





Pronator syndrome has classically required open surgery that leaves a large scar; initial endoscopic techniques required approaches of an average 4cm without achieving release of all structures. The purpose of this study was to describe a new endoscopic approach that allows the median nerve to be safely and completely decompressed, leaving a smaller and less visible scar.
MethodsDescription of a new approach for decompression of the median nerve in the proximal third of the forearm with minimal incision and endoscopic technique in cryopreserved cadaveric specimens, describing incision, endoscopic anatomy, safe corridors and decompression sites.
ResultsIn 20 elbows of cadavers, an endoscopic approach of the median nerve in the proximal forearm with a 4mm endoscope and 0° of angulation was performed. The advantages and limitations of the technique and surgical details are presented for release in the most common compression points of the nerve in the forearm. We performed this technique in 3 patients with good results without complications.
DiscussionRelease of the median nerve and section of potential aponeurotic compression structures by endoscopy is possible. The ulnar head of the pronator and the aponeurotic arch of the flexor digitorum superficialis are frequently implicated in the syndrome. The scar is aesthetically good. It is a relatively new technique, with lower morbidity that allows faster recovery of patients.
ConclusionsIt is possible to perform a complete decompression of the median nerve in the forearm using an endoscopic approach, safely with lower comorbidity for the patient.
El síndrome de pronador ha requerido clásicamente de una cirugía abierta que deja gran cicatriz; técnicas endoscópicas iniciales requerían abordajes de 4cm en promedio y sin lograr una liberación de todas las estructuras. El propósito de este estudio es describir un nuevo abordaje endoscópico que permita descomprimir el nervio mediano de forma segura y completa con una cicatriz de menor tamaño y menos visible.
MétodosDescripción de una nueva técnica de descompresión del nervio mediano en el tercio proximal del antebrazo con incisión mínima y técnica endoscópica en especímenes cadavéricos criopreservados, describiendo incisión, anatomía endoscópica, corredores seguros y sitios de descompresión.
ResultadosSe realizó en 20 codos de cadáveres abordaje endoscópico del nervio mediano en el antebrazo proximal con endoscopio de 4mm y 0° de angulación. Se presentan ventajas y limitaciones de la técnica y detalles quirúrgicos para la liberación en los puntos de compresión más comunes del nervio en el antebrazo. Realizamos en 3 pacientes esta técnica con buenos resultados sin complicaciones.
DiscusiónEs posible una liberación del nervio mediano y sección de estructuras aponeuróticas potenciales de compresión por endoscopia. La cabeza cubital del pronador y la arcada aponeurótica del flexor digitorum superficialis están implicados frecuentemente en el síndrome. La cicatriz es estéticamente buena. Es una técnica relativamente nueva, con menor morbilidad que permite una recuperación más rápida de los pacientes.
ConclusionesEs posible realizar una descompresión completa del nervio mediano en el antebrazo con técnica endoscópica, segura y menor comorbilidad para el paciente.
Pronator syndrome or proximal compressive neuropathy of the median nerve (MN) in the forearm, initially described in 1951 by Seyffarth,1 includes symptoms such as pain in the volar surface of the forearm, paresthesias in MN distribution and reduction of grip strength. In 1952 Kiloh and Nevin2 described the syndrome caused by isolated compression of the anterior interosseous nerve (AIN) in the forearm. Proximal nerve compression of the MN in the forearm has a low prevalence and it is difficult to differentiate from carpal tunnel síndrome (CTS). Five proximal to distal compression sites have been described: the ligament of Struthers, bicipital aponeurosis (a.k.a. lacertus fibrosus (LF), vascular arches, the fibrous band of the pronator teres muscle (PT) and the fibrous arch of the flexor digitorum superficialis muscle (FDS).3
The syndrome may be caused by stretching, bruising, supracondylar fractures of the humerus, infection, neuritis, tumour compression anomalous vascular formations or aponeurotic bands of the FDS or the PT.4
Most of reported cases in the literature describe a fibrous band between the two muscle heads of the PT as the cause of compression.3
Surgery of this pathology is performed when physical therapy, activity modifications and analgesia are unable to provide favourable outcomes for a prolonged period.5 Decompression has classically been described using a longitudinal, transverse or s-shaped incision, which are large in size so as to reach all compression points. Different authors report good functional outcomes in long-term follow-up.4
Nowadays endoscopic decompression of different peripheral entrapment neuropathies—for example in CTS,6 cubital tunnel syndrome7,8 and tarsus tunnel syndrome—are performed routinely and with favourable outcomes. For some 5 years the possibility of performing endoscopic release of the median nerve in the forearm has been proposed9 and several authors have reported short series with improvement of functional scales of up to 62%.10,11
Using a minimal approach and endoscopic technique it is possible to decompress the MN in all the points mentioned without the need for exposure using an extensive standard incision.12
The aim of this study was to describe the surgical approach for the release of the MN in the proximal third of the forearm using an endoscopic technique, and its clinical usage.
Materials and methodsDescriptive study of anatomical research on the elbows of fresh cadavers over 18 years of age who did not present with alterations of the anatomical site under study, supplied randomly and with a convenience sample size.
Inclusion criteria: fresh cadavers taken randomly from the Latin American Centre for Research and Training in Minimally Invasive Surgery (CLEMI for its initials in Spanish).
