



Scapular spine stress fractures have been scarcely reported in the literature. Their pathomechanics, clinical course and treatment are not well established. We review 3 cases in 2 patients that were associated with cuff dysfunction. On follow-up, none of these fractures progressed to healing. Two of them needed osteosynthesis and bone grafting, and the third one became a painless non-union.
The authors propose the combination of 3 factors as a reason for this lesion: a functionally impaired cuff, a greater activation of the muscles with origin and insertion in the spine-acromion and a fragile bone. As we believe that these fractures are unstable, and non-union would be expected, their surgical management is recommended.
Las fracturas de estrés de la escápula son extremadamente raras, más aún aquellas que afectan a la espina. Su patogénesis, biomecánica, evolución clínica y tratamiento no están bien establecidos. En este artículo se describen 3 casos en 2 pacientes con lesión asociada del manguito rotador. Durante el seguimiento ninguna de las fracturas consolidó, 2 de ellas precisaron intervención quirúrgica mediante osteosíntesis y aporte de injerto, y la tercera permaneció como seudoartrosis indolora.
Los autores proponemos como patogénesis de este tipo particular de fracturas la combinación de 3 factores: un manguito alterado funcionalmente, un incremento en la acción de los músculos con origen e inserción en la espina de la escápula o base del acromion, y cierta fragilidad ósea concomitante. Pensamos que este tipo de fractura es inestable, acompañándose de una ausencia de consolidación, motivo por el que recomendamos su tratamiento quirúrgico.
Stress fractures of the scapular spine or the base of the acromion are unusual.1–3 In most cases they are described in young patients, associated to a violent muscular contraction in isolation or to repetitive load on the shoulder. This mechanism is also found in other stress fractures.4,5 Their presence in patients of advanced-medium ages in association with a concomitant rotator cuff lesion is even rarer. After reviewing the existing literature we only found 5 cases reporting this combination.6–8 This unusual location lies in the lateral edge of the spine of the scapula, where it thickens and rounds to join the glenoid cavity and give rise to the base of the acromion. Therefore, it is an area where powerful muscles intersect (insertion of the trapezius, origin of the deltoid), and these muscles require an adequate support for a correct movement of the shoulder girdle. The purpose of describing the present case reports is to provide a deeper insight into the etiology, pathomechanics, diagnosis and treatment of this particular type of fracture.
