



To analyse a series of patients with bone tumours reconstructed with modular prostheses and to evaluate: (1) Survival of the implant. (2) Causes of failure. (3) Complication rates. (4) Limb salvage overall survival. (5) Functional results and full weight bearing.
Materials and methodsA retrospective study from longitudinally maintained oncology databases was undertaken. All patients with bone tumours reconstructed with endoprosthesis were analysed. A total of 106 patients matched the inclusion criteria. They were divided into groups: group 1, primary bone tumours; group 2, bone metastasis; group 3, osteoarticular allograft reconstruction revisions. The type of failures were classified according to Henderson et al. (2014) and functional results assessed by the Musculoskeletal Tumor Society (MSTS). Demographic analysis, survival and the differences between groups were recorded.
ResultThe mean follow-up of the patients was 68 months. Mean age was 43 years. Overall implant survival was 86.4% at 2 years (95% CI: 79–94) and 73% at 5 years (95% CI: 60–80). Nineteen patients (18%) developed a prosthetic failure. The limb salvage overall survival was 96% at 5 years (95% CI: 91–99). The mean functional results according to the MSTS was 24 and mean time to full weight bearing was 2.3 weeks.
ConclusionsLimb conservation surgery and endosprosthetic reconstruction is a valid option for patients with bone tumours with failure rates similar to other reconstruction methods.
Analizar una serie de pacientes oncológicos tratados con prótesis modulares y evaluar: 1) Supervivencia del implante. 2) Causas de fracaso. 3) Tasa de reintervención. 4) Supervivencia del miembro. 5) Resultados funcionales y tiempo hasta la carga completa.
Materiales y métodosSe realizó una búsqueda retrospectiva en una base de datos oncológica entre marzo de 2001 y agosto de 2015 de pacientes con tumores óseos y pacientes con cirugía de revisión de trasplantes óseos reconstruidos con endoprótesis. Se incluyó a 106 pacientes con seguimiento mínimo de 2 años. Se dividió la población en 3 grupos: grupo 1, tumores óseos primarios; grupo 2, metástasis ósea; grupo 3, revisiones de trasplantes óseos masivos. Las causas de fracasos fueron clasificadas según Henderson et al. (2014) y la funcionalidad se evaluó según el la escala de la Musculoskeletal Tumor Society (MSTS). Se realizó análisis demográfico, estimación de la supervivencia y se compararon las diferencias entre grupos.
ResultadosEl seguimiento medio de los pacientes fue de 68 meses. La edad promedio fue de 43 años. La supervivencia global del implante fue del 86% a 2 años (IC 95%: 79-94) y del 73% a 5 años (IC 95%: 60-80). Diecinueve pacientes (18%) presentaron fracaso protésico, con revisión. La conservación del miembro en nuestra serie fue del 96% a 5 años (IC 95%: 91-99). Los resultados funcionales promedio según la escala de la MSTS fueron de 24 y el tiempo medio para carga completa de 2, 3 semanas.
ConclusiónLa cirugía de conservación de miembro representa el tratamiento de elección en pacientes con tumores óseos y la reconstrucción con endoprótesis resulta una alternativa válida, con índices de fracaso similares a otras reconstrucciones.
The treatment of musculoskeletal tumours has undergone momentous change in recent decades. At the beginning of the nineteen seventies the mainstay of treatment for these types of tumours was amputation, with survival rates of less than 30%.1,2 With the advent of neoadjuvant chemotherapy and the advances in radiation therapy, survival rates improved significantly, rising to 60%–70% at 5 years.3,4 Limb salvage surgery is currently the treatment of choice for most of these patients. Many studies in the literature show that there are no differences in terms of survival between patients treated with limb salvage surgery and amputated patients.5–7 A great many reconstructive options for the treatment of bone defects after oncological resections have been described. These include biological or prosthetic reconstructions or a combination of both, such as alloprostheses.8–11
Reconstruction with structural allograft after tumour resection in the limbs makes it possible to preserve more bone stock and biomechanically restore the flexor-extensor and ligament system, with the limitations that weight-bearing of the limb must be restricted for a prolonged period of time, it requires an extensive rehabilitation period, and there is a risk of transplant failure given the need for adjuvant radiation treatment. By contrast, endoprostheses show greater benefits for people with tumours of poor prognosis or the elderly, and enables early ambulation and cessation of pain. Associated advantages and disadvantages have been described for both procedures, but there is controversy with regard to the best reconstructive option.12–14 Historically, our institution was renowned for its use of bone transplants as a reconstructive technique.15–17 However, since the beginning of 2000 there has been a major increase in the indication for endoprostheses in limb salvage surgery.18 The use of endoprostheses has evolved in recent decades, principally due to the improvements to these implants. Their advantages are availability, their flexibility in dealing with varying bone defects, they enable early weight bearing and mobilisation, and patients are able to rapidly resume their daily living activities. On the other hand, complications such as loosening, dislocation, decoupling of the implant's modules, and infection remain a concern for surgeons.19,20
The aim of our paper was to study a series of oncological patients treated with modular endoprostheses and assess:
Material and methodsA retrospective search on our longitudinal oncological database was performed between March 2001 and August 2015 of all patients who underwent reconstruction with modular endoprostheses. Skeletally mature patients were included in the study, with primary or secondary bone tumour disease, and with a minimum follow-up of 24 months for the patients who were alive at the time of the study. All patients operated for purely reconstructive purposes or treated in a different institution were excluded. The indications for the use of modular endoprostheses in oncological patients in our institution were: patients with a poor response to chemotherapy, with metastases (with expected survival of more than 6 months), undergoing adjuvant radiotherapy treatment, elderly patients, the anatomical region of the proximal femur, and with reconstructive surgery secondary to the failure of massive bone transplants. Modular prostheses with rotating hinges and cemented stems were used, manufactured by Zimmer Biomet Spain S.L.U. (Barcelona, Spain). The study population was divided into 3 groups: group 1, comprising patients with primary malignant or benign locally aggressive tumours; group 2, patients with bone metastases and group 3, patients reconstructed with a modular endoprosthesis due to failure of massive bone transplants.
