


Radical prostatectomy may have a significant impact on quality of life (QoL) because of erectile dysfunction, depression and incontinence. In this study, the mood and QoL of patients who underwent radical prostatectomy due to localized prostate Ca and were non-relapsed at least 12 months after operation were evaluated.
Materials and methodsWe evaluated 35 patients who underwent radical prostatectomy operation between 2000 and 2011 and showed no reduction during 12 months observation. IIEF, Beck Depression test, and EORTC 3.0 quality of life were given and scored. In this study, the effects of erectile dysfunction according to Beck depression test and QoL scores and correlation between the mood and QoL are evaluated.
ResultsIn our study, ED groups categorized as mild, moderate and severe had no correlation with Beck depression scores (p=0.874). But only the patients with severe and moderate erectile dysfunction had moderate and severe depression scores. Negative correlation was determined (p=0.013) when Beck Depression scores with IIEF scores without categorizing ED groups. Correspondingly, negative correlation was determined (p=0.048) between QoL and IIEF scores, whereas positive correlation was determined (r=0.756 and p<0.001) between QoL and Beck Depression scores.
ConclusionsWe observed that an increase of erectile dysfunction elevated depression symptoms and resulted in bad quality of life. During tumor control, it is important to use methods that do not affect QoL.
La prostatectomía radical podría impactar de manera significativa en la calidad de vida (QoL) debido a la disfunción eréctil, la depresión y la incontinencia. En este ensayo se analiza el estado anímico y la QoL de los pacientes que se sometieron a prostatectomía radical debido a un cáncer de próstata localizado y no recidivante al menos 12 meses después de la intervención.
Material y métodoSe evaluaron 35 pacientes que se sometieron a prostatectomía radical entre los años 2000 y 2011 y no mostraron ninguna reducción durante los 12 meses de control. Se entregaron y analizaron los resultados en los test IIEF, Inventario de Depresión de Beck y EORTC 3.0 de calidad de vida. En este estudio se examinan los efectos de la disfunción eréctil conforme al Inventario de Depresión de Beck y la puntuación de QoL, así como la correlación entre el estado anímico y la calidad de vida.
ResultadosEn nuestro estudio, los grupos clasificados con disfunción eréctil leve, moderada o grave no guardaron correlación con las puntuaciones de depresión de Beck (p=0,874). Únicamente los pacientes con una disfunción eréctil grave o moderada arrojaron resultados de depresión moderada o grave. Se estableció una correlación negativa (p=0,013) de los datos de Depresión de Beck con los del IIEF sin clasificar los grupos con disfunción eréctil. Asimismo, se ratifica una correlación negativa (p=0,048) entre el IIEF y la QoL, si bien sí existe una correlación (r=0,756 y p<0,001) entre los datos de la QoL y el Inventario de Depresión de Beck.
ConclusionesObservamos que un aumento en la disfunción eréctil eleva los síntomas de depresión y acarrea una peor calidad de vida. Es importante utilizar métodos que no afecten la calidad de vida para el control de los tumores.
Prostatecancer (PCa) is the most common diagnosed cancer in the Western world, and, secondly, the most common cause of cancer-related deaths.1 After the diagnosis of prostate cancer,2 treatment options and related complications affect the patient's quality of life (QoL). Radical prostatectomy (RP) surgery for treatment of PCa declines the patient's quality of life (QoL) due to complications such as depression, disturbances in bowel function, incontinence and sexual dysfunction (SD).3 However, 45% of patients state that quality of life after RP is as important as cancer control.4
SD corrupts self-confidence, mood and the quality of life in inter-family relationships. Sexual satisfaction is an important indicator of life satisfaction.5 Considering that long term complications of prostate cancer treatments are erectile dysfunction (ED) and incontinence, these issues are important in QoL.6 Furthermore, 20% of patients prefer to be potent to cancer cure.7
In this study, emotional states, erectile functions QoL scores and their relations of the nonrelapsed patients who underwent RP were assessed.
Materials and methodsPatients, who underwent RP between 2000 and 2011 and were non-recrudescent for at least one year follow-up were included in the study between May 2012 and July 2012. Patients without ED and depression treatment prior to surgery were included in this study. After local ethics committee approval dated 07.02.2013 with 2012-135D1 project number, the names of the patients were found by scanning files and they were invited to our clinic for our survey. Purpose of the study was explained and volunteer patients were included in the study upon their written consent.