Cadavers under 18 years of age or those presenting with alterations in the anatomical site under study were excluded.
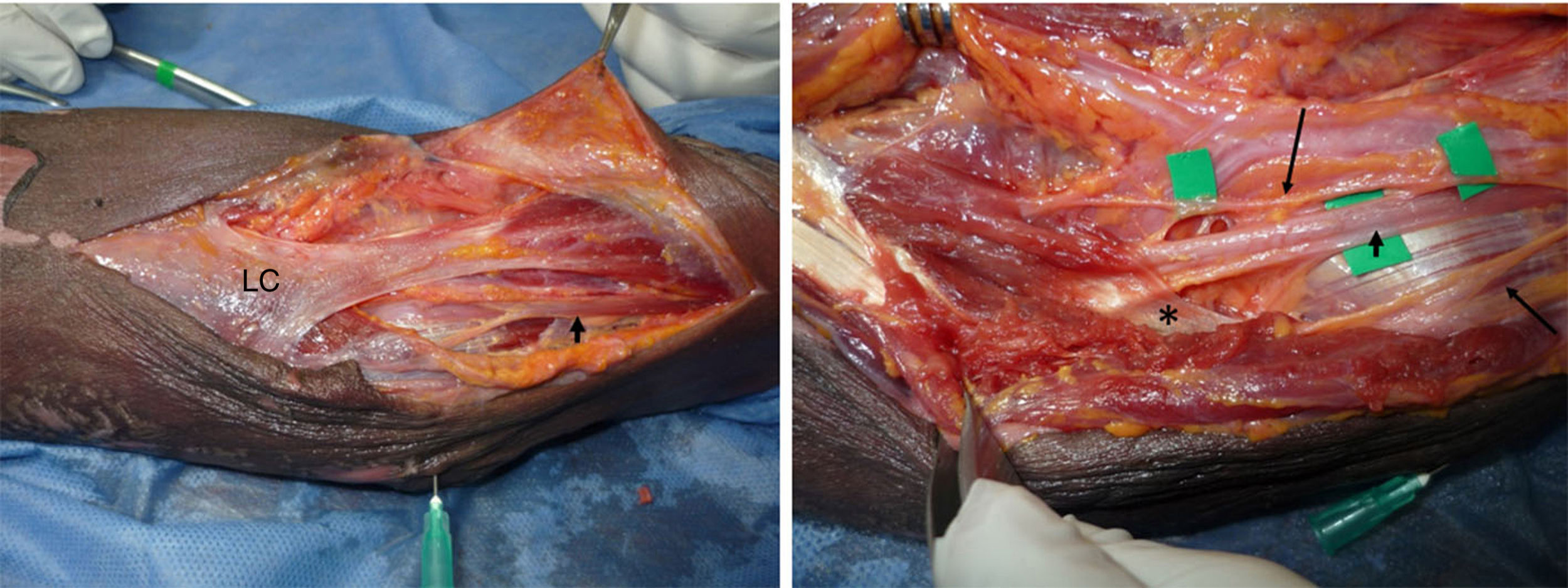
Four mm 0° and 30° endoscopies were used for the research. An open approach with additional endoscopy was used in a pilot study to accurately mark the sites to be dissected and endoscopically released (Figs. 1 and 2).
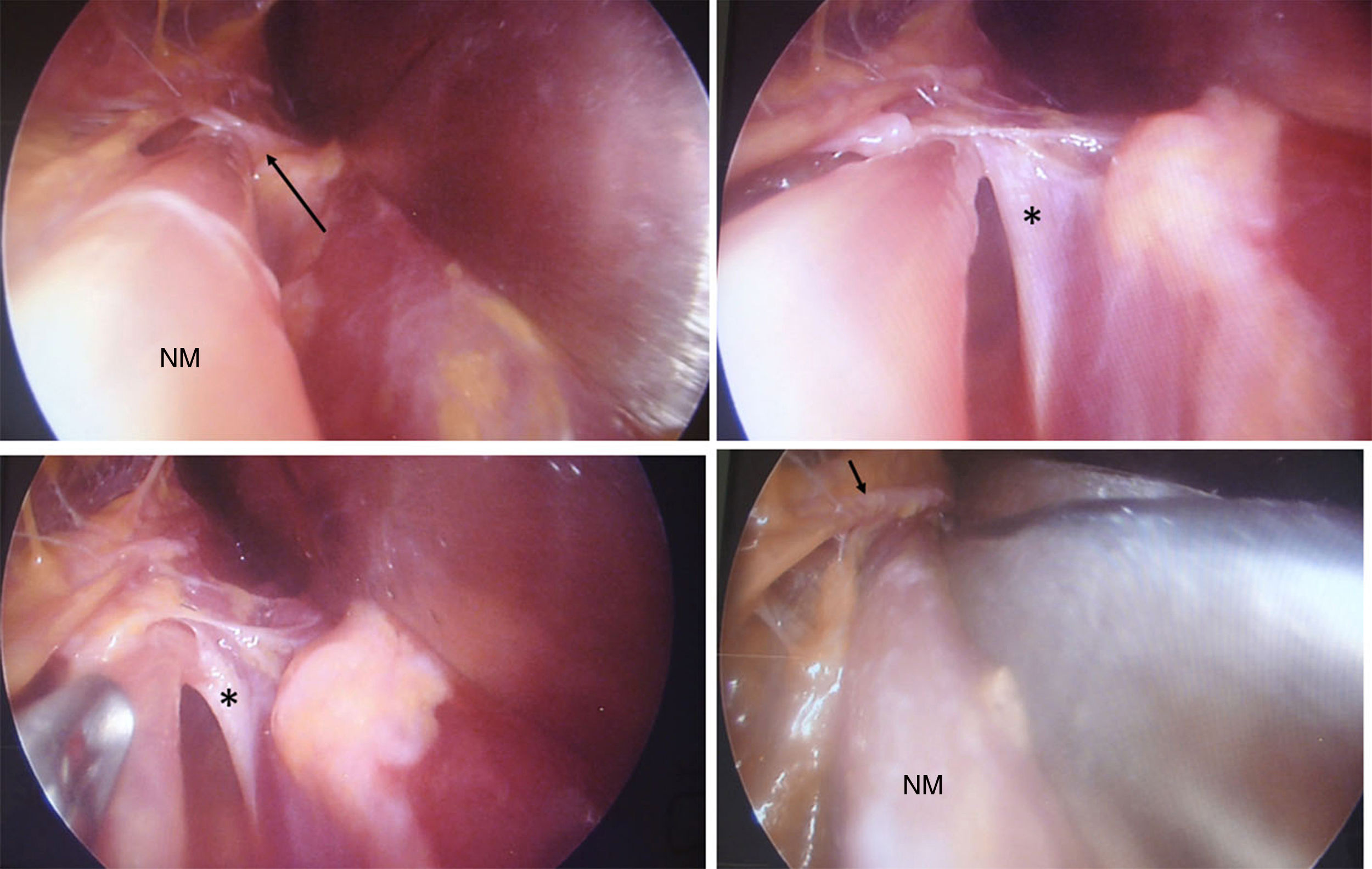
. Right: lifting the LC the MN is observed penetrating under the deep fascia of the PT (asterisk). Branches for the PT muscle are observed (long black arrows). The brachial artery is found lateral to the MN.")
Proximal third dissection of the forearm. Distal: left. LC: lacertus fibrosus, underneath of which is the MN (short black arrow). Right: lifting the LC the MN is observed penetrating under the deep fascia of the PT (asterisk). Branches for the PT muscle are observed (long black arrows). The brachial artery is found lateral to the MN.

