synovitis, foot involvement occurs in 90% of patients at some point of its evolution,29–31 and it is the second joint group most frequently affected following the hands (63.9% forefoot).30 In fact, 15% of patients can start with isolated commitment at this level and exhibit structural damage before in any other joint.32 The EULAR-OMERACT ultrasound working group recently released the definition and classification of synovitis in rheumatoid arthritis based on consensus, considering it as that synovial hypertrophy associated or not with power Doppler signal.11 If we take into account our findings and those previously related we can consider that synovitis of the MTP1 and MTP3 joints associated or not with joint effusion are common findings in asymptomatic subjects and, therefore, they lack sufficient specificity at the time of defining or categorizing an inflammatory disease (except for that of microcrystalline origin). In order to improve this specificity, some authors consider the fifth metatarsal joint as an area of “high performance” and a good starting point for the ultrasound evaluation of the patient with suspected inflammatory joint disease, as it is the anatomical region in which most frequently and early erosive changes appear.33–36 Millot et al., in their case-control study, compared patients with early arthritis (n = 127, French multicenter cohort ESPOIR) with a control group of healthy subjects of the same age and gender (n = 127). In 11% of the control group (n = 14) 14 joints with erosions were found, 8 in the MTP5 joint, 5 in the MCP2 joint, and one in the MCP5 joint. 78% of the total of erosions were scored as grade 1 or 2, and none was associated with a power Doppler signal.13 Contrary to this, Padovano et al., in 6621 recesses, did not report erosive commitment at the level of the MTP5 joints, which could be explained by the lower average age of their participants (35.5 years vs. 48.3 years) and the type of linear transducer used (18 MHz vs. 16 MHz).16 In our volunteers, only 1.3% of the total findings corresponded to erosions located in the feet (n = 3), 2 in the MTF1 joints and only one in the MTP5 joint, that in concordance with Millot was scored as grade 1 and was not associated with power Doppler signal. In the same sense, Machado et al. compared 78 healthy volunteers (average age of 44 years) with 60 patients with established rheumatoid arthritis, concluding that finding a bone erosion grade 2 in the lateral recess of the fifth MTP joint conditioned a 100-fold greater probability to belong to the group of arthritis compared with a score of 0 (p ≤ 0.001).20 One of the aspects highlighted in the work conducted by Millot was that in none of its participants were found an association between the erosion and the power Doppler signal, or between the erosion and synovial hypertrophy in the same recess,13 data that are in contrast with ours in which one volunteer presented a combination of erosion grade 3 and synovial hypertrophy grade 2 in the MTP1 joint. In addition to this, only in one of the total of our volunteers was observed a power Doppler signal grade 1 in the MTP5 joint (0.43%). The present study highlights the absence of power Doppler signal at the level of the first MTP joints, contrary to what was reported by Machado18 and Padovano,16 in which a high percentage is registered; however, the latter author agrees not to show signs of neovascularization in any of the MTP5 joints assessed. It could be said, then, that at the level of these joint groups the fifth metatarsal joint could offer greater specificity when discriminating between normality and abnormality (inflammation or lesion).
In about 30% of the volunteers, ultrasonographic findings on the hands were registered, involving in order of frequency the MCP, the radiocarpal and finally the distal interphalangeal joints. Padovano et al. recognized that in the upper extremities the most affected recesses were the radiocarpal and MCP3 in 6% and 2%, respectively,16 however, and according to Hau et al.,37, they did not find any ultrasonographic abnormality in the PIP joints, a result that is in contrast with ours, in which a non-negligible number of the total of findings (7.3%: 59% joint effusion, 35% synovitis and 5.6% erosion) were found at this level, which could be explained in large part by the higher average of age of our participants and the type of occupation predominantly manual during more than 10 years. In the MCP region, we documented that 15% of the total findings corresponded to synovitis (synovial hypertrophy grade 1 in its totality). Fodor et al.15 did not demonstrate synovitis in the MCP 2–5 joints of 50 healthy volunteers with an average age of 42 years and moderate physical activity, however, and contrary to what was published by Padovano, who did not registered erosions,16 these were identified in 7% of them, mainly in the MCP2 joint. In the present study it was possible to document only one erosion (grade 1) in the MCP2 articular recess, which was not associated with synovitis.
8% of the volunteers showed ultrasonographic alterations in radiocarpal recesses, and of the total of abnormalities documented there, 60% corresponded to synovitis (92% grade 1) and 40% to joint effusion (78% grade 1 and 22% grade 2). This commitment is also described by Machado et al.;18 however, a significant percentage of these recesses were found associated with erosions and power Doppler signal. In rheumatoid arthritis the joint most frequently involved at the level of the hand is the wrist, reaching 75% of them, and specifically its ulnar aspect is the one that almost always becomes the first site to be affected.38–41 Of the totality of ultrasound findings in our participants, only 0.8% of them were located in the distal radioulnar joint (2 cases of mild synovitis), which makes it the individual recess with fewer recorded findings.
