



Traumatology and Orthopedic Surgery is one of the specialities with most complaints due to its scope and complexity. The aim of this study is to determine the characteristics of the complaints made against medical specialists in Traumatology, taking into account those variables that might have an influence both on the presenting of the complaint as well as on the resolving of the process.
Material and methodsAn analysis was performed on 303 legal judgments (1995–2011) collected in the health legal judgements archive of the Madrid School of Medicine, which is linked to the Westlaw Aranzadi data base.
ResultsCivil jurisdiction was the most used. The specific processes with most complaints were bone-joint disorders followed by vascular-nerve problems and infections. The injury claimed against most was in the lower limb, particularly the knee. The most frequent general cause of complaint was surgical treatment error, followed by diagnostic error. There was lack of information in 14.9%. There was sentencing in 49.8% of the cases, with compensation mainly being less than 50,000 euros.
ConclusionsTraumatology and Orthopedic Surgery is a speciality prone to complaints due to malpractice. The number of sentences against traumatologists is high, but compensations are usually less than 50,000 euros. The main reason for sentencing is surgical treatment error; thus being the basic surgical procedure and where precautions should be maximized. The judgements due to lack of information are high, with adequate doctor–patient communication being essential as well as the correct completion of the informed consent.
La Traumatología y Cirugía Ortopédica es una de las especialidades más reclamadas por su amplitud y complejidad. Nuestro objetivo es determinar las características de las reclamaciones presentadas contra médicos especialistas en Traumatología, considerando todas aquellas variables que puedan tener influencia tanto en el planteamiento de la demanda como en la resolución del proceso.
Material y métodosSe ha realizado un análisis de 303 sentencias judiciales (1995-2011) recogidas en el archivo de sentencias judiciales sanitarias de la Escuela de Medicina Legal de Madrid que se nutre de la base de datos de Westlaw Aranzazi.
ResultadosLa jurisdicción civil fue la más empleada. El proceso específico más reclamado fueron los trastornos osteoarticulares seguidos de las alteraciones vasculonerviosas y de las infecciones. La lesión reclamada ocurrió con más frecuencia en miembros inferiores sobre todo rodilla. La causa general de reclamación más frecuente fue el error terapéutico quirúrgico seguido del error diagnóstico. En el 14,9% fue el defecto de información. Existió condena en el 49,8% de los casos siendo la indemnización mayoritariamente menor de 50.000 euros.
ConclusionesConcluimos que la Traumatología y Cirugía Ortopédica es una especialidad proclive a las reclamaciones por mala praxis. El número de condenas a traumatólogos es elevado pero las indemnizaciones suelen ser menores de 50.000 euros. El motivo fundamental de las reclamaciones es el error terapéutico quirúrgico siendo pues el acto quirúrgico fundamental y donde se deben extremar las precauciones. Las condenas por deficiente información son elevadas siendo fundamental una adecuada comunicación médico-paciente y rellenar correctamente el consentimiento informado.
As Traumatology and Orthopedic Surgery is one of the specialities giving rise to the most litigation due to its amplitude and complexity, this article is intended to set out the characteristics of the lawsuits brought against specialists in Traumatology and Orthopedic Surgery, considering all those variables with a possible impact on both the lodging of the complaint and the resolution of the process.
The increase in the recourse to the courts in connection with health-care matters in Spain affects all specialities,1 whether these are surgical or medical, hospital-based or elsewhere. During the period between 1995 and 1998, a total of 932 complaints (both judicial and extra-judicial) were lodged against the national health system.
Medical errors cost the now-defunct INSALUD the equivalent of 4.33 million euros for compensation to 95 patients (an average of €46.8 thousand per patient).2
By specialities, Emergency Medicine represented 23.8% of all complaints, Gynecology and Obstetrics 18.2%, Traumatology and Orthopedic Surgery 11.2% and Neurosurgery 4.6%.2 These data are in line with those shown in the study undertaken by Torre from the Willis insurance company using re-insurance data from the public health services in Spain during the period from 2005 to 2007.3 A study conducted by Britain's National Health Service reported that 3254 complaints were dealt with during the years 1999–2000, with a cost of £386 million.4
One immediate consequence of this situation may be the systematic practice of defensive medicine,5,6 which moves away from the fluid relationship between doctors and their patients based on mutual trust and with a bioethical focus that boosts the patient's autonomy.