This study was conducted in compliance with the ethical regulations of the declaration of Helsinki and was approved by the university ethics committee where the study was based. The authors declare that they have no conflict of interests in conducting this study and did not receive any sources of financing.
ResultsAn anatomical study was conducted on 20 elbows of 11 cadaveric specimens for endoscopic dissection of the MN to achieve its decompression in the elbow and the proximal third of the forearm.
Supine positioned, with surgeon positioned medial to the elbow and assistant on the contralateral side. Marking of anatomical references: limb extended on hand table, surgeon located medially to the elbows and assistant contralaterally. Marking of anatomical references: epitrochlear, lateral epicondyle, interepicondylar line and biceps tendon.
A transversal approach on the elbow crease of 2.5cm was made from the cubital edge of the biceps tendon towards the medial epicondyle with subsequent dissection and retraction of the branches of the medial forearm cutaneous nerve and of the basilic vein.
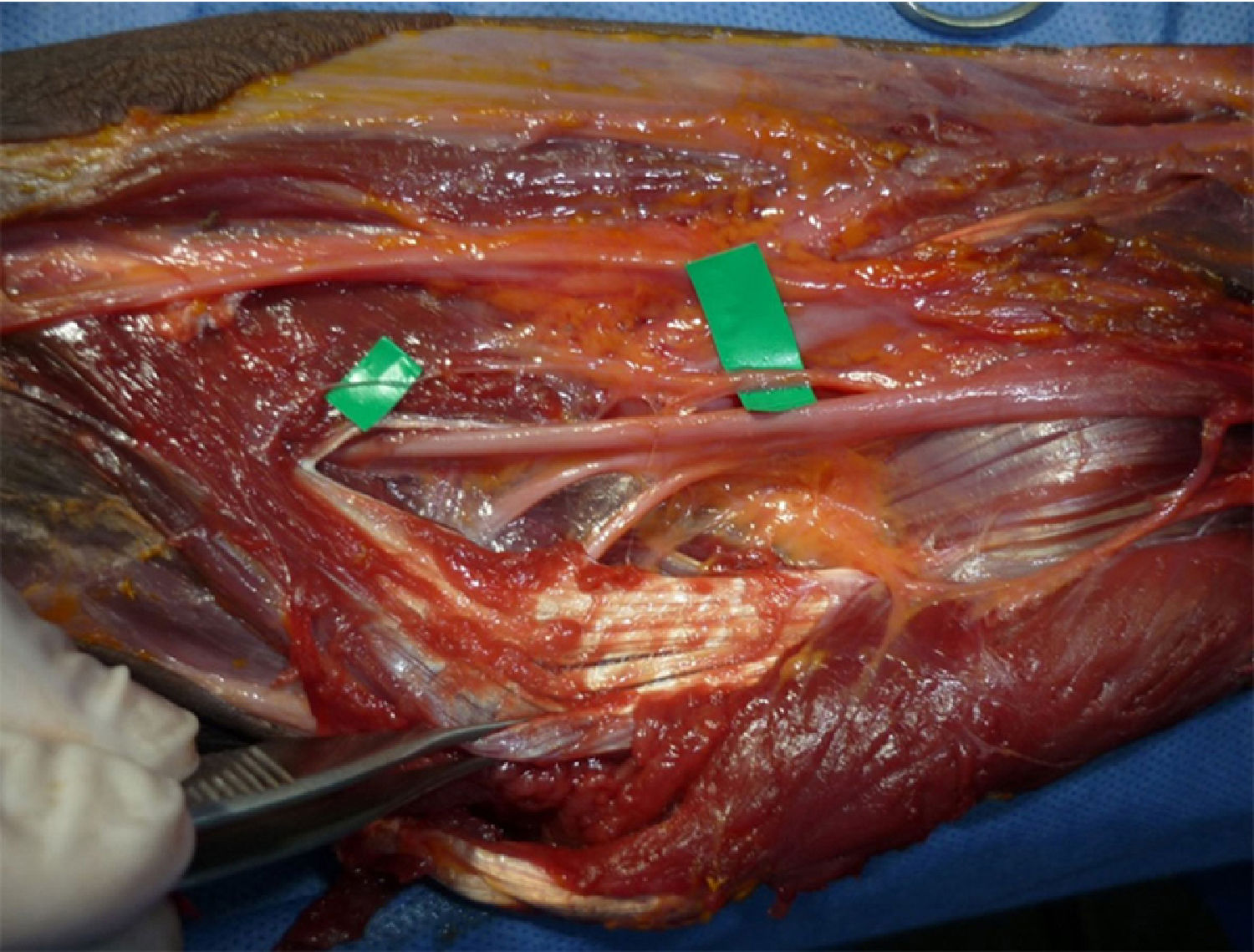
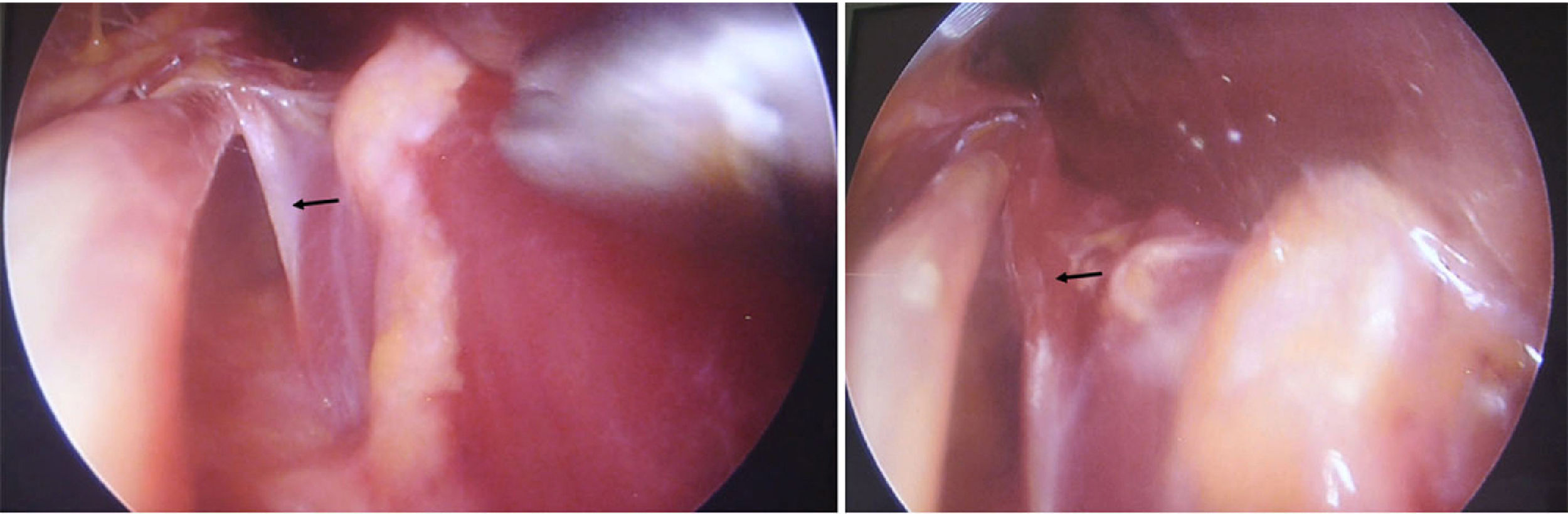
The LF was immediately located, and sectioned. The PT muscle was then retracted medically and the brachial biceps laterally exposing the vascular nerve structures (Figs. 3 and 4). Blunt dissection was then performed to identify the MN, which was found medially and deeply to the brachial artery. Identification of possible vascular arcades, coagulation or ligature and cutting of the same. All of these steps were performed under direct observation.
 and dissection and sectioning of the lacertus fibrosus (arrow head).")