The following variables were analysed:
- •
Survival of the implant according to the Kaplan–Meier method.
- •
Causes of limb salvage surgery failure according to the classification by Henderson et al. (2014). There are 5 types. From 1 to 3 are mechanical failures. Types 4 and 5 are non-mechanical failures. Type 1: soft tissue failure (1A: functional failure; 1B: coverage failure). Type 2: aseptic loosening (2A:
at 2 years). Type 3: structural failure (3A: implant rupture or wear; 3B: periprosthetic fracture). Type 4: infection that requires a change of prosthesis (4A: at 2 years). Type 5: recurrence or progression of the tumour in contact with the prosthesis (5A: soft tissues; 5B: bone). - •
Rate of reinvention due to complications.
- •
Limb salvage rate.
- •
Functional outcomes were assessed according to the MSTS score that gives a maximum score 30 points and a minimum of 0. Time to weight bearing was analysed from the first postoperative day to the time that the patient was able to walk bearing 100% of their weight.
- •
Survival was analysed using the Kaplan–Meier method. The student's t-test was used for the demographic analysis of the groups. The differences in the groups were compared using the log-rank test. STAVIEW software was used for the statistical analysis. A p<.05 was considered statistically significant.
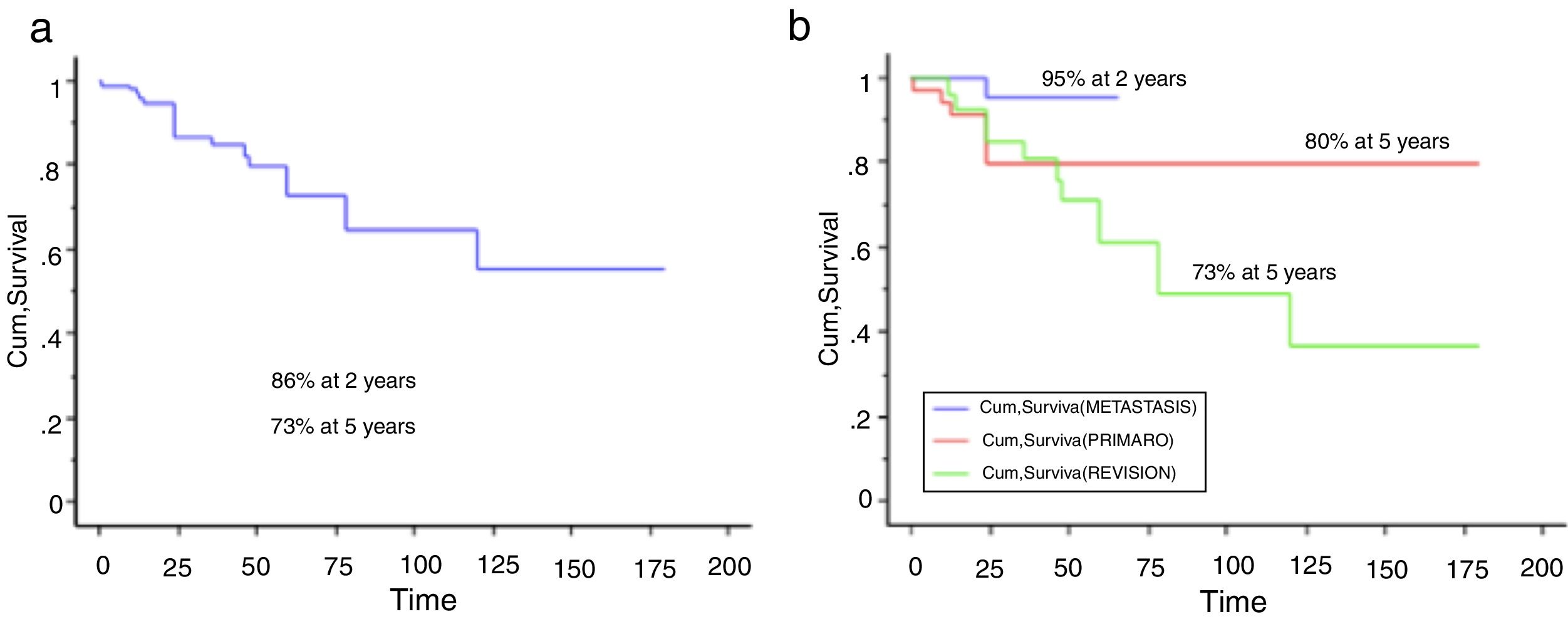
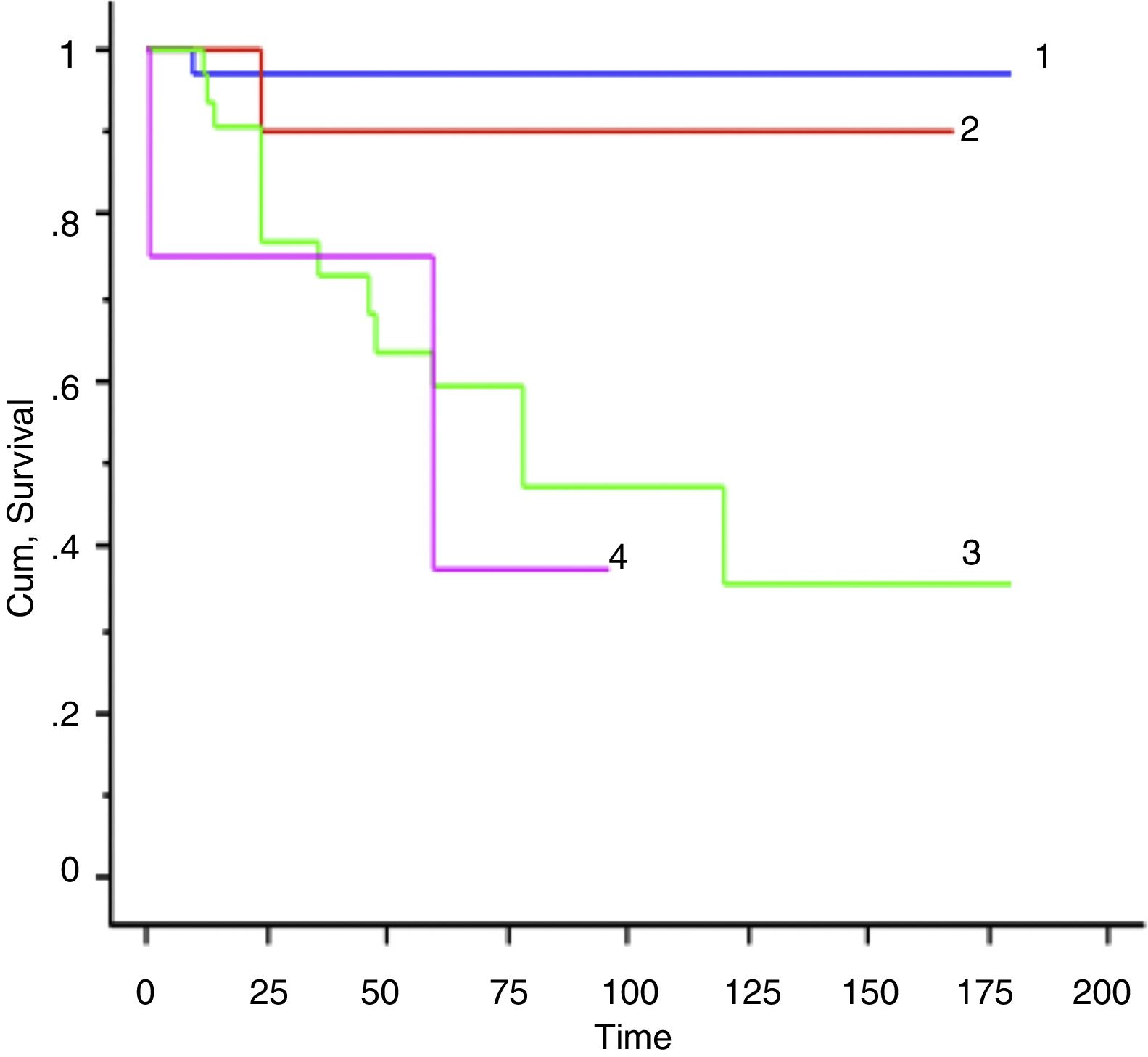
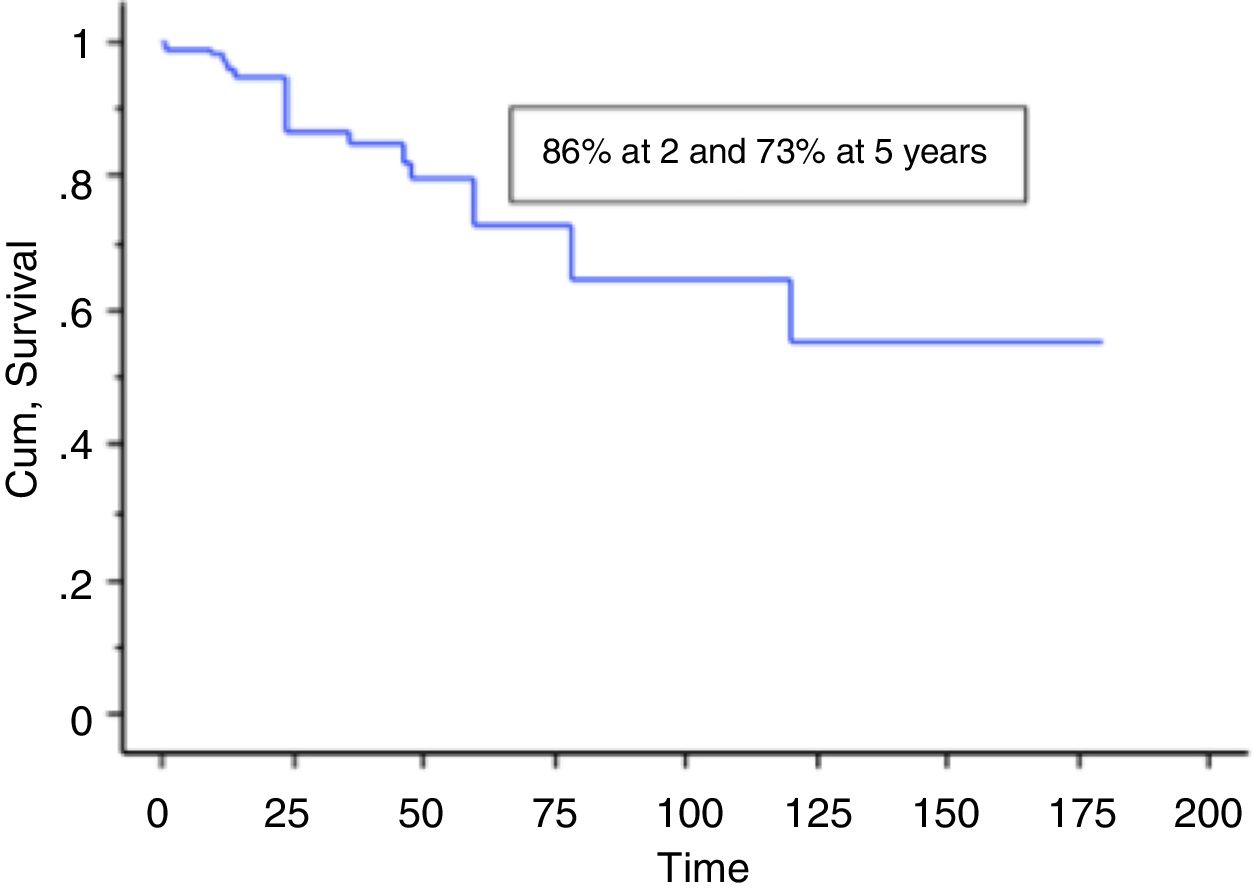
A total of 106 patients with bone tumours treated with modular endoprostheses were included in the study. The mean age of the series was 48.5 (95% CI range: 14–89), and the average patient follow-up was 68 months (95% CI range: 24–288). The overall survival of the implant in our series was 86.4% at 2 years (95% CI: 79–94), and 73% at 5 years (95% CU: 60–80) (Figs. 1–3). According to the anatomical site, survival of the reconstruction in the hip was 97% at 5 years (95% CI: 91–102), in the humerus it was 90% at 5 years (95% CI: 77–103), and 60% at 5 years in the knee (IC 95%: 40–78) (Fig. 4).
 Overall survival of the implant was 86.4% at 2 years (95% CI: 79–94), and 73% at 5 years (95% CI: 60–80). (b) Overall survival of the implant per group: primary: 80% at 2 and at 5 years (95% CI: 65–94.4); metastasis: 95% at 2 years; revisions: 73% at 5 years (95% CI: 60–80).")

 Hip: 97%; (2) humerus: 90%; (3) knee: 60%; (4) total arthroplasties: 45%.")
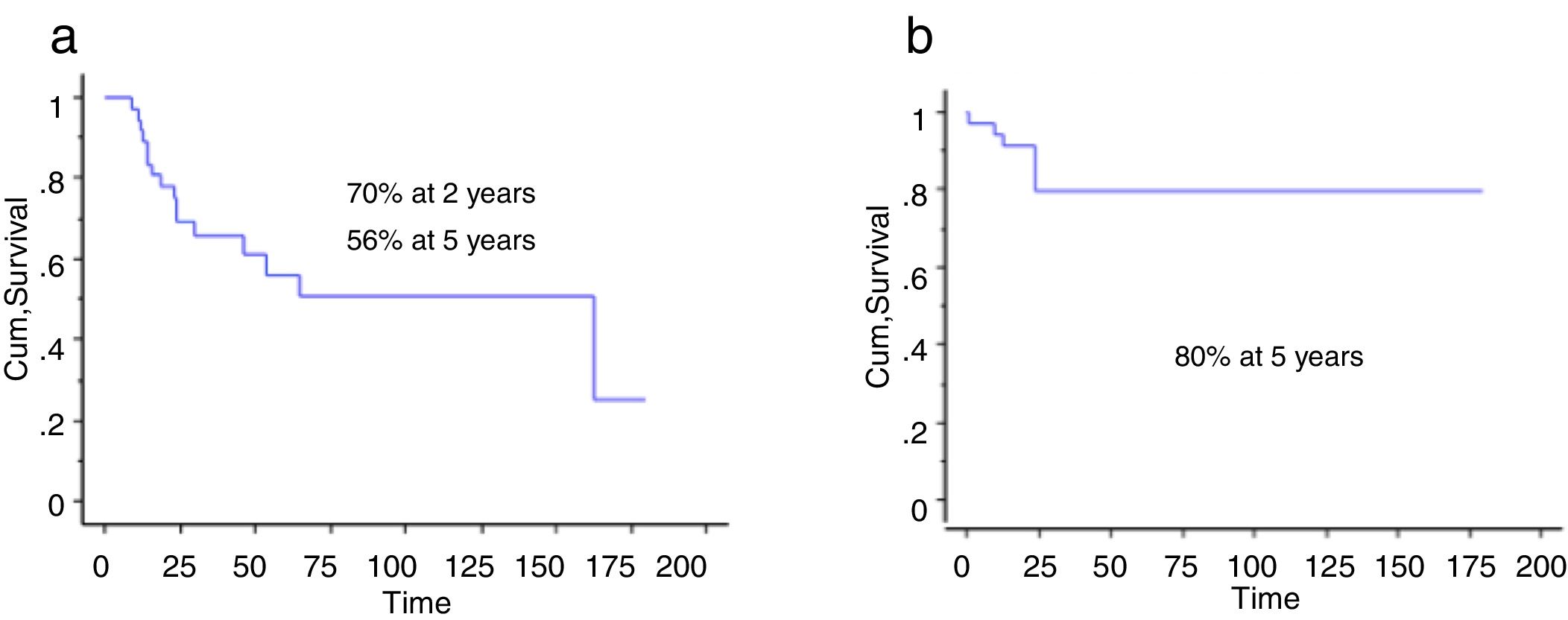
 Primary bone tumour survival at 2 years was 70% (95% CI: 54–84), and 56% at 5 years (95% CI: 71–70). (b) Overall primary implant survival: 80% at 2 and at 5 years (95% CI: 65–94.4).")
