






Sporotrichosis is a fungal disease caused by the Sporothrix schenckii species complex. It is usually acquired by trauma with plants. Lymphatic-cutaneous is the most common clinical manifestation.
Case reportThe present case describes the development of an epidermoid carcinoma as a late complication on a long evolution sporotrichosis scar. During a period of 50 years, the patient had lesions in the right hand. Sporotrichosis was diagnosed and treated with potassium iodide. Eleven years after the healing of the lesions, a squamous cell carcinoma on the scar of this mycosis was diagnosed.
ConclusionsThe chronic sporotrichosis injury was probably the cause of the tumor developed on the scar.
La esporotricosis es una enfermedad causada por el complejo de especies Sporothrix schenckii. Generalmente se adquiere por traumatismos con plantas. El compromiso linfocutáneo es la manifestación clínica más común.
Caso clínicoEl presente caso describe la aparición de un carcinoma epidermoide como complicación tardía en la cicatriz de una esporotricosis de larga evolución. Durante 50 años el paciente presentó lesiones en la mano derecha, se diagnosticó esporotricosis y se trató de manera tópica con yoduro de potasio. Once años después de la cicatrización de la esporotricosis, se diagnosticó un carcinoma de células escamosas en la cicatriz de esta micosis.
ConclusionesEl daño en el tejido producido por la esporotricosis crónica podría ser la causa que desencadenó el proceso tumoral sobre la cicatriz.
Sporotrichosis is a fungal disease produced by the Sporothrix schenckii species complex, which includes species such as Sporothrix brasiliensis, S. schenckii sensu stricto, Sporothrix globosa, Sporothrix luriei, Sporothrix mexicana, and Sporothrix pallida.1 This disease appears in a chronic or subacute form and is characterized by the presence of ulcerative nodular lesions along the lymph nodes.3,9 Despite being reported throughout the world, infections caused by the S. schenckii complex are epidemic in tropical and temperate regions.9 Outbreaks are related to farm or garden work,4 while zoonotic transmission has also been described.2
Several pathogenic and resistance mechanisms have been investigated in the S. schenckii complex, such as the presence of proteases, adhesins, cell wall and antioxidant enzymes.11 Chronic interaction with fungi may produce in the host different responses.5
Considering that cancer is a multifactorial disease, long interaction between the pathogen and the host may lead to cell changes. The role of different pathogens in cancer development has been investigated, as, for example, oncogenes activated by viruses.8 However, there are few reports in the scientific literature concerning the development of cancer as a consequence of an sporotrichosis. In this context, the present study describes the development of a squamous cell carcinoma on the scar of a healed lesion from a chronic sporotrichosis.
In 2003, a 73 year-old male patient, retired and residing in Palmeira das Missões (Brazil), sought medical attention. He presented suppurative vegetating lesions on his right arm, as shown in Fig. 1a-c. The patient related that he had kept these lesions hidden by using a t-shirt for about 50 years. The patient had also a vegetative lesion on the left foot, which had appeared three months before the medical assessment (Fig. 1d). The anatomopathologic exam showed suppurative chronic inflammation, epithelial hyperplasia, edema and granulation tissue.
, forearm (b), elbow (c) and left foot (d).")
The result of the mycological exam of the sample collected from the right arm was positive for S. schenckii complex. The patient was treated with potassium iodide and, within 5 weeks, 90% regression in the right arm lesions and 60% regression in the left foot lesions were observed. Following this therapeutic intervention, the patient was considered completely cured after 9 weeks.
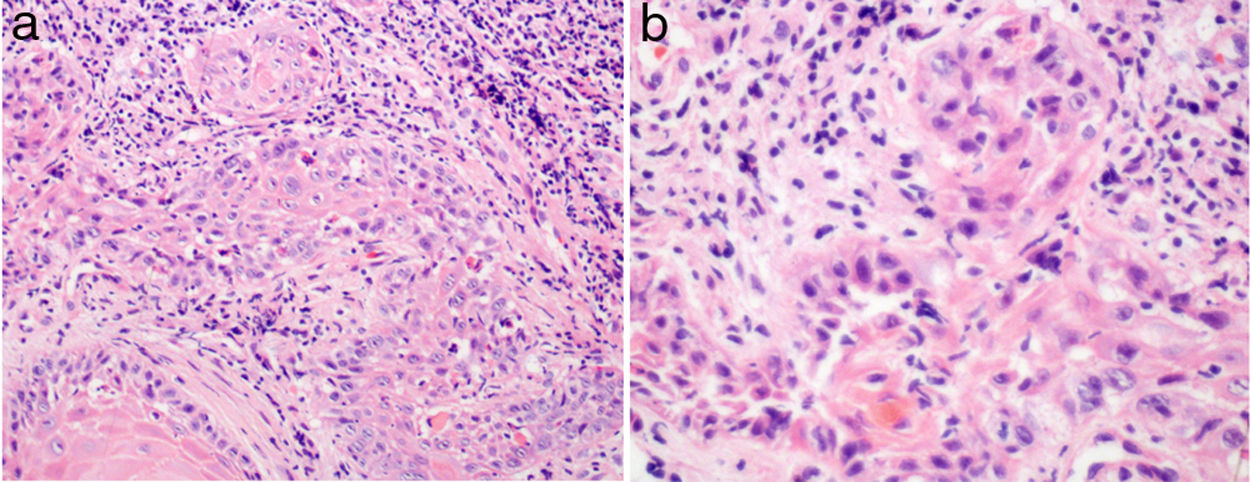
In 2014, eleven years after the diagnosis and cure of the sporotrichosis, the patient ask for medical attention due to the presence of hyperkeratotic lesions on the right hand and scars on the lesions treated previously (Fig. 2). Samples were sent for mycological and histopathologic exams. The anatomopathologic analysis showed well-differentiated squamous cell carcinoma (Fig. 3), while the mycological exam was negative. The patient was submitted to surgical procedure, and treated with cryotherapy. The case evolved to total recovery in about 4 months after the treatment.

 and 400× (b).")
The spontaneous resolution of S. schenckii infections occurs rarely and, therefore, most cases require treatment.6 Potassium iodide solution is the first choice therapy in small lesions due to its effectiveness and low cost.10 In extensive lesions the therapeutic alternative is the use of itraconazole, alone or associated with potassium iodide solution, thermotherapy or cryotherapy.4 The immune response and the pathogenicity of the infective strain may determine the invading degree in S. schenckii complex infections.5,11 In the present case it is possible that the foot lesion was produced by autoinoculation, taking into account the long time the lesion in the hand was present. The distant autoinoculation is well documented in S. schenckii complex.7
Considering that both the hands of the patient showed a similar photodamage degree, it can be inferred that not the exposure to ultraviolet radiation but the chronic sporotrichosis injury was the cause of the tumor developed on the scar.