Nonetheless, an analysis of the factors giving rise to a complaint and the constraints influencing judicial decisions may be helpful for specialists in traumatology and orthopedic surgery to evaluate certain clinical practices, especially maximizing the precautions taken in view of signs that may lead to a judicial complaint.
In the practice of traumatology and orthopedic surgery, there are certain peculiarities7 that should be pointed out as they make this speciality particularly liable for litigation in connection with professional liability:8–10
- -
Patients with special characteristics such as polytraumatized individuals with whom proper communication between the patient and the physician is non-existent and the attention they require is multi-disciplinary with the participation of varied medical and surgical specialities, thus increasing the risk of litigation.
- -
Fractures treated as emergency cases where the treatment is conducted in difficult and adverse conditions.
- -
Treatment of young adults with greater expectations regarding the outcome following treatment.
- -
Use of implants (prostheses and osteosynthesis material).11
- -
The necessary active collaboration by patients in their treatment (rehabilitation, …)
- -
Existence of numerous sub-specialities in Traumatology and Orthopedic Surgery with a large number of specific procedures in each one (hand, spine, foot, …).
At the present moment, most of the medical literature published on medical negligence relate to the United States, but the analysis of the scenario in this country is different from what we might find in our setting as there are notable differences between the Spanish health and legal systems and those in the United States.
Arymani-Manso et al.12 provide us with an approach that is much closer to our context by reflecting data from insurers in Catalonia where 1.33% of physicians insured faced some sort of complaint, although only 0.26% had to pay any compensation to the party bringing the complaint.
At national level, we also have studies providing fundamental data such as the risk factors involved in surgery on mistaken locations, including, in particular, emergency operations, multiple simultaneous operations on the same patient, obesity or deformities in the patients, lack of familiarity with the instruments to be used, etc.13
AimsThe aim of the present paper is to analyze the court judgments handed down on appeal against specialists in traumatology and orthopedic surgery by establishing a classification of the medical surgical procedure referred to in the complaint and analysing the resolution of the judgments, i.e. considering whether the court finds against the physician and the amount of any penalty.
In this way, the results will be able to facilitate safer practice of the speciality, both for the patient and for the doctor.
There is no similar study in the literature of recent years referring specifically to the speciality of Traumatology and Orthopedic Surgery in Spain.
Material and methodsThe present study has been conducted on the “archive of court judgments on health-related cases at the School of Legal Medicine in Madrid”, part of the Complutense University in Madrid. This archive contains 2817 court judgments referring to health-related lawsuits from first instance and appeal courts in the civil, penal and administrative-dispute jurisdictions during the period between 1995 and January 2011.
This archive receives the judgments published by the CENDOJ and Westlaw Aranzadi database which collated all court judgments published by appeal and higher courts during the period under study.
The judgments of first instance courts are not uniformly published in any database.
We should clarify that the Spanish jurisdictional hierarchy is established on the basis of their trial function, i.e. we can distinguish, on the one hand, the courts of first instance or sole instance, which resolve on the matters for the first time, and, in certain cases (when there is disagreement on the judgment handed down), a second instance is possible, where the matter is tried again by a higher court (the regional High Courts of Justice, the Supreme Court and the National Court of Appeal).
In order to carry out the present study, 303 judgments have been selected out of the total of 2817 judgments relating to medical malpractice included on the archive in accordance with the following inclusion criteria:
- 1.
Judgments referring to a specialist in traumatology and orthopedic surgery in connection with the exercise of the speciality, as per the definition and maneuvers contemplated in ORDER SCO/226/2007 dated January 24th, 2007, which approved and published the training program for the speciality of Orthopedic Surgery and Traumatology in Spain.
- 2.