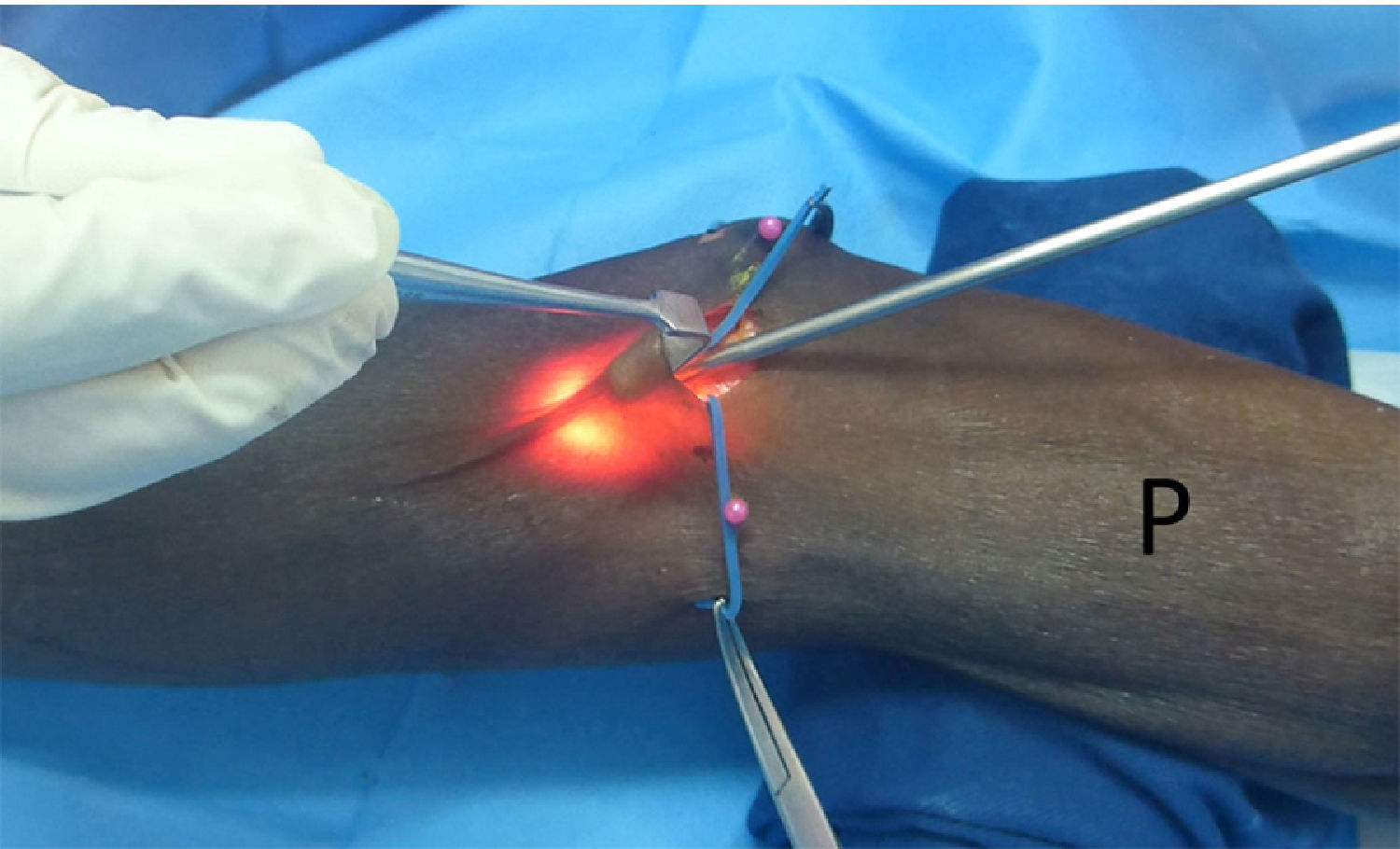
A narrow, long branched separator was then used by the assistant to improve the field distally and provide sharper viewing of the MN at the beginning of the endoscopy insertion. For complete proximal and distal release we used endoscopy lenses of 0° and 30°. Finally, after the initial tests the one which showed the best results was the 4mm with 0° angulation (Fig. 5).