Beck Depression Inventory (BDI), IIEF (International Index of erectile function) and the EORTC QLQ-C30 version 3.0 Scale quality of life questionnaires were given to the patients by a researcher. Overall quality of life questionnaire consists of 30 questions and three sections including global health status, quality of life symptom section and functional section. Functional charts include physical, role, cognitive, emotional and social functions. Nausea, vomiting, fatigue, pain and social functions are evaluated in symptom charts. In addition, dyspnea, insomnia, loss of appetite, constipation, diarrhea and financial difficulties are measured by one question. The 30 items on the scale are scored as 1-none, 2-less, 3-mean, 4-too many. In questions 29 and 30 patients were asked to assess their health and quality of life from one to seven as 1-too bad and 7-excellent. 29th and 30th questions revealed patient's well-being. Lower scores in functional and symptom sections indicate high QoL whereas higher scores indicate low QoL. In terms of these definitions, the total score of the QoL, functional score and symptom score were calculated. According to the IIEF scores, 26–30 are considered as normal, 17–25 as mild, 11–16 as moderate, and 6–10 as severe ED.
SPSS (Statistical package for social sciences) for Windows 16.0 software (SPSS Inc. Chicago, Illinois, USA) was used for statistical analysis. Descriptive statistical methods (frequency counts, mean, standard deviation) were used in evaluation of data. Chi-square test was used for comparison of classified data between the groups. In the analysis of continuous variables, Spearman's correlation analysis and Kruskal–Wallis tests were used. Statistical significance was accepted as p-value<0.05.
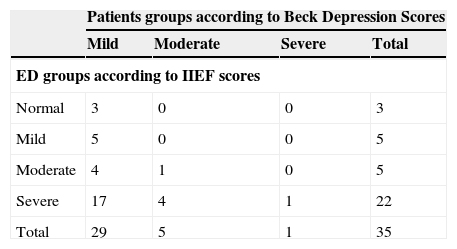
ResultsThe mean age of the 35 patients enrolled in the study was 66.66+7.17. Severe erectile dysfunction was detected in 22 (62.9%) patients, moderate erectile dysfunction in 5 (14.3%) patients, and mild erectile dysfunction in 5 (14.3%) of 35 patients was determined. Only 3 patients (8.6%) did not have erectile dysfunction. Only 1 (2.9%) of the patients had severe depression scores, while 5 (14.3%) had moderate and 29 (82.9%) patients had mild depression scores in terms of Beck Depressşion scores. No correlation between the ED group and the Beck Depression scores were observed (chi-square test, p=0.874, Spearman's correlation analysis, p=0.195). However only moderate and severe depression scores were found in patients with the severe and moderate erectile dysfunction (Table 1).
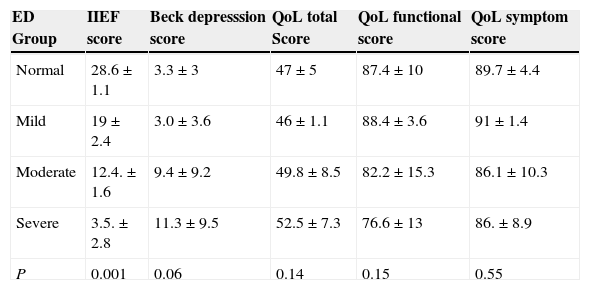
Negative correlation was examined between the Beck depression and IIEF scores without separating into ED groups (r=−0.417, p=0.013). Correspondingly, negative correlation was detected between the QoL score and the IIEF total score (r=−0.335, p=0.048), and positive correlation was detected between QoL total score and the Beck Depression scores (r=0.756 and p<0.001). Beck depression scores, QoL total score, QoL functional score and QoL symptom scores when ED's were grouped are shown in the table below.These groups differentiated from each other according to Kruskal–Wallis test (Table 2).
Beck Depression score, QoL total score, QoL functional score and QoL symptom score according to ED groups.
| ED Group | IIEF score | Beck depresssion score | QoL total Score | QoL functional score | QoL symptom score |
|---|---|---|---|---|---|
| Normal | 28.6±1.1 | 3.3±3 | 47±5 | 87.4±10 | 89.7±4.4 |
| Mild | 19±2.4 | 3.0±3.6 | 46±1.1 | 88.4±3.6 | 91±1.4 |
| Moderate | 12.4.±1.6 | 9.4±9.2 | 49.8±8.5 | 82.2±15.3 | 86.1±10.3 |
| Severe | 3.5.±2.8 | 11.3±9.5 | 52.5±7.3 | 76.6±13 | 86.±8.9 |
| P | 0.001 | 0.06 | 0.14 | 0.15 | 0.55 |
Sub-group analysis in terms of QoL scores showed positive significant correlation between QoL functional scores that were calculated by the formula with the IIEF score (r=0.338 and p=0.047). The correlation between QoL symptom score and IIEF score was not significant (r=0.243 and p=0.160). Correlation between QoL functional scores and the Beck depression scores were negatively significant (r=−0.708, p<0.001). Also positive significant correlation was observed between the Beck Depression Inventory score and the detected QOL symptom scores detected (r=0.788, p<0.001).