The size of the resection was not a prognostic factor for the prosthetic reconstruction failures (p: .2). Primary surgery vs revision surgery was not associated with a higher rate of implant failure (p: .21).
The limb salvage rate in the entire series was 96% at 5 years (95% CI: 91–99). The mean time until the patients were able to fully weight bear was 2.3 weeks (range 2–5).
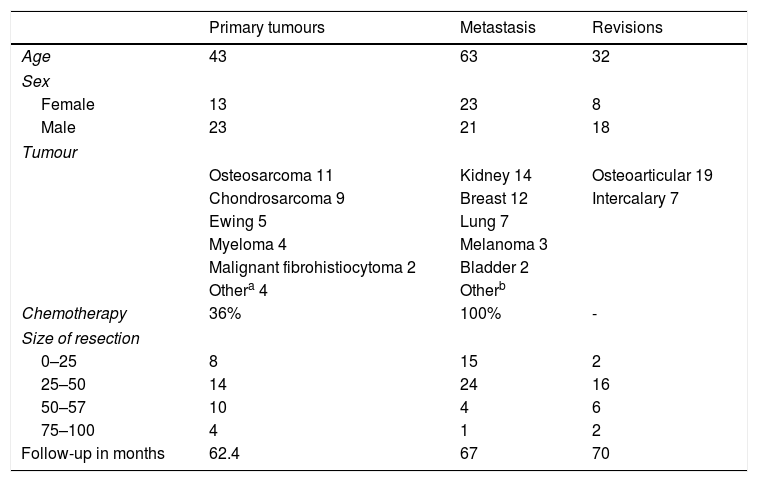
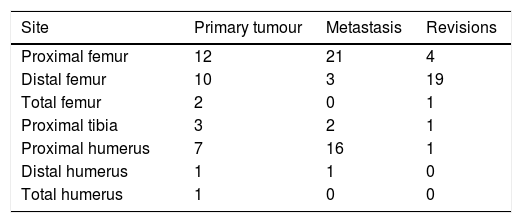
Group 1 primary bone tumours: 36 patients were included. The mean age of the series was 43 (range 14–81), and the average follow-up was 62.5 months (range 24–180 months). The demographic characteristics of the series are summarised in Table 1. The most common anatomical site was the proximal femur (33%), followed by the proximal humerus (19%), then the distal femur (8%), and the proximal tibia (8%) (Table 2).
Demographic outcomes.