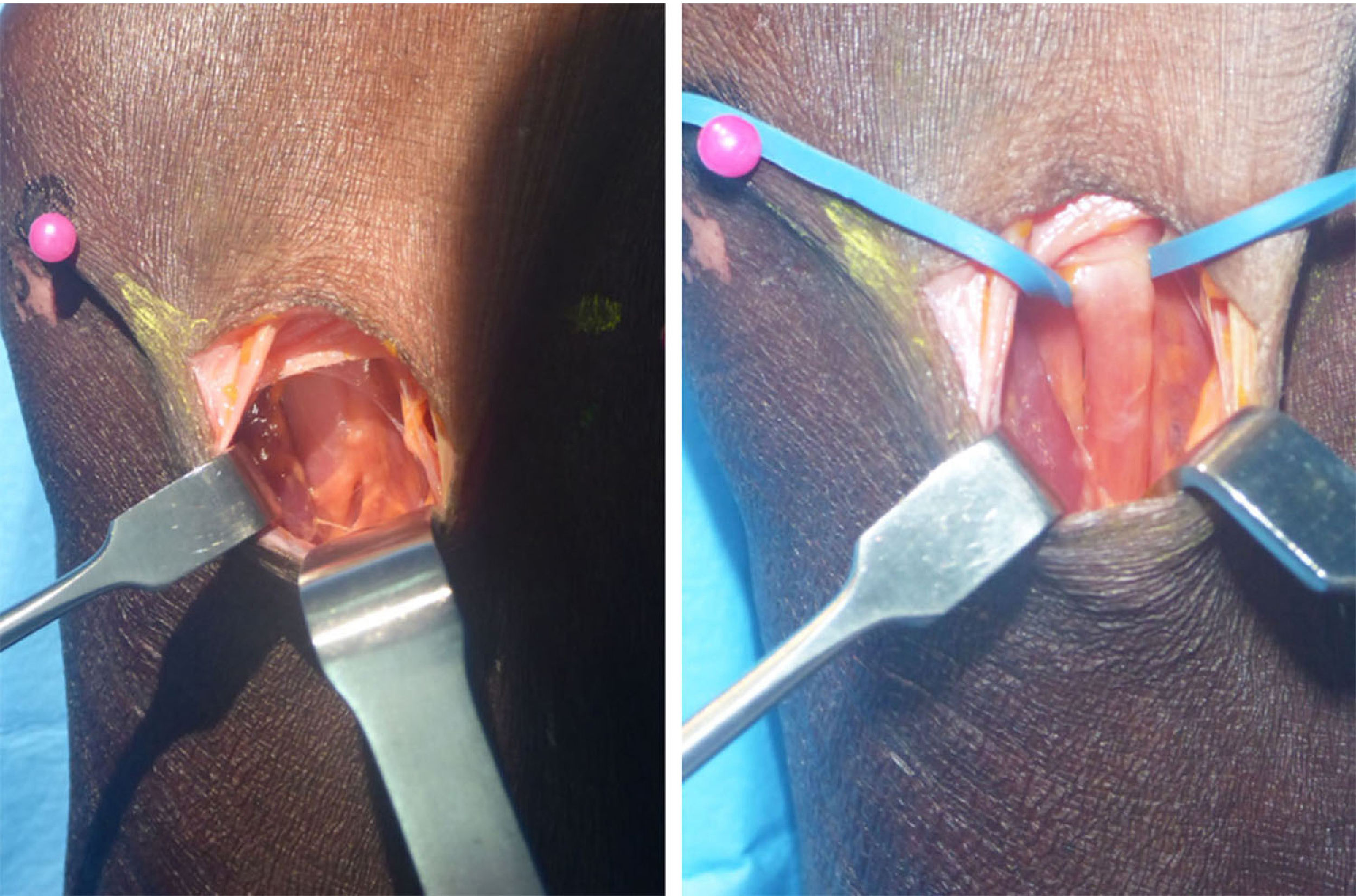
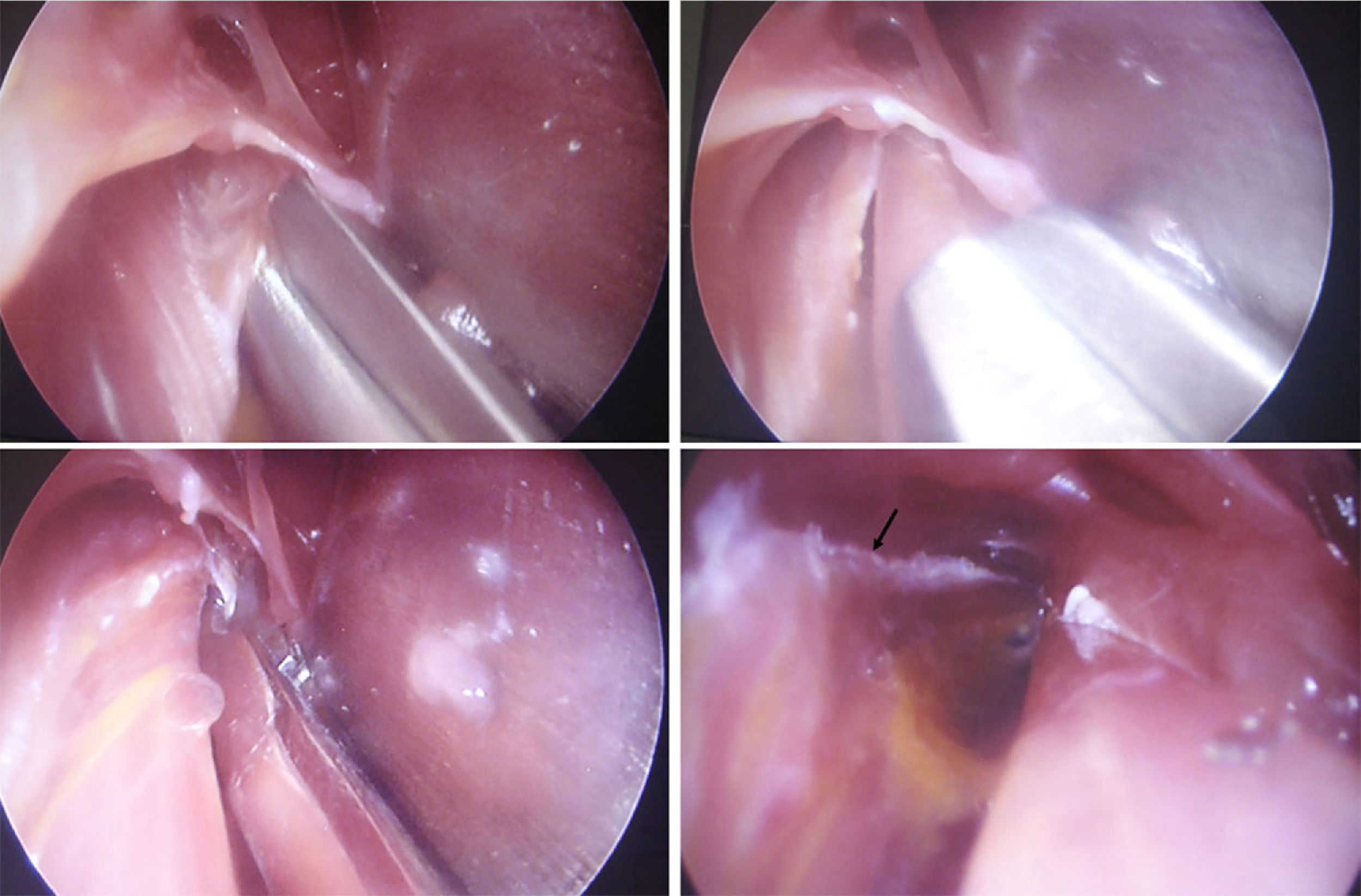
For dissection and release of both the PT and the FSA arcade, the separator traction made it possible to divide the muscle and nerve levels with greater clarity facilitating the procedure. The fibrous band of the PT muscle was located and a progressive dissection of it was performed with curved, long and thin arthroscopic or Metzenbaum scissors. Identification was then made and sectioning of the fibrous arcade of the FDS muscle. Then, with digital dissection and the help of the separator an approach proximal to the incisions towards the arm was made to verify the presence of the ligament of Struthers, achieving complete release of the MN in this way in all possible compression points (Figs. 6–9).

 appears which is sectioned with thin blunt scissors (short arrow).")


Complete release was possible in all cases.
After the endoscopic approach had been performed, the cubital fossa was explored by open surgery to assess the result. Sufficient distal release was confirmed, and even the fibrous arcade of the FDS which is the most distal structure of the dissection was reached.
In this way an endoscopic MN releasing technique in the proximal compression in the forearm was standardised to be used in clinical practice.
We used this technique in 3 clinical cases, with good outcomes and with no complications.
DiscussionPronator syndrome or proximal compressive neuropathy of the median nerve (MN) in the forearm, presents with symptoms such as pain in the volar side of the forearm, paresthesias in MN distribution and reduction of grip strength. This pathology is low in prevalence and is difficult to differentiate from CTS.
Multiple compression sites of the MN9 have been described: the ligament of Struthers is the most proximal compression site and connects the supracondylar process to the epitrochlear, trapping the MN and the brachial artery. It is observed in approximately 13% of the general population and rarely leads to symptoms. The LF (bicipital aponeurosis) is the least frequent cause of the pronator syndrome. The LF is the medial extension of the biceps and covers the MN and the brachial artery in the internal bicipital corridor. Compression may be secondary to hypertrophy or anomalies of the aponeurosis.13 The fibrous bands between the deep and superficial heads of the PT are frequently cause of compression of the MN and the AIN. The cubital head of the PT has been most commonly reported as the greatest cause of entrapment and is also where the most anatomical variations are to be found.