Judgments were expressly excluded where, even though the surgical act or the treatment performed formed part of the speciality of Traumatology and Orthopedic Surgery, it was carried out in that specific case by a professional other than a traumatologist (podologist, physiotherapist, etc.).
- 3.
The text of the judgment set out the reasons for the complaint, the circumstances and the place in which these occurred, their consequences and the court's resolution.
A data collection form was designed to record the details relating to each court judgment and this has implemented a series of variables that will be detailed in the results section below.
After producing a descriptive study of the variables, these were then contrasted using contingency tables with the χ2 test in the SPSS 15 statistical software, with the level of statistical significance set at 95% (P<0.05).
For a better interpretation of the tables containing the results, we should indicate that there are two categories analyzed in the present paper and these are intimately related and may even be confused with each other, namely the specific and general causes giving rise to the complaint, and so the following indications are given:
- -
The specific causes indicate in detail the lesion directly giving rise to the complaint:
- -
Infection: in the course of an orthopedic or surgical treatment, an infection occurred and was the reason for lodging the complaint.
- -
Vascular or nerve lesion.
- -
The patient developed a compartmental syndrome in the course of treatment.
- -
During evolution, the patient presented some kind of additional complication (bleeding, thromboembolism, vein thrombosis, cardiac pathology, pulmonary pathology, …) that we have decided to name as a group “systemic complications”.
- -
In the category of osteoarticular alterations, we have included residual joint pain, loss of joint mobility, joint deformities, …
- -
In the category of general causes, albeit intimately related with the specific causes, we have wished to design a more extensive category of grounds for complaint:
- -
Defective information: this includes both the lack of informed consent and defects in how it was obtained.
- -
Error in diagnosis: the patient alleges in the complaint that there was an error in the diagnosis; this category includes fractures that went unnoticed in an initial evaluation.
- -
Error in orthopedic therapy: patients indicate a non-surgical error in their treatment as the grounds for their complaint (poor application of casts, etc.).
- -
Error in surgical therapy: patients indicate an error in the course of their operation as the grounds for their complaint.
- -
Wrong side: the party bringing the complaint was operated on the contralateral limb.
- -
The category of poor medical follow-up includes grounds for complaint in the course of surgical or orthopedic treatment, such as delay in the diagnosis of infections, errors in the pharmacological prescription, non-prescription of anti-thrombotic drugs, etc.).
After studying the 303 judgments handed down in the second instance regarding negligence in traumatology, we have obtained the following results: (Tables 1–3)
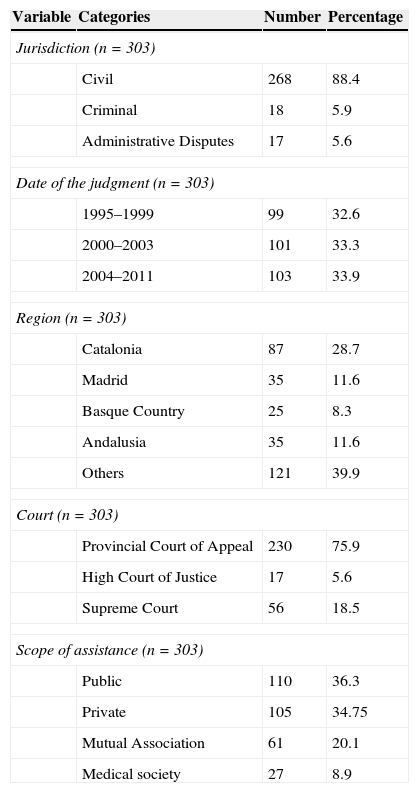
Administrative variables.