There was no correlation between IIEF scores and questions 29 and 30 of QoL questionnaire form that evaluates global health status (r=0.187 and p=0.282), however, positive significant correlation was observed between the Beck depression scores (r=0.375 and p=0.026). There was no difference between ED groups for global health score (Kruskal–Wallis test, p=0.302). Moreover the groups were different from each other with chi-square test (p=0.874) and there was no significant correlation between them according to Spearman's correlation analysis (p=0.195).
DiscussionProstate cancer is detected at an early stage than before because of the wide spread use of PSA, thereby increasing the duration of life after diagnosis and the majority of patients die from causes other than cancer.8 Patients’ QoL, who were diagnosed with prostate cancer and died for other reasons, is more affected by treatment when compared to undiagnosed prostate cancer patients who have lost their lives for other reasons.Quality of life measurements are beneficial to increase the quality of health system and problems encountered during practical applications. It helps to determine priorities and the most important problem by enabling communication with health workers and patient and their relatives.9
In addition, detecting patient's problem and ensuring communication, helps to make the treatment options the most appropriate for the patients. Disease course that is assessed by several objective methods can also be evaluated by the patient's, by self-examination.
Many researchers studied QoL after radical prostatectomy, radiation therapy and brachytherapy in patients with localized prostate cancer.10 In most of these studies, QoL during the year following treatment has been observed at the basal level.11 Therefore, we considered it would be appropriate to conduct inspections at the end of a year's time.
Bacon et al. investigated the effect of treatments on QoL in localized prostate cancer patients and they showed that most affected functions are sexual and urinary functions (ED and incontinence).6 It was observed that these problems also have adverse effects to QoL. In our study, patients with decreasing erectile function scores had higher depression scores.
Penson et al. states in his study that ED is the most important independent factor that demolishes QoL, two years after the main prostate cancer treatment.12 According to Nelson et al. theory ED patients with prostate cancer can cope more easily with the ED because they give the same importance to ED treatment as cancer treatment. The study investigated the relationship between ED and depression in prostate cancer patients and ED's relationship with severe depression has been shown. Interestingly ED patients with prostate cancer can cope better with ED than the patients with ED alone.13
Today, the relationship between ED and depressive symptoms are defined significantly. In our study, although there was no correlation between ED severity and the Beck depression scores, in non-separated groups of ED severity, IIEF score and the Beck Depression scores were found to have negative correlation. When ED scores were divided into groups there was no significant relationship between BECK depression scores and ED groups with chi-square test and Spearman's correlation analysis. However, only in patients with moderate and severe depression scores have moderate and severe ED scores. In undivided groups negative correlation was found between IIEF scores and Beck scores. As ED score decreases BECK score increases. There was a negative correlation between QoL scores and IIEF scores. As QoL scores increases, IIEF score decreases. A significant positive correlation was found between QoL score and BECK depression score. While QoL scores increases, BECK depression scores also increases. As global health status in QoL form is assessed, it is observed that global health status is not affected by ED but depression effects the global health status.
Today, more and more patients can be screened and diagnosed by means of cancer diagnostic tests and aggressive treatment applied to augment the QoL. The result is perceived as augmented QoL along with long-living people. This situation leads us to a controversy: treatment of cancer or QoL. Treatments that do not impair QoL and active follow-up treatment options may replace unnecessary aggressive treatments. Today, minimal invasive treatment approaches and methods emerged, claiming less morbidity while controlling cancer check-up. The most important argument is that laparoscopic and robot-assisted laparoscopic prostatectomy is to be minimally aggressive and claimed to have little effect on incontinence and erectile function than open surgery.14
In our study, reliable forms of queries and the reliability of the statistical analysis reinforce our study. Vulnerable point of the study is small number of reference groups.
ConclusionsDespite the small number of patients, in this study, it is observed that as the erectile dysfunction increases, depressive symptoms and QoL are impaired. At the same time we determined that QoL is deteriorated with increase in depressive symptoms.
Considering that minimal invasive treatment approaches preserve erectile function and continence maintains and augments QoL, contributions and support to these studies would lead us to see cancer survivors and happy people.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.