Several variants have been described which range from just a muscular head, a fibro muscular head and a highly fibrotic or aponeurotic head. A short cubital and tendinous head has also been found, or joined to the FDA arch, or with three origins and a humeral head perforated by the MN. The FDS muscle varies in its origin and size, and the MN may be compressed by one or two aponeurotic arches of this muscle.14
Pronator syndrome symptoms may be confused with other entrapment pathologies, being erroneously diagnosed as CTS in up to 50% of cases.14 The clinical symptoms of the pronator syndrome are hypoesthesia of the hand in the median region (58%), reduction of the strength of the flexor muscles of the fingers and of the hand (49%), pain in the forearm (39%), paresthesia (25%), positive tunnel sign on the PT (7%) and nocturnal paresthesia (2%).15
The electromiography with neuroconduction speeds may be useful in some cases. Magnetic resonance may show changes in signal intensity in T2 with fat suppression.
Surgical treatment outcomes of the release of the pronator syndrome were not as good as those of the CTS. The cause of this is not clear but is probably due to the appearance of MN adherences in the surgical release site, an incomplete release, or the nerve’s many ramifications, which increase the difficulty of its release.
Classically surgical treatment was performed of the entrapment of the MN in the proximal third of the forearm using open surgery.16
Hsiao et al.17 studied 21 cases with simultaneous presentation of CTS and pronator syndrome and considered the principal factor in diagnosing two-point compression to be the appearance of paresthesias in the thenar eminence and pain in the proximal portion of the forearm associated with nocturnal paresthesias. Endo scopic release of the carpal tunnel endoscopy and open surgical release of the PT were performed and when comparing them with their cases of carpal tunnel research they found that 6% of patients with CTS also had PT level compression. At the time of release 28.57% of patients presented with entrapment of the bicipital aponeurosis, 47.6% between the humeral and cubital heads of the PT and 23.8% in the aponeurotic arch of the FDS; 71% of patients reported that they were free from pain, paresthesias and loss of sensitivity, with improvement of strength and 6 patients presented with occasional paresthesia and pain without loss of sensitivity, with strength <50% compared with the contralateral hand. They thus highlighted the importance of considering a diagnosis of double entrapment, pronator syndrome with suspected CTS in many patients.