| Variable | Categories | Number | Percentage |
|---|---|---|---|
| Jurisdiction (n=303) | |||
| Civil | 268 | 88.4 | |
| Criminal | 18 | 5.9 | |
| Administrative Disputes | 17 | 5.6 | |
| Date of the judgment (n=303) | |||
| 1995–1999 | 99 | 32.6 | |
| 2000–2003 | 101 | 33.3 | |
| 2004–2011 | 103 | 33.9 | |
| Region (n=303) | |||
| Catalonia | 87 | 28.7 | |
| Madrid | 35 | 11.6 | |
| Basque Country | 25 | 8.3 | |
| Andalusia | 35 | 11.6 | |
| Others | 121 | 39.9 | |
| Court (n=303) | |||
| Provincial Court of Appeal | 230 | 75.9 | |
| High Court of Justice | 17 | 5.6 | |
| Supreme Court | 56 | 18.5 | |
| Scope of assistance (n=303) | |||
| Public | 110 | 36.3 | |
| Private | 105 | 34.75 | |
| Mutual Association | 61 | 20.1 | |
| Medical society | 27 | 8.9 | |
Clinical variables.
| Variable | Categories | Number | Percentage |
|---|---|---|---|
| Patient gender (n=303) | |||
| Men | 142 | 46.9 | |
| Women | 161 | 53.1 | |
| Specific causes triggering the complaint (n=303) | |||
| Infection | 36 | 11.9 | |
| Vascular or nerve lesion | 103 | 34 | |
| Compartmental syndrome | 7 | 2.3 | |
| Systemic complications | 25 | 8.3 | |
| Bone or joint alteration | 132 | 43.6 | |
| General location of the symptoms (N=303) | |||
| Hip | 36 | 11.9 | |
| Knee | 59 | 19.5 | |
| Foot-ankle | 50 | 16.5 | |
| Other lower limbs | 26 | 8.6 | |
| Upper limbs | 66 | 21.8 | |
| Spine | 66 | 21.8 | |
| Pathology (n=303) | |||
| Orthopedics | 131 | 43.2 | |
| Traumatology | 172 | 56.8 | |
Judicial variables.
| Variable | Categories | Number | Percentage |
|---|---|---|---|
| Number of professionals involved (n=303) | |||
| One | 237 | 78.2 | |
| More than one | 49 | 16.2 | |
| Number not defined | 17 | 5.6 | |
| Type of professional sued (n=303) | |||
| Traumatologist | 287 | 94.7 | |
| Traumatologist+another physician | 11 | 3.6 | |
| Traumatologist+another type of professional | 5 | 1.7 | |
| General grounds alleged in the complaint (n=303) | |||
| Defective information | 45 | 14.9 | |
| Error in diagnosis | 52 | 17.2 | |
| Error in orthopedic therapy | 41 | 13.5 | |
| Error in surgical therapy | 114 | 37.6 | |
| Improper follow-up | 50 | 16.5 | |
| Wrong side | 1 | 0.3 | |
| Outcome of the harm sued for (n=303) | |||
| Death | 20 | 6.6 | |
| Bodily injuries | 270 | 89.1 | |
| Moral damages | 13 | 4.3 | |
| Economic amount of the suit (n=125) | |||
| <€50,000 | 27 | 21.6 | |
| €50,000–€100,000 | 42 | 33.6 | |
| >€100,000 | 56 | 44.8 | |
| Amount of the compensation (n=135) | |||
| <€50,000 | 71 | 52.6 | |
| €50,000–€100,000 | 38 | 28.1 | |
| >€100,000 | 26 | 19.3 | |
| Guilty verdict (n=303) | |||
| Yes | 151 | 49.8 | |
| No | 152 | 50.2 | |
| Finding as to costs (n=303) | |||
| Yes | 192 | 43.2 | |
| No | 111 | 56.8 | |
The civil jurisdiction was more frequently used to bring judicial complaints against traumatologists and orthopedic surgeons (88.4%), with the provincial courts of appeal handing down the largest number of judgments (75.9%).
The region of Spain with the largest number of judgments handed down is Catalonia (28.7%), followed by Madrid and Andalusia (11.6% each).
The area of health care most often involved was private medicine (63.75%).