| Primary tumours | Metastasis | Revisions | |
|---|---|---|---|
| Age | 43 | 63 | 32 |
| Sex | |||
| Female | 13 | 23 | 8 |
| Male | 23 | 21 | 18 |
| Tumour | |||
| Osteosarcoma 11 | Kidney 14 | Osteoarticular 19 | |
| Chondrosarcoma 9 | Breast 12 | Intercalary 7 | |
| Ewing 5 | Lung 7 | ||
| Myeloma 4 | Melanoma 3 | ||
| Malignant fibrohistiocytoma 2 | Bladder 2 | ||
| Othera 4 | Otherb | ||
| Chemotherapy | 36% | 100% | - |
| Size of resection | |||
| 0–25 | 8 | 15 | 2 |
| 25–50 | 14 | 24 | 16 |
| 50–57 | 10 | 4 | 6 |
| 75–100 | 4 | 1 | 2 |
| Follow-up in months | 62.4 | 67 | 70 |
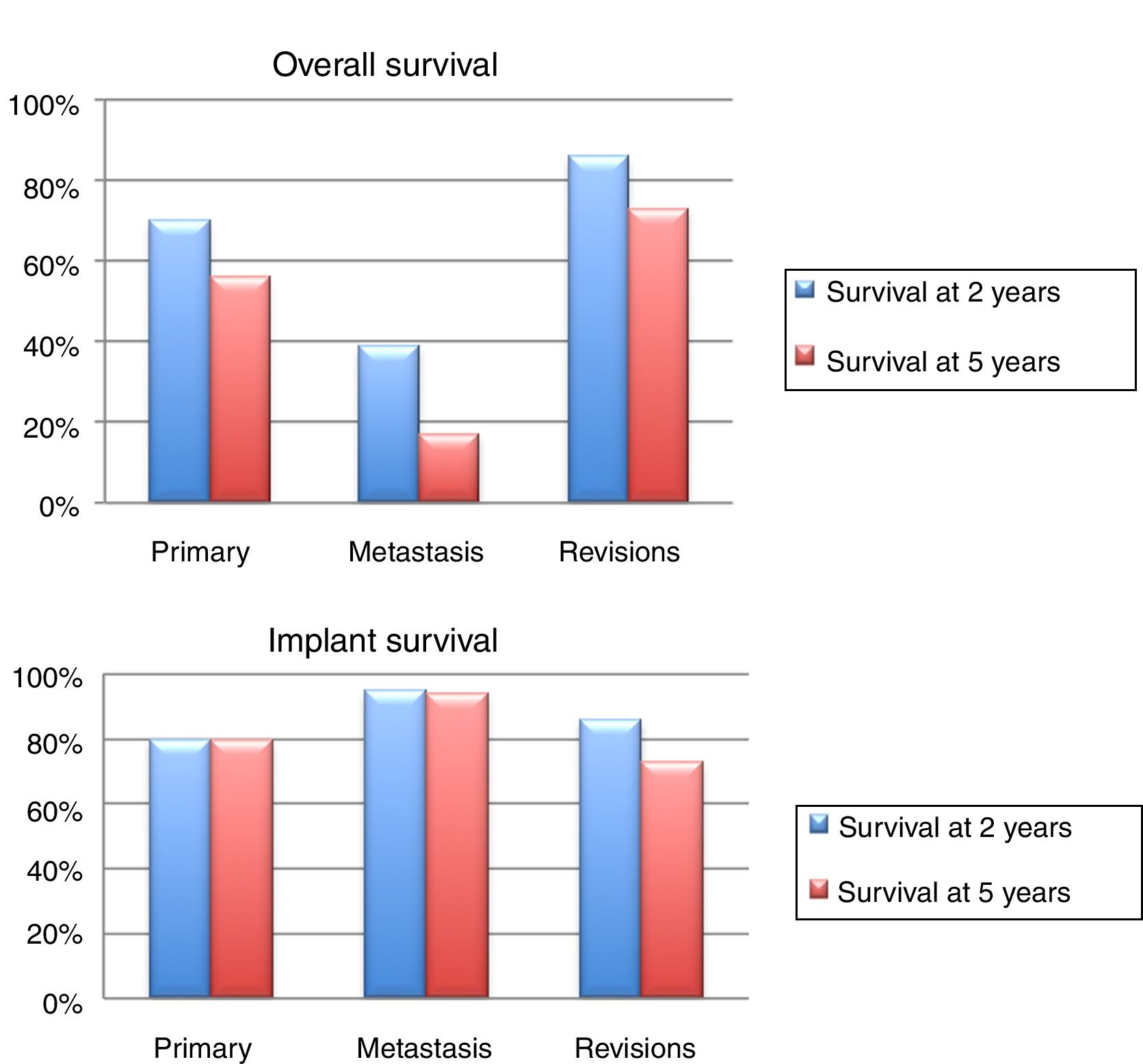
The patients’ overall survival at 2 years was 70% (95% CI: 54 –84), and 56% at 5 years (95% CI: 71–70). The survival at 2 and 5 years of the implant was 80% (95%CI: 65–94.4) (Fig. 5). Adjuvant chemotherapy was a risk factor for failure of the reconstruction (p<.01); not the size of the resection (p: .2) or the presence of a pathological fracture (p: .67).