Luangjarmekorn et al.18 compared the treatment outcomes of patients with a history of unsuccessful release of the CTS with suspicion of pronator syndrome concurrent with surgical review of simultaneous release of the PT versus release of only carpal tunnel syndrome. They found there was a greater possibility of complete recovery of hypoesthesia (60% vs. 0%) and pain (55% vs. 0%) in patients in whom the PT had been relapsed. Compression was found in 90% of cases in the deep head of the PT and in 50% in the LF. Release was performed using an open technique, with a double approach in the proximal portion of the forearm or a classical long incision.
Hagert19 carried out a prospective study with 44 patients with proximal entrapment of the MN and used a minimally invasive surgical technique, local anaesthesia with lidocain and epinephrine and no tourniquet (wide-awake technique), with significant improvement in functional score. He performed surgery of 2–3cm transversally in the cubital fossa, only releasing the LF.
Zancolli et al.20 published a minimally invasive surgical technique using a 3.5cm oblique approach, 6cm distal to the epitrochlear on the fexopronator table, dissecting through the superficial fascia sectioning the septum between the PT and the flexor carpis radialis to access the deep fascia of the superficial head of the PT and decompress the MN. They described 44 cases treated with this technique with disappearance of symptoms in 93% of cases. One disadvantages is that this technique does not allow for the release of other more proximal compression sites such as the ligament of Struthers or the LF, and requires major anatomical knowledge to identify the intermuscular septa which are not always very visible and to perform extensive transmuscular dissection.
In 2011 Keiner et al.9 were the first to propose the possibility of making an endoscopic release of the AIN. One cadaveric study describes a 4cm incision in the forearm where the MN and division of the AIN may be viewed, performing distal release, but in one in vivo case this required a 5cm approach to achieve release. Unlike our technique, it uses a longitudinal approach which is less aesthetic, without proximal exploration or release and also using a 30° lens which in our case we found hindered technique and limited suitable observation of the surgical field.
Lee et al.10 then published the first study in vivo with follow-up of endoscopic surgical interventions for the release of the pronator syndrome, in which they reported 14 cases, excluding patients with concomitant CTS or other neuropathies, with an average follow-up of 22months and improvement on the functional scale. They performed a longitudinal incision of 3cm distal to the cubital fossa, involving the LF, proximal and distal blunt dissection under direct observation, haemostasis of the vascular arcades with bipolar and proximal release of the bicipital aponeurosis and the ligament of Struthers if they were present. Distal release was made under endoscopic guidance cutting the fibrous band of the PT and the FDS.10 The advantages of this technique is that it provides good visualisation with a small incision and with less postoperative pain. Its limitation is that it could not be compared to a control group with open surgical release.
It is believed that endoscopic release leads to faster recovery, less pain and a smaller scar, although this has yet to be demonstrated with larger studies. Prospective controlled randomised studies with long-term follow-up are required to support the hypothesis put forward on the success of MN endoscopic release.
In 2014 Leclère et al.12 demonstrated the surgical technique using an endoscopy at 30°, with bipolar cautery. They also performed a 3cm longitudinal incision, carrying out the technique on two patients in a similar way to that described by Lee with improvement of the functional scale.
The difference with our study is mainly due to the type of approach used: they carried out a longitudinal approach on the forearm and we used a transversal approach in the cubital fold. Both lead to excellent viewing but the transverse approach is aesthetically better because it over the elbow crease.
One of the advantages of endoscopic approach in the proximal third of the forearm is the fact that it leads to a less traumatic dissection, does not require the dissection of muscles which play no part in this pathology, allows for the assessment of all compression sites and the safe anatomical corridors are easy to identify and follow. All of this reduces the risk of complications and preserves the advantage of a minimally invasive technique and with an aesthetically good result. Probable complications are lesion of the brachial artery due to poor technique or vascular anomaly and incomplete release of the MN in the proximal forearm.
Endoscopic release is not indicated in patients who have previously had surgery in the proximal third of the forearm.
This technique is easily reproducible.
ConclusionsClear knowledge of the anatomy of the cubital fossa is necessary, particularly relating to the MN with the brachial artery to prevent iatrogenic lesions.
Our procedure shows that it is possible to achieve complete decompression of the MN in the proximal forearm using a minimum approach and it is aesthetically better than procedures previously published in the literature.
Randomised and comparative prospective studies need to be conducted with a classical open approach to assess the long-term functional results of endoscopic treatment of the proximal entrapment of the MN.
Level of evidenceLevel of evidence type III
FinancingWe received no financing
Conflict of interestsWe have no conflict of interests to declare.
Please cite this article as: Vergara-Amador E, Castillo-Pérez S, Tovar-Cuellar W. Liberación endoscópica del nervio mediano en el tercio proximal del antebrazo. Nuevo abordaje. Rev Esp Cir Ortop Traumatol. 2019;63:439–446.