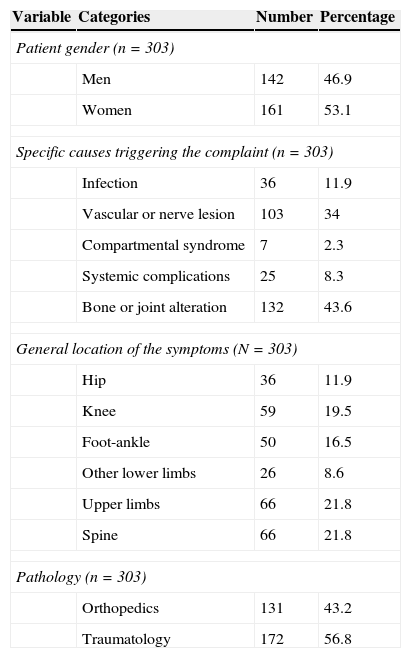
With regard to the gender of the patients involved, the proportion recorded was similar (46.9% men and 53.1% women).
The specific cause responsible for the largest number of court judgments was post-treatment osteoarticular alterations (43.6%), comprising alteration of joint mobility, residual pain, etc., followed by vascular or nerve lesion (34%) and infections (11.9%).Only a small percentage (2.3%) was due to a compartmental syndrome.
More often than not, the lesion referred to in the judicial complaint occurred in the lower limbs (56.5%), with the knee the area most frequently involved.
The etiology of the lesion was traumatic in 56.85% of cases and orthopedic (prosthetic surgery, non-traumatic bone deformities such as hallux valgus, non-traumatic pathologies of the spine, …) in 43.2%.
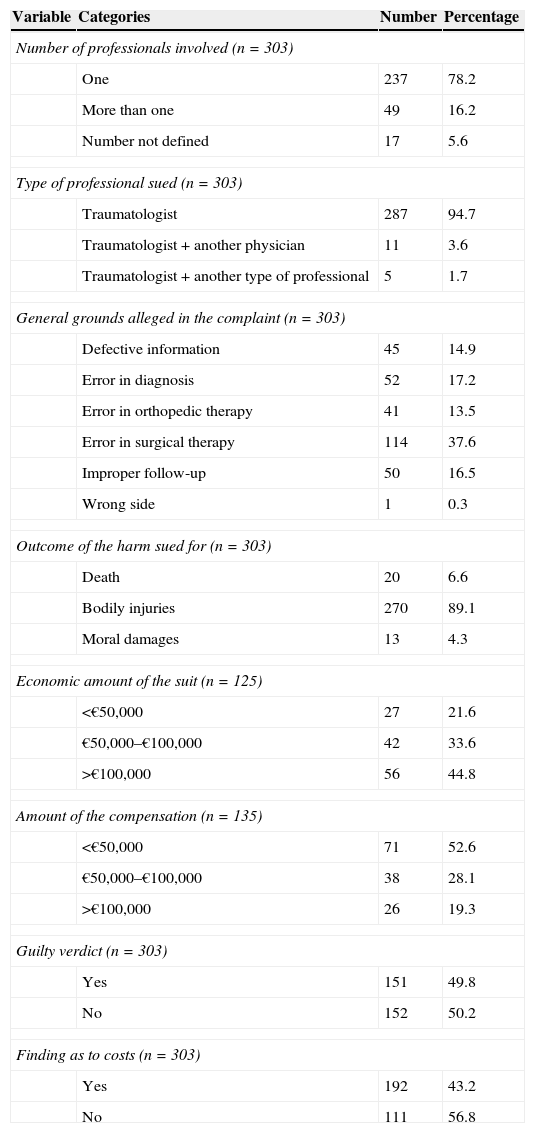
In the writ of complaint, the economic amount most often requested as compensation was greater than €100,000 (in 44.8% of cases).
In 94.7% of the cases, the complaint was brought against a specialist in traumatology in isolation and without the involvement of other physicians or other professionals. In addition, in 78.2% of the cases, only one professional was involved.
Within the general causes, the circumstance most often alleged in the judicial complaint in the second instance was an error in surgical therapy followed by error in diagnosis.
In a far from negligible 14.9% of cases, the fact giving rise to the complaint was a lack of informed consent (40 cases) or generic informed consent (5 cases).