With regard to neoangiogenesis, it represents the first step in the inflammatory cascade of synovitis that eventually leads to the development of erosions.36 Although in several studies the power Doppler signal has been registered in joints of healthy subjects,13–16,18,24,42 in the hands of the group of subjects evaluated it was not identified despite their predominant sociodemographic profile.
The present study was able to recognize in a significant number of articular recesses the double contour sign, classically considered in the literature as a product of the deposit of urates on the surface of the articular cartilage.43–45 Salazar and Calvo46 documented this sign in the first MTP joint in 24% of asymptomatic patients with hyperuricemia, which raises the possibility of metabolic syndrome or asymptomatic hyperuricemia as a potential etiology of these abnormalities in our participants.
Little information published in the literature is available in reference to the articular ultrasonographic findings of asymptomatic subjects and their relationship with sociodemographic aspects. Machado et al.18 demonstrated that the association of their semi-quantitative measurements with the sociodemographic characteristics was very sporadic and inconsistent in the 130 healthy volunteers evaluated. On the contrary, our work allowed us to demonstrate a positive relationship between joint effusion and synovial hypertrophy with variables such as age, exclusive manual occupation and working time longer than 10 years. In the volunteers aged between 51 and 60 years it was possible to identify the greatest number of findings, being synovial hypertrophy and joint effusion the predominant abnormalities in 43% and 39%, respectively. Compared with the synovial effusion, the association was stronger for synovitis in those volunteers with a working time longer than 10 years; and in those participants with exclusive manual occupation the association was greater for joint effusion. This gives us a glimpse that age and biomechanical factors are important variables when interpreting the joint ultrasonographic findings in hands and feet. For the remaining sociodemographic variables and other semi-quantitative measurements, such as erosion and power Doppler, it was not possible to determine associations due to the smaller sample size that was grouped in these results. Further studies with a larger sample size will provide a complement for such information.
One of the characteristics of musculoskeletal ultrasound that puts it at a disadvantage compared to other imaging modalities is its operator-dependent nature.8,47 Several studies have related that in the scenario of inflammatory joint disease, intra- and interobserver concordance is good in general; however, the works that evaluate concordance in healthy and asymptomatic individuals are scarce, and are conducted in a low number of participants and with variable results.48–52 Fodor et al.,15 using a linear transducer of 18 MHz, reported that the interobserver concordance for the semi-quantitative evaluation of erosions in MCP joints was excellent (Kappa = 0.83). The study conducted by Machado, on the other hand, reports relatively wide ranges of concordance.18 There the Kappa value for the semi-quantitative evaluations ranged between 0.341 and 0.71. Our work shows that the interobserver concordance was slight (Kappa = 0.2155) and lower than the intraobserver (Kappa = 0.4591), which suggests that the standardization of study protocols in musculoskeletal ultrasound in our environment It is an urgent and unavoidable task.
The limitations of this study include the operator-dependent nature of ultrasonography and its aspects related to the configuration of the equipment, the lack of confirmation of our findings with other imaging modalities, the use of static images instead of dynamic images in the evaluation of the interobserver concordance and the relatively asymmetric distribution of the participants regarding some of their sociodemographic variables.
ConclusionOur work represents the first study conducted in Colombia in which the semi-quantitative ultrasonographic findings in the joints most frequently compromised by inflammatory diseases in an important number of asymptomatic volunteers with diverse sociodemographic characteristics are described in detail. We were able to document that the absence of significant inflammatory changes at the level of the fifth metatarsal joint and, in the case of the hands, the absence of power Doppler signal, the lack of distal radioulnar involvement, the absence of synovitis accompanied by erosion and a greater predominance of mild alterations (joint effusion and synovitis grade 1), constitute potentially specific findings in asymptomatic subjects that deserve to be confirmed as such in future studies.
FundingThe present work was funded by the Colombian Association of Rheumatology by public call of the year 2017.
Conflict of interestThe authors declare that they have no financial or personal relationship with individuals or organizations that could give rise to a conflict of interest in relation to the present study.
We extend our sincere gratitude to the volunteers who supported the development of this work: workers of the sections of transport, gardening, maintenance, plumbing and general services of the National University of Colombia. To the professors, students, administrative body, healthcare staff, and to the patients and their accompanying relatives of the National University Hospital of Colombia.
Please cite this article as: Calderón-Cordero C et al. Hallazgos ultrasonográficos a nivel de articulaciones de manos y pies en sujetos voluntarios asintomáticos. Rev Colomb Reumatol. 2019;26:165–176.
