


To compare the effect of phosphodiesterase inhibitors and physical exercise alone in patients with erectile dysfunction (ED).
Materials and methodsA total of 60 patients with a satisfactory cardiopulmonary performance who consulted the outpatient clinics of Urology and Physical Therapy and Rehabilitation were included in the prospective study. In the study, 30 patients were scheduled for 6 weeks of vigorous aerobic exercise program to be carried out for 75min a day, 3 days a week. The remaining 30 patients received only an oral form of a phosphodiesterase inhibitor. All patients completed International Index of Erectile Function (IIEF) and quality of life (SF-36) forms before and after the treatment.
ResultsMedian age of the patients was 55.63±12.93 years with body mass index ranging between 18.99 and 35.86kg/m2. A statistically significant increase has been observed for IIEF-5 and SF-36 scores both in the physical exercise and medical treatment groups. However, in the medical treatment group post-treatment variation in IIEF-5 and SF-36 mental scores in the medical treatment group were statistically significantly higher when compared with the physical exercise group. Increase in physical SF-36 scores in the physical exercise group was more prominent without any statistically significant difference between groups.
ConclusionEmerging evidence indicates that exercise has a positive effect for improving many factors in men with erectile dysfunction including changes in body composition, physical function, risk of comorbid conditions, depression, quality of life and an increase in pelvic oxygenation and penile blood flow, and thus before or during the treatment with a phosphodiesterase inhibitor, regular physical activity should be recommend for all ED patients.
Comparar el efecto de inhibidores para la fosfodiesterasa y el ejercicio físico de manera independiente en pacientes con disfunción eréctil (DE).
Materiales y MétodoSe incluyeron un total de 60 pacientes en el estudio prospectivo. Estos pacientes habían acudido a las consultas externas de clínicas de Urología y Terapia física y Rehabilitación, no tenían diagnosticados trastornos neurológicos o psiquiátricos y presentaban función cardiopulmonar satisfactoria. En el estudio, 30 de los pacientes fueron sometidos a un programa de seis semanas consistente en la realización de actividad aeróbica vigorosa durante 75 minutos, tres veces por semana. Los 30 pacientes restantes recibieron una toma oral del inhibidor para la fosfodiesterasa. Todos los pacientes cumplimentaron los formularios del Índice internacional de la función eréctil (IIEF) y de calidad de vida (SF-36) antes y después del tratamiento.
ResultadosLa mediana para la edad de los pacientes fue de 55,63±12,93 años, con un índice de masa corporal incluido en el rango 18,99–35,86kg/m2. Se pudo observar un incremento significativo en los puntajes de los formularios IIEF-5 y SF-36, tanto en el grupo que recibió terapia física como el que recibió tratamiento médico. Sin embargo, en el grupo con tratamiento médico, la variación post-tratamiento en los puntajes obtenidos en el IIEF-5 y en los resultados mentales del SF-36 fue más alta que en el grupo que recibió terapia física. El aumento en el puntaje del SF-36 en el grupo de actividad física mostró una tendencia al alza, sin que las diferencias fueran significativas entre los grupos.
ConclusionesNuevas evidencias indican que el ejercicio físico tiene un efecto positivo para la mejora de varios factores en hombres con disfunción eréctil, incluyendo la composición corporal, la función física, el riesgo de comorbilidad, la depresión, la calidad de vida y el aumento de la oxigenación pélvica, además del flujo sanguíneo en el pene. Por tanto, de forma previa o conjunta a la indicación de inhibidores de la fosfodiesterasa, la actividad física regular debe ser recomendada a todos los pacientes con DE.
Erectile dysfunction (ED) is defined as the inability to achieve and maintain penile erection sufficient to permit a satisfactory sexual intercourse for at least 6 months.1 Penile erection is achieved through integrated and simultaneous functioning of neural, hormonal and vascular mechanisms. For the realization of penile erection, nitric oxide (NO) released from nerve endings via parasympathetic activation enters into cavernous smooth muscle cells and activates guanylate cyclase or adenylate cyclase enzymes which trigger increased production of cyclic guanylate monophosphate (cGMP) and cyclic adenylate monophosphate. With this mechanism, phosphorylation of potassium and calcium channels takes place with a resultant decrease in intracellular calcium content. As a consequence, penile smooth muscle relaxes and cavernous corpora fill with blood and expand. For the maintenance of erection, penile blood inflow should be in excess of retrograde flow into the circulation. This phenomenon is actualized via increase in the amount of blood entering into cavernosal corpora thanks to relaxation of smooth musculature of trabeculae and decreased return of blood into circulation due to compression of emissary veins by means of distended corpora.2,3 Besides, increase in parasympathetic tonus triggered by nerves originating from S2 to S4 which innervate cavernosal arteries and trabeculated smooth muscles and decrease in sympathetic tonus stemming from T12-L2 must accompany these vascular changes. These innervations ensures higher nitric oxide (NO) concentrations in penile tissues.2,4 With aging among essential building blocks of ED hormonal, neurologic factors, deleterious life style (smoking, alcoholism, sedentary life etc.) and comorbidities (diabetes mellitus, hypertension, obesity, coronary artery disease, drugs etc.) increase incidence of ED.5 In this study, excluding major neurological problems and considering comorbidities caused by ED and related disorders, we investigated treatability of erectile dysfunction using aerobic exercise whose applicability can be medically tested.