The harm claimed for was, in 89.1% of the cases, bodily injury, followed by death in 6.6% and moral damages in 4.3%.
In the judgments handed down in the second instance, the court found against the medical practitioner in 49.8% of the Traumatology and Orthopedic Surgery cases, with the amount of the compensation awarded being less than €50,000 most times (52.6%).
The mean amount of the compensation was €81,767 with a maximum of €867,000 and a minimum of €600.
The two largest compensation awards were €800,000 and €867,000.
It is striking that, in both these rulings, the act complained about in the lawsuit was the non-existence of informed consent resulting in the death of the patient.
In the first case, the specific cause listed in the complaint was a vascular lesion in an orthopedic procedure on the knee and, in the second case, a nerve lesion in an orthopedic procedure on the lower spine.
The court ordered the payment of legal expenses in 43.2% of the cases.
With respect to the cross-tabbed contrast of variables through the χ2 test contingency tables, the following results stand out:
When relating the type of jurisdiction with the existence of a ruling against the practitioner, it is noteworthy that there is a smaller number of such rulings in the criminal jurisdiction and a larger number in the civil courts.
By crosstabbing the act complained about and the jurisdiction used, the outstanding statistically significant results are that the civil jurisdiction more often hears complaints regarding defective information while the administrative-dispute jurisdiction hears those for errors in diagnosis.
Comparing the act complained about and the existence of a ruling against the practitioner, there is a clear relationship between defective information and rulings against the practitioner.
In all 3 cases with a diagnosis of gaseous gangrene, the court's ruling went against the traumatologist.
It is also noteworthy that no ruling is handed down against the practitioner in most of the cases where the act complained about was an error in surgical or orthopedic therapy.
The data available in the comparison of health-care scope and the existence of malpractice rulings were not statistically significant but the crosstabbing of the health-care scope and the act complained about was significant, with a predominance of defective information and error in diagnosis in the private health-care area.
When comparing the act complained about and the amount of the award, smaller amounts (<€50,000) were observed in the case of errors in diagnosis, as opposed to moderate amounts (€50,000-€100,000) in the case of errors in surgical therapy.
No statistically significant results were observed with regard to the relationship between the specific cause and the existence of a ruling against the practitioner, but such results were evident in the crosstab between the specific cause and the amount of the award. Awards of >€100,000 were more common in the case of compartmental syndrome, whereas the awards were <€50,000 in residual osteoarticular alterations.
When the result was the death of the patient, compensation of less than €50,000 is unusual; however, in the case of moral damages, the compensation was for the most part less than €50,000.
DiscussionAn overall study of malpractice in traumatology and orthopedic surgery in Spain is a complex exercise.
In order to assess the problem from a global perspective, we would need to have data available on first instance judgments, appeals in the second instance, extra-judicial complaints, etc. but there is no national archive reflecting these data, and the creation of more complete databases would be very desirable.2,12
Different perspectives can be applied to approach this problem:
- -
Studies by insurance companies.
- -
Studies by professional medical associations.
- -
Studies of judgments.
- -
Hospital complaints.
Although, obviously, none of these approaches studies the problem at a global level, they do provide us with very useful information for use in day-to-day medical practice of traumatology.
Apart from the purely traumatological perspective, we also have studies available on adverse effects and clinical safety that are useful to identify potential health risks closely related to future complaints for medical negligence14 as well as studies from the legal perspective of the judges themselves, aimed more at defining medical imprudence and its various degrees.15
Traumatology and Orthopedic Surgery is a speciality entailing a high degree of litigation risk.
In the study carried out on the complaints submitted to the National Medical Arbitration Commission16 in Mexico City, 282 cases were assigned to the speciality of Traumatology and Orthopedics out of a total number of 1925 complaints, implying 14.64%. This figure is in percentage terms similar to that of our series (15.69%)2,17 although the complaints involving our speciality ranked first in the total of complaints lodged by specialities in Spain over Gynecology-Obstetrics.