Case reportsCase 1The patient was a 56-year-old, right handed female without any prior history of trauma and with a history of systemic lupus erythematosus with 23 years evolution, who was following treatment with corticosteroids. She had suffered pain in the right shoulder for 3 years, and recent inability to elevate the arm above the head. The pain occurred mainly due to movement, but occasionally also at rest and at night. Examination revealed diffuse pain in the posterior aspect of the shoulder and the spine of the scapula. Active joint balance was 120° anteversion and 90° abduction, passively reaching 150 and 110°, respectively.
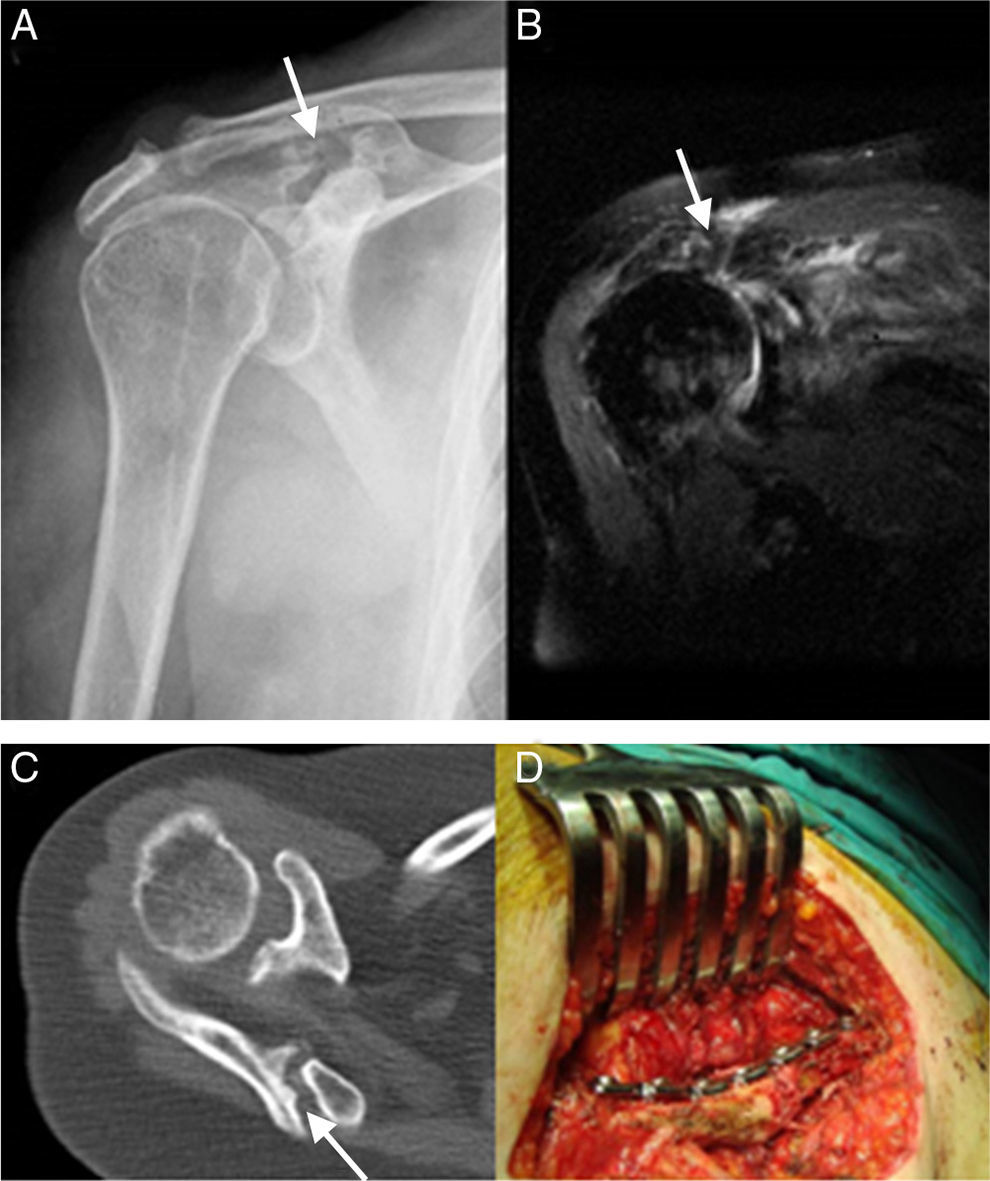
The simple radiographic study (including 3 anteroposterior, lateral and axillary projections) revealed the presence of a displaced fracture of the spine with cranial migration associated to the humeral head, indicative of rotator cuff arthropathy. This was confirmed by magnetic resonance imaging (MRI) (Fig. 1). The patient was initially treated conservatively.
 Simple radiograph in anteroposterior projection: fracture of the base of the acromion (arrow) and elevation of the humeral head. (B) Magnetic resonance imaging (MRI): massive rotator cuff tear (arrow). (C) Computed tomography (CT) scan showing a displaced fracture of the spine of the scapula, with no evidence of consolidation (arrow). (D) Internal fixation with a reconstruction plate.")
(A) Simple radiograph in anteroposterior projection: fracture of the base of the acromion (arrow) and elevation of the humeral head. (B) Magnetic resonance imaging (MRI): massive rotator cuff tear (arrow). (C) Computed tomography (CT) scan showing a displaced fracture of the spine of the scapula, with no evidence of consolidation (arrow). (D) Internal fixation with a reconstruction plate.
At 6 months follow-up, the simple radiographic study showed a lack of consolidation, which was confirmed by a computed tomography (CT) scan (Fig. 1). Due to persistent pain, the patient was intervened through a direct approach to the spine of the scapula, where an open fracture reduction and osteosynthesis were performed, with contribution of an autogenous graft and a reconstruction plate with 7 perforations (Fig. 1). The concomitant massive rotator cuff tear was not repaired. After surgery, the pain decreased considerably, not requiring analgesic treatment, but both active and passive joint balance remained unchanged. At present, the patient is awaiting an intervention to implant a reverse prosthesis in order to treat the rotator cuff arthropathy.
Case 2The patient was a 77-year-old female without a previous history of trauma, who was referred to our Shoulder and Elbow Surgery Unit by the Rheumatology Department due to bilateral shoulder pain with 2 years duration, which had worsened considerably in the previous 6 months. Upon physical examination, the patient presented moderate pain along the spine of the scapula in both shoulders. Active joint balance was 140° flexion and 125° abduction in the left shoulder, and 110° flexion and 90° abduction in the right shoulder. Passive joint balance was complete in both shoulders.