Materials and methodsA total of 60 patients who described ED and consulted to the outpatient clinics of Urology and Physical Therapy and Rehabilitation without any established diagnosis of neurological or psychiatric disease were included in the study. Prior to the study, hormone profiles of the patients were routinely analyzed. Patients with hormonal problems were excluded from the study. The study participants were randomized to 6 weeks of aerobic exercise (n=30) or only phosphodiesterase inhibitor therapy (n=30). All patients included in the exercise program were consulted as for the evaluation of their cardiopulmonary status and patients with higher risk were excluded from the study. The patients included in the exercise program were subjected to vigorous aerobic exercises under the surveillance of a physiotherapist and a physician for 3 days a week and 75min a day in our Physical Therapy and Rehabilitation Unit. In the medical therapy group, the patients received daily doses of 5mg tadalafil. All patients were requested to complete International Index of Erectile Function (IIEF-5) and quality of life (SF-36) forms before and after the treatment.
Statistical analysisFor statistical analysis NCSS (Number Cruncher Statistical System) 2007&PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah, USA) program was used. In the evaluation of study data, descriptive statistical methods (means, standard deviation, median, frequencies, ratio and minimum, maximum) were used. For the comparison of quantitative data and pair wise comparisons of variables without normal distribution Mann–Whitney U test was used. For the evaluation of qualitative data, Pearson's chi-square, Fisher's Exact Test and Yates Continuity Correction Test (chi-square test with Yates correction) were employed Statistical significance was evaluated at p<0.01and p<0.05.
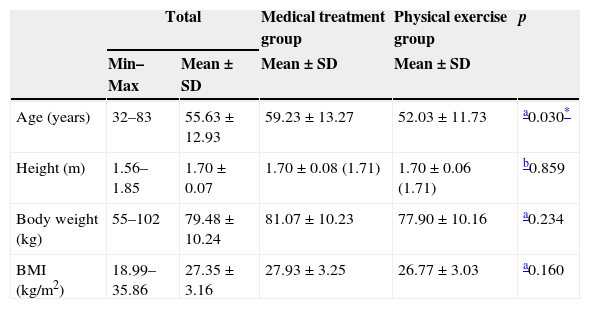
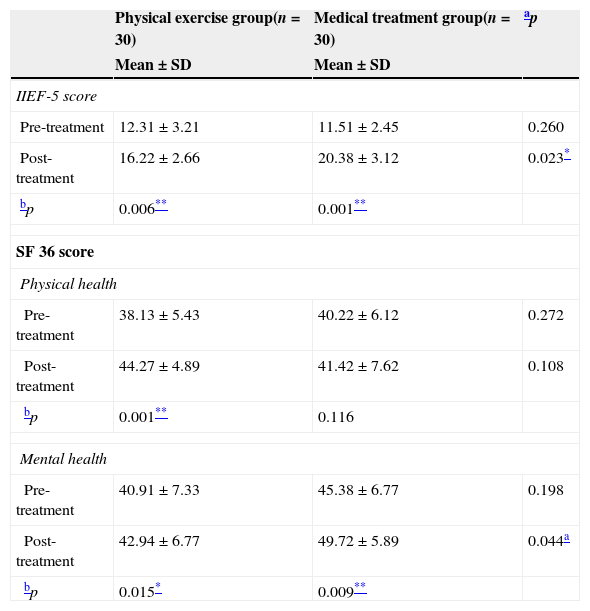
ResultsMedian age of the patients was 55.63±12.93 (range: 32–83) years with body mass index (BMI) ranging between 18.99 and 35.86kg/m2 (Table 1). Mean age of the cases in the physical exercise group was significantly lower relative to those in the medical therapy group (p=0.030; p<0.05). A statistically significant difference was not detected between BMI of the two groups (p=0.160; p>0.05). Pretreatment IIEF-5 scores did not demonstrate statistically significant differences between groups (p>0.05), while significantly higher post-treatment IIEF scores were found in the medical treatment group (p<0.05). When compared with the pretreatment values, increase in post-treatment IIEF-5 scores in the patients who were under physical exercise therapy was found to be statistically significant (p<0.01). Increases in post-treatment IIEF-5 scores in patients with medical treatment were statistically significant relative to the pretreatment levels (p<0.01). Pre and post-treatment SF- 36 physical scores were not statistically significantly different (p>0.05), while in patients under physical exercise therapy, increases in post-treatment SF-36 physical scores were found to be statistically significant when compared with the pretreatment values (p<0.01). In the medical treatment group post-treatment SF-36 physical scores were statistically significantly higher relative to the pretreatment values (p<0.01). Pretreatment SF 36 mental scores did not differ statistically significantly between groups (p>0.05), however in the medical treatment group post-treatment scores were significantly higher (p<0.05). In patients who received physical exercise post-treatment SF-36 mental scores were detected to be statistically significantly higher than pretreatment values (p<0.05). In the medical treatment group, increases seen in post-treatment SF-36 mental scores were statistically significant (p<0.01). Comparisons between two groups are summarized in Table 2.