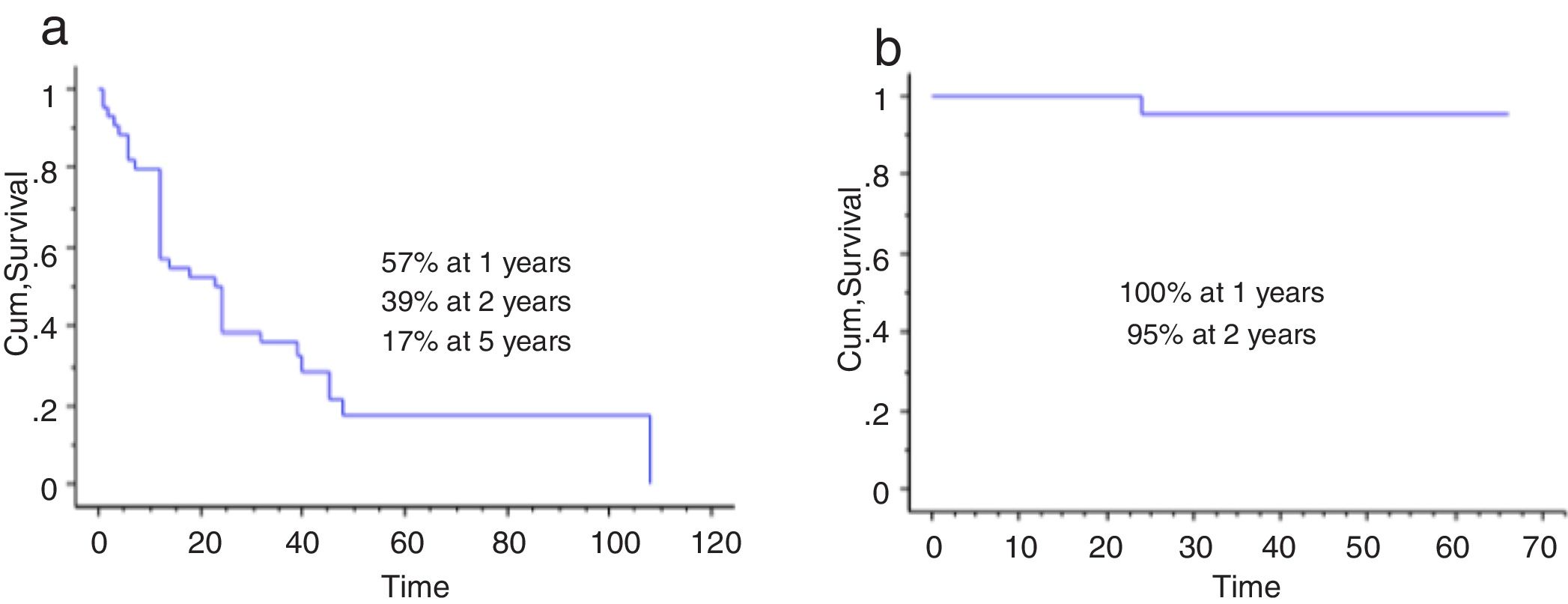
 The overall survival rate of the patients with metastatic bone tumours was 57% at year one, 39% at 2 years and 17% at 5 years. (b) Implant survival in this group was 100% at 12 months and 95% at 24 months.")
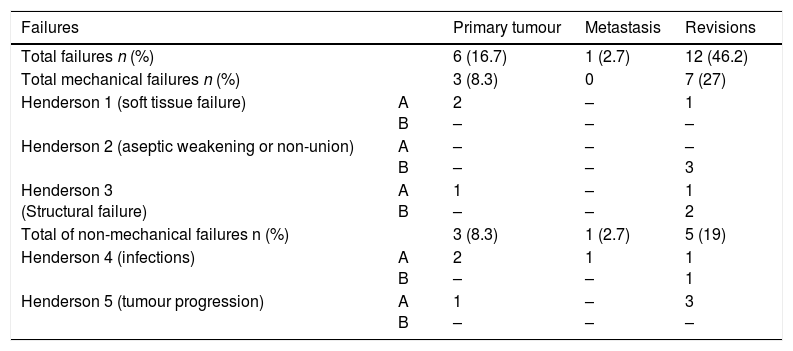
Three failures were classified as mechanical (2 type 1A, one type 3A), and 3 as non-mechanical (2 type 4A, one type 5A). The mean time until failure was 16 months (range: 1–24). Seventeen of the 36 patients (47.2%) had to be treated with at least one further surgical procedure due to a complication (total 22 procedures). The causes were: local recurrence (9), infection (5), and dislocations (5). The limb salvage rate was 94.4% (95%CI: 91–99). The functional assessment according to the MSTS was 26 points (range: 20–29).
Group 2 bone metastases: 44 patients were included in this group. The average age was 63 (range 34–89). The mean follow-up was 67 months (range 24–170). The demographic characteristics are summarised in Table 1. The most common anatomical site was the proximal femur (21/44 patients; 48%), then the proximal humerus (16/44 patients; 36%), followed by the distal femur (3/44 patients; 9%) (Table 2).
The patients’ overall survival was 57% at one year (95% CI: 42 and 51), 39% at 2 years (95% CI: 24 and 73), and 17% at 5 years (95% CI: 24–30). The survival of the implant in this group was 100% at 12 months, and 95% at 24 months (95% CI: 87–100) (Fig. 6). The only patient who failed was due to an acute infection (Henderson 4A). Six of the 44 patients (14%) had to be treated by at least one further procedure due to a complication (total of 7 procedures). The causes were: dislocation (n=4) and infection (n=3). The limb salvage rate in this group was 100%. The functional assessment according to the MSTS score was 24/30 (range: 19–29).
, and 73% at 5 years (95% CI: 60–80).")
Group 3 revision of massive bone transplants. Twenty-six patients were included in this group, with an average age of 32.5 years (range: 14–76), and a mean follow-up of 70 months (range: 12–180). The primary reconstructions were 7 intercalary transplantations, and 19 osteoarticular transplants.
The survival of the implant was 86% at 2 years (95% CI: 79–94), and 73% at 5 years (95% CI: 60–83). Twelve reconstructions failed; mechanical cause was the most prevalent (n=7) and, of these, aseptic loosening (Henderson type 2A) was the most frequent (n=3). The other failures are detailed in Table 3. Fourteen of the 26 patients (58%) had to be treated with at least one further surgical procedure, due to a complication, with a total of 27 procedures. The causes were: infection (n=8), implant rupture (n=3), tumour recurrence (n=4), loosening (n=3), and dislocation (n=3).