Álvarez González et al.18 came to the same conclusion in this regard when they used data from the Legal Medicine Institute in Málaga on malpractice complaints in this province. They noted that, by speciality, Traumatology was ranked first.
In Catalonia, more centralized studies have been carried out under the auspices of the professional associations of physicians in Catalonia. Using data on 24,000 insured physicians for the period from 1986 to 2005, it was found that 5246 complaints were lodged and the conclusion12 was that 1.33% of all physicians insured had to face some kind of complaint although only 0.26% had to pay any compensation to the party bringing the lawsuit.
This finding is very different from the number of rulings against medical practitioners reflected in our series of second instance judgments where the rulings against medical practitioners came to 49.8% of the cases as our series covers more complex cases requiring the use of the courts and of the just in the first instance but also a subsequent review in a higher court.
Even so, both series reflect compensation awards habitually less than €50,00012 (in our series, 52.6% of the rulings awarded less than €50,000).
In our study, the mean cost of the compensation awards is €81,767 with a maximum of €867,000 and a minimum of €600, to which we should add the cost of legal fees that were ordered to be paid in 43.2% of the proceedings. In a recent study published in the New England Journal of Medicine19 on the risk of malpractice by specialities, the mean compensation award, considering all the specialities receiving complaints, came to $274,887 (€207,350), a figure therefore far higher than in our cases.
Insurance companies mostly establish a compensation cap of €600,000 per claim, so the professional is in most cases covered by the insurance in place. Traumatology and Orthopedic Surgery is, however, one of the few specialities where this limit is exceeded, albeit only in 0.6% of cases.
The permanent sequelae (89.1%) most commonly referred to in the lawsuits are death (6.6%), a percentage clearly lower than that recorded in other medical or surgical specialities (Neurosurgery, Psychiatry), probably related to the kind of pathologies diagnosed and treated in traumatology, where the risk to life (excepting polytraumatized patients) is frequently less than in other specialities.
The fact that a patient dies does not tip the balance toward a ruling against the medical practitioner as might be expected and as happens in other specialities (similar ratios between rulings against and in favor of the traumatologist) but such an outcome does have a great impact on the quantification of the compensation which is logically higher in most cases, even sometimes reaching €800,000.
Rulings awarding moral damages (4.3%) are not very relevant in traumatology.
In our series, most of the legal claims that were successful sought economic compensation and 88.4% were brought in the civil courts, with only 5.9% brought in a criminal jurisdiction. This study considers the judgments against traumatologists in the second or later instance, which means that many criminal lawsuits are either not admitted for consideration and are dismissed or else the medical practitioner is not found guilty in the first instance, as the total volume of claims lodged before the criminal courts is far higher.
In this sense, our data can be superimposed, within the European area, on those obtained in Italy,20 where most of the lawsuits brought were solely for compensation.
- -
The private health-care sector gives rise more frequently to complaints (over 60% of cases), probably due to the profile of users of private medicine who often view the payment for services as a guarantee of the outcome.
- -
With regard to the reasons for the lawsuits, errors in surgical therapy were the most common (37.6% of cases), followed by errors in diagnosis and poor follow-up of the patient.
If we add together the errors in orthopedic and surgical therapy, the percentage amounts to 51%, i.e. more than half the complaints related to treatment errors.
Defective information or communication is the reason alleged for bringing a lawsuit in 14.9% of the cases and in 77.8% of these, they were followed by a ruling against the traumatologist. This finding must strengthen the voices advocating the relationship between safe medical practice and good communications with patients.
In this sense, an informed consent21 document in which the patients set down in writing that they have been duly informed and that they consent to the procedure does not prevent lawsuits but can aggravate them. We must not focus solely on the signing of the informed consent form as a document that can be shown not to have been understood by the patient or that was completed in a rush or without proper anticipation can be invalidated,8 so it is fundamental to reflect on patients’ case notes that information about the procedure to be performed and its possible complications has been given and that this has been understood. Poor or insufficient communication with patients enormously increases the risk of being sued.