Follow-up at the Rheumatology consultation was due to thoracolumbar pain, leading to a diagnosis of osteoporotic crushing of 3 thoracic vertebrae. The patient also underwent a bone densitometry study which revealed severe osteoporosis.
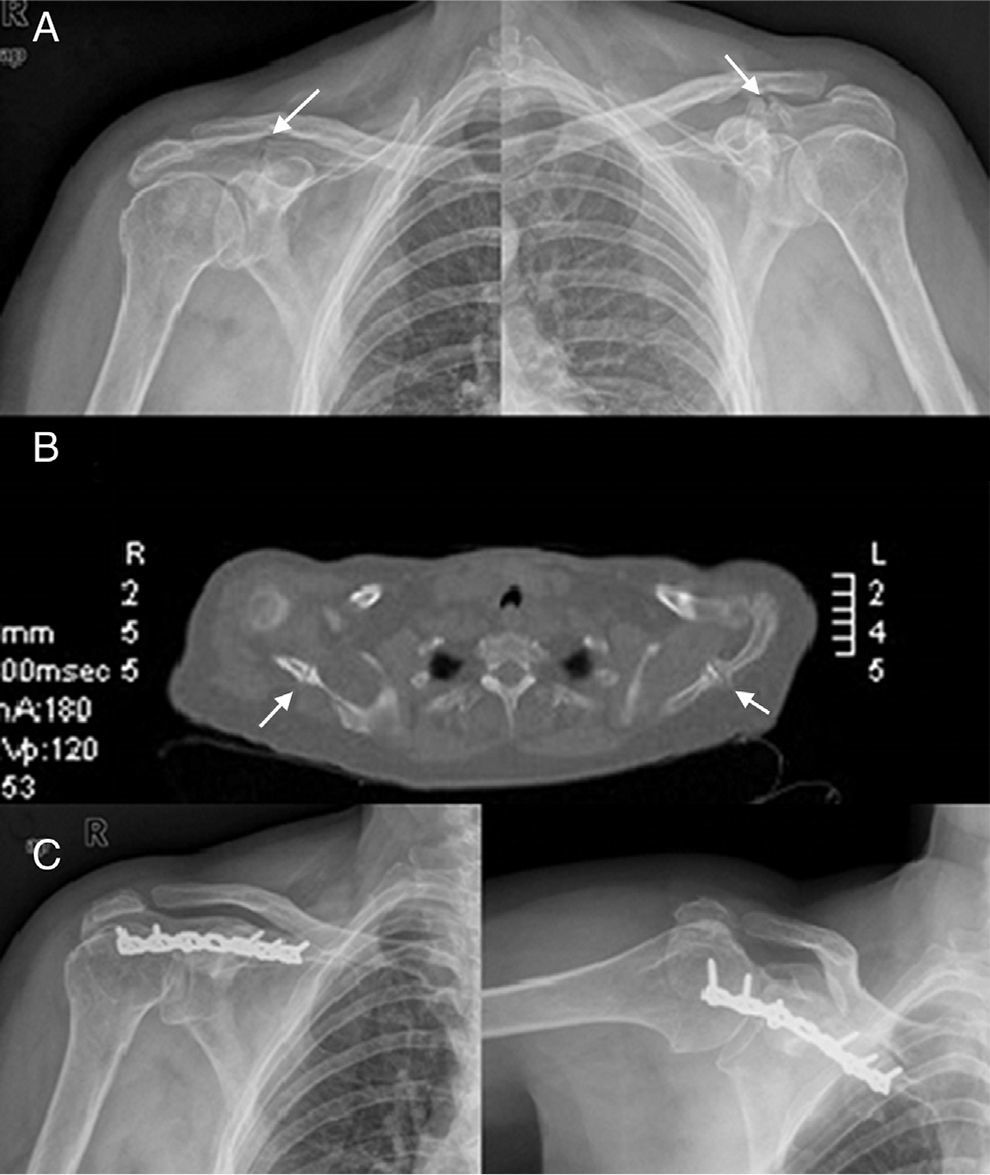
Simple radiographic study (anteroposterior, lateral and axillary) of both shoulders found a bilateral fracture of the spine of the scapula (Fig. 2). We requested an MRI study, which identified rotator cuff arthropathy in the right shoulder and massive tear with involvement of the supraspinatus and infraspinatus muscles on the left shoulder.