Type of prosthetic failure according to Henderson et al.
| Failures | Primary tumour | Metastasis | Revisions | |
|---|---|---|---|---|
| Total failures n (%) | 6 (16.7) | 1 (2.7) | 12 (46.2) | |
| Total mechanical failures n (%) | 3 (8.3) | 0 | 7 (27) | |
| Henderson 1 (soft tissue failure) | A B | 2 – | – – | 1 – |
| Henderson 2 (aseptic weakening or non-union) | A B | – – | – – | – 3 |
| Henderson 3 (Structural failure) | A B | 1 – | – – | 1 2 |
| Total of non-mechanical failures n (%) | 3 (8.3) | 1 (2.7) | 5 (19) | |
| Henderson 4 (infections) | A B | 2 – | 1 – | 1 1 |
| Henderson 5 (tumour progression) | A B | 1 – | – – | 3 – |
Source: Henderson et al. (2014).21
According to the MSTS assessment, the mean functional outcome was 24 points (range: 17–28).
DiscussionLimb salvage surgery is the treatment of choice for patients with malignant and locally aggressive bone tumours. Although many reconstructive techniques have been described, there is no evidence in the literature that one technique is superior to the others. Albergo et al. compared 133 patients with proximal tibia reconstructions with massive bone transplants and endoprostheses, and found no differences in the failure rates at 5 and at 10 years.23 In recent decades, the use of endoprostheses to reconstruct large segmentary bone defects has gained acceptance among orthopaedic surgeons. This is due to advances in adjuvant therapies for the treatment of oncological patients, to the improved prosthetic designs and their availability, to advances in surgical techniques, and increased surgeon experience. Myers et al. studied the long-term follow-up of distal femoral endoprostheses, where the risk of revision surgery due to aseptic loosening of the hinged prostheses was 35%, was 24% with constrained prostheses with hydroxyapatite, and 0% for those with hydroxyapatite collar.24
The survival rates of endoprostheses vary according to their location, from 54% in the proximal tibia to 90% in the proximal femur.25,26 Zeegen et al. studied 141 patients with endoprostheses, and reported an overall survival rate of the implant of 88% at 3 years, and 76% at 5 years, with a survival rate at 3 years in the hip and shoulder of 100%, 87% in the knee, and 53% for total femur implants.27 The overall survival of the implant in our series was 86% at 2 years, and 73% at 5 years. According to anatomical site, in the hip it was 97% at 5 years, in the humerus it was 90%, and 60% in the knee. We believe that these findings are in line with the corresponding survival rates in the studies published in the literature. In terms of the survival of the implant in each particular group, we found that the patients with metastases had better rates compared to the other 2 groups (100% at one year and 95% at 2 years). However we must stress that this finding relates to the low overall survival of these patients, which was 17% at 5 years.28 According to the classification by Henderson et al., 19 implant failures were described in our series, and the most prevalent were mechanical. The most frequent sites of failure were the distal femur, and the proximal tibia. Of the mechanical failures, those of soft tissues, type 1 in the classification, presented in the hip and shoulder principally, which reflects the intrinsic instability of these joints.19 Unwin et al. described the results of 1001 endoprostheses with aseptic weakening as the final outcome, and reported that the prosthesis failed most frequently in the distal femur, with a 9.9% revision rate.29
Forty seven percent of the patients with primary tumours, 58% of patients who had undergone revision surgery due to failed massive bone transplants, and 13% of the patients with metastases had to be reoperated due to a complication. Infection was the main reason for reintervention in all of the 3 groups. However, in our series less than 8% of the endoprosthesis failures were caused by infection. Jeys et al. reported a periprosthetic infection rate of 11% in a series of 1264 oncological patients treated with endoprostheses over a period of 37 years.30
Although it was expected that revision surgery secondary to a failed massive bone transplant would have a higher rate of complications than primary surgery, the implant failure rate between these 2 groups was not statistically significant (p: .21), which was also reported by Zeegen et al.27
Grimer et al., in their paper on very long term follow-up of endoprosthetic replacement for malignant bone tumours, reported an average of 2.7 reinterventions per patients. However, the risk of amputation at 30 years was 16%, and most of the patients preserved their limb.31 In our series, the rates of limb preservation were 96% at 5 years.
Our paper has some limitations: its short-term follow-up, retrospective design and the heterogeneity of the sample.
ConclusionLimb salvage surgery is the treatment of choice for patients with bone tumours and reconstruction with endoprostheis is a valid alternative, with similar failure rates to other forms of reconstruction.
Level of evidenceLevel of evidence III.
Conflict of interestsThe authors have no conflict of interest to declare.
Please cite this article as: Cabas-Geat AE, Bruchmann MG, Albergo JI, Ayerza MA, Farfalli G, Aponte-Tinao LA, et al. Reconstrucción con prótesis modulares posterior a una resección oncológica. Evaluación de los fracasos y análisis de la supervivencia. Rev Esp Cir Ortop Traumatol. 2019;63:173–l80.