An analysis of lawsuits brought in the United States showed that an independent factor distinguishing between the existence or otherwise of formal complaints was the number of minutes dedicated to the interview by the physician, with an average of 15.0 in those facing lawsuits versus 18.3 in those not sued. Factors involved in relationships between physicians and patients, such as tone of voice, also seem to be decisive.
- -
The specific symptom or process suffered by the patient lodging the lawsuit was, in most cases, an osteoarticular alteration following treatment (43.6%), consisting in a loss of joint mobility, residual pain, etc., followed by vascular or nerve lesion (34%) and infection in 11.9% of cases.
When the infection was gaseous gangrene due to Clostridium perfringens, the court ruling went against the medical practitioner in 100% of the cases versus 58% for the total of all infections.
In the case of neurovascular lesions, the ruling against the medical practitioner occurred in 55% of cases.
For compartmental syndromes, the ruling went against the medical practitioner in 57% of cases, with compensation of >€100,000 being awarded in 75% of cases, probably related to the disabling sequelae following such syndromes.
- -
The largest number of complaints brought involved the lower limbs (56.5%), with the knee being most often involved.
With the results obtained in our study of second-instance reviews of judgments, we can describe a profile in traumatology and orthopedic surgery with a particularly strong tendency for more medical complaints. Thus, orthopedic surgeons must maximize the precautions adopted in our day-to-day activities with:
- -
Patients using private health care.
- -
Patients belonging to the Catalan or Madrid regions.
- -
Patients undergoing surgery for orthopedic or traumatological pathologies.
- -
Locations involving the spine or legs.
- -
Unsatisfactory outcome following surgery.
- -
Patients who have not been correctly informed or have not perceived a fluid communication and relationship with their physician.
- -
As a speciality, Traumatology and Orthopedic Surgery tends to receive more complaints for malpractice in traumatological cases rather than in orthopedic practice.
- -
The number of rulings against traumatologists is high but the compensation awarded tend mostly to be less than €50,000 and are covered in most cases by the insurance policies taken out by medical professionals.
- -
The fundamental reason for patient complaints is an error in surgical therapy, so the surgical operation is fundamental and this is where all possible precautions must be taken.
- -
Court judgments against medical practitioners for a lack of information or poor communication are very high and so it is important to encourage adequate communication between doctors and their patients and also to fill in correctly the informed consent document, making sure that the patient has understood the procedure to be performed and its potential complications; it is appropriate to add a reference to these discussions in the case file.
- -
The largest number of complaints has to do with obtaining compensation, especially in private practice, with a predominance of claims brought in the civil courts; for this reason, it is essential to have third-party liability insurance in place for retroactive cover and to keep the cover in place over a long period of time.
- -
The most serious processes such as gaseous gangrene, compartmental syndrome, etc., where the speed of diagnosis and treatment are fundamental, are the basis for a large number of rulings finding against traumatologists.
Our study only takes into account the court judgments handed down in the second instance, without any consideration being given to judgments handed down in the first instance nor to those complaints against traumatologists in which a settlement is reached out of court.
Such data would have been a perfect complement to the present study to evaluate globally and more completely the malpractice complaints lodged against traumatologists and orthopedic surgeons but it has not been possible to include these as there is no national archive collating them.
In this sense, Spanish authors2,12 have underlined the need for databases as well as more local and national studies.
Ethical responsibilitiesProtection of persons and animalsThe authors state that no experiments have been performed in this research on humans or on animals.
Data confidentialityThe authors state that they have followed the protocols of their work center with regard to the publication of patient details.
Right to privacy and informed consentThe authors state that they no patient data appear in this article.
Level of evidenceLevel of evidence III.
Conflict of interestThe authors state that they have no conflicts of interest to declare.
Please cite this article as: Cardoso-Cita Z, Perea-Pérez B, Albarrán-Juan ME, Labajo-González ME, López-Durán L, Marco-Martínez F, et al. Análisis de sentencias judiciales relativas a negligencias médicas emitidas contra traumatólogos entre 1995 y 2011. Rev Esp Cir Ortop Traumatol. 2015;60:29–37.