 Anteroposterior projection showing a bilateral fracture of the scapular spine (arrows). (B) Computed tomography (CT) scan: bilateral fracture with no evidence of consolidation (arrows). (C) Anteroposterior and axillary projections showing internal fixation with a reconstruction plate.")
(A) Anteroposterior projection showing a bilateral fracture of the scapular spine (arrows). (B) Computed tomography (CT) scan: bilateral fracture with no evidence of consolidation (arrows). (C) Anteroposterior and axillary projections showing internal fixation with a reconstruction plate.
Initially, the patient was treated conservatively, with progressive mobilization as the pain improved. She regained a virtually full range of motion in her left shoulder, with no residual pain. However, moderate-severe pain persisted in the right shoulder, with the same functional limitations suffered previously. After 1 year of follow-up, the simple radiographic study of both shoulders showed no signs of any consolidation whatsoever. This was confirmed by a computed tomography scan (Fig. 2). Painless pseudoarthrosis remained in the left shoulder and the patient was able to resume her previous activity with that shoulder. However, in the right side, the accompanying symptoms eventually led to an open reduction and internal fixation through a reconstruction plate and autogenous graft, performed by a direct approach to the scapular spine. The patient reported improvement of pain and, after a period of 6 months, postoperative radiographs showed consolidation of the fracture (Fig. 2).
DiscussionScapular fractures are rare, accounting for less than 1% of all fractures and usually being associated with high-energy trauma (traffic accidents). Stress fractures of the scapula are even rarer and the few cases reported have occurred among athletes in relation to repeated microtrauma or violent muscle contraction.1–3 There are very few studies indicating its association with alterations in the function of the rotator cuff and particularly in the context of cuff arthropathy.9 Lastly, only in 5 cases, belonging to 3 different works, has the fracture been located at the lateral end of the spine, passing in front of the spinoglenoid cavity, where the base of the acromion begins.6–8 This was the location of the fracture in the cases reported in this work, and the fact that these fractures were located precisely in the portion of the spine which presents greater thickness and resistance in order to fulfill its role as the source of the base of the acromion is worthy of investigation, even beyond the few references found in the current literature.
Dennis et al.9 published 3 cases of stress fractures of the anterior portion of the acromion (not of the base) among patients with established rotator cuff arthropathy, 2 of whom were being treated with corticosteroids due to rheumatoid arthritis. A dual etiology could be clearly established in these cases, involving bone fragility and the purely mechanical injury. The etiology would be simple to establish, with a humeral head impacting on a weakened bone. Anatomically, our causes were more related to those reported by Roy et al.6 and Shindle et al.7 The former reported 1 case of atraumatic stress fracture with an osteoporotic origin in the base of the acromion associated with rotator cuff arthropathy, whilst the second work described 2 cases of fractures of the scapular spine which were unrelated to any previous trauma, among patients with a previous rotator cuff arthropathy, 1 of them also associated with prior bone radiotherapy. In these 2 works we would have to exclude the direct action of the humeral head pressing on a weakened bone, but we would find a traction mechanism on pathological bones.
The primary function of the muscles making up the rotator cuff is to stabilize the glenohumeral joint exerting a compressive force on the humeral head on the concave surface of the glenoid and labrum, so that the main movement muscles of the shoulder (deltoid, latissimus dorsi) may carry out their function without significant superior displacement of the head on the glenoid. Alterations of the compressive force exerted by the rotator cuff on the humeral head end up causing glenohumeral instability by superior translation of the humeral head.9
The spine and acromion are the origin of the deltoid muscle (consisting of 3 parts: anterior, middle and posterior) and insertion of the trapezius muscle. Differences in the activity of each of the bellies of the deltoid muscle have been observed. When the arm is in abduction, the posterior portion of the deltoid acts as an external rotator. This is an important fact in patients with massive rotator cuff tear affecting the infraspinatus and teres minor muscles. Moreover, differences in the action of the uppermost fibers of the trapezius have also been observed in patients with symptomatic and asymptomatic rotator cuff tears. When the patient is symptomatic it is possible to observe an increase in the activation of the upper trapezius due to compensation of the elevation deficit by an increase in shoulder rotation.
Moreover, small differences in scapular kinematics have been observed among patients with and without subacromial impingement. Patients suffering impingement presented a slight increase in upward rotation of the tip of the scapula, along with elevation of the clavicle during flexion movements and a slight increase in posterior translation and inclination of the clavicle during elevation in the plane of the scapula. These differences have relative clinical importance, but represent compensatory movements which, in a certain way, can contribute to an overload of the scapular spine and the acromial process.
Fragility fractures are one of the main types of stress fracture and usually occur when a normal load is applied to a bone whose mechanical characteristics are weakened due to a deficiency of elasticity. They can occur virtually anywhere in the skeleton and are associated with multiple conditions, such as rheumatoid arthritis, osteoporosis, Paget's disease, osteomalacia and rickets, renal osteodystrophy and bone irradiation. The loss of the mechanical properties of a bone due to a decrease in bone mineral density in a long bone can be partially compensated by changes in the diameter of its diaphysis. However, this compensatory mechanism does not take place in cancellous bone, thus increasing the risk of fractures due to mechanical overloads. Out of the 5 cases similar to ours described previously,6–8 1 had undergone prior radiotherapy on the area due to breast cancer, another case, an 82-year-old female, had been diagnosed with osteoporosis, and the last case, a 78-year-old female, had not been diagnosed with any disease, but her age and gender allowed us to assume the presence of associated osteoporosis. The history of our 2 patients included diminished biomechanical properties of their bones. One had a long history of corticosteroid therapy, whilst the other had been diagnosed with severe osteoporosis through bone densitometry.
Therefore, the authors suggest that this type of fracture, very rare in this location, requires the combination of 3 factors. Firstly, the presence of a rotator cuff injury, which, as observed in the cases presented, can range from a massive tear thereof to a smaller lesion which alters its functionality. Secondly, an increase in activity (due to the previous injury) of the muscles with origin and insertion in the spine of the scapula or base of the acromion, during arm lifting movements. Lastly, the presence of decreased bone mineral density and changes in the microarchitecture (as is the case in osteoporosis) which make the bone biomechanically inferior to normal bone. These 3 etiological factors would cause a disruption in the kinematics of the scapula to compensate the glenohumeral dysfunction, which would eventually lead to a fracture in this location.
Aside from the etiopathogenesis of the fracture, and offering a more clinical view, we could add that in all 3 cases it was possible to establish the diagnosis through physical examination and simple radiography. The presence of pain over the spine and base of the acromion in patients with the aforementioned predisposing factors (rotator cuff dysfunction and bone fragility) should immediately make us think of this type of fracture, which may be easily confirmed by a complete radiographic study in 3 planes. It is not necessary to perform bone scintigraphy scans, and magnetic resonance imaging has only been used to assess the condition of the rotator cuff, reserving CT scans for the follow-up of fractures (displacement and consolidation process). Regarding treatment, common fractures of the spine of the scapula and base of the acromion normally associated with high-energy trauma are generally non-displaced fractures and their treatment is often conservative.10 Shindle et al.7 described 2 cases and both required surgical treatment. One of them was due to an absence of progression in the consolidation process, and the other due to persistence of pain. Roy et al.6 described another case which ended in a painless pseudoarthrosis and which did not require surgical intervention. Two of the 3 cases reported in this article eventually required open reduction and osteosynthesis with a plate. The presence of persistent pain and absence of consolidation were the 2 criteria followed to indicate an intervention. Conservative treatment was only applied in 1 case, in a patient suffering a bilateral fracture. Although consolidation was not achieved, pain and function improved with rehabilitation, and the demands of the shoulder decreased as the operated contralateral shoulder improved and assumed tasks which it could not perform previously. We agree with Roy et al. that these fractures are unstable due to increased mobility in the focus, causing altered scapular kinematics, which in turn increases the risk of pseudoarthrosis in this particular type of fractures. For these reasons, the authors propose surgical treatment thereof. A parallel issue would be that related to rotator cuff injury, whose treatment must be individualized according to the degree of injury (rehabilitation treatment, rotator cuff repair or inverted arthroplasty, depending on each case, in order to achieve a normalization of shoulder kinematics).
Level of evidenceLevel of evidence iv.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Please cite this article as: García-Coiradas J, Lópiz Y, Marco F. Fracturas de estrés de la espina de la escápula asociadas a lesión del manguito rotador: a propósito de 3 casos y revisión de la literatura. Rev Esp Cir Ortop Traumatol. 2014;58:314–318.