Distribution of descriptive characteristics of the physical exercise and medical treatment groups.
| Total | Medical treatment group | Physical exercise group | p | ||
|---|---|---|---|---|---|
| Min–Max | Mean±SD | Mean±SD | Mean±SD | ||
| Age (years) | 32–83 | 55.63±12.93 | 59.23±13.27 | 52.03±11.73 | a0.030* |
| Height (m) | 1.56–1.85 | 1.70±0.07 | 1.70±0.08 (1.71) | 1.70±0.06 (1.71) | b0.859 |
| Body weight (kg) | 55–102 | 79.48±10.24 | 81.07±10.23 | 77.90±10.16 | a0.234 |
| BMI (kg/m2) | 18.99–35.86 | 27.35±3.16 | 27.93±3.25 | 26.77±3.03 | a0.160 |
The comparison of the pre-/post-treatment data of the physical exercise and medical treatment groups.
| Physical exercise group(n=30) | Medical treatment group(n=30) | ap | |
|---|---|---|---|
| Mean±SD | Mean±SD | ||
| IIEF-5 score | |||
| Pre-treatment | 12.31±3.21 | 11.51±2.45 | 0.260 |
| Post-treatment | 16.22±2.66 | 20.38±3.12 | 0.023* |
| bp | 0.006** | 0.001** | |
| SF 36 score | |||
| Physical health | |||
| Pre-treatment | 38.13±5.43 | 40.22±6.12 | 0.272 |
| Post-treatment | 44.27±4.89 | 41.42±7.62 | 0.108 |
| bp | 0.001** | 0.116 | |
| Mental health | |||
| Pre-treatment | 40.91±7.33 | 45.38±6.77 | 0.198 |
| Post-treatment | 42.94±6.77 | 49.72±5.89 | 0.044a |
| bp | 0.015* | 0.009** | |
IIEF-5, International Index of Erectile dysfunction; SF-36, Quality of Life Scale Short Form.
Epidemiological studies conducted up to now, have demonstrated that sedentary life is closely related to the comorbidities of ED. In a meta-analysis, patients who were physically active and those leading a sedentary life were compared and a relative risk of 0.53 was detected in favor of ED.6 Besides, some studies have revealed that physical exercises can remedy these comorbidities by themselves or together with various modifications in life style.
Because of its various etiological factors, management of ED requires a multidisciplinary approach. In our study, we tried to rule out psychiatric, neurological and hormonal etiologies. Causes of ED potential vascular pathologies related to aging, which we could not completely verify with radiological and laboratory tests (as endothelial dysfunction), and androgen deprivation were implicated and accordingly the patients were included in various treatment protocols. However we know that all of these causes are interrelated and none of them are local etiological factors. They are in fact outcomes of systemic responses.
Curative effects of physical exercise on both ED and androgen deprivation have been indicated.7 Many relevant mechanisms of ED have been described. These mechanisms involve adipose tissue, skeletal muscle, decreased production of cytokines from endothelial cells and mononuclear cells, increase in NO biocompatibility, enhancement in antioxidant defense mechanism and endothelial regenerative capacity.8 However, as observed by many authors, exercises do not change levels of plasma vascular endothelial growth factor (VEGF) and erythropoietin.9 Many studies have analyzed the correlation between physical exercise and androgen levels. In individuals indulging in physical exercises, higher total testosterone and sex hormone binding globulin (SHBG) but lower free testosterone levels have been detected.10
One of the debates on physical exercise is related to its duration. Nowadays, uncertainties are related to the duration and dosage of exercise.11 Various studies have indicated that based on the body weight of the patient, an individual performing an aerobic activity of moderate intensity lasting for 150min or vigorous activity of 75min a week will spend 800–1200kcal (3349–5023kJ) which might be sufficient for an adequate endothelial function.12 In our study, patients in the exercise program were enrolled into a vigorous aerobic exercise program lasting for 75min a day for 3 days a week. In the current management of non-psychogenic ED, in addition to modifications in life style, medical treatment with phosphodiesterase inhibitors takes the first place. The success rates of this treatment approach vary between 60 and 80 percent. Among life style changes, physical exercise has an important role. When the literature is screened regarding treatment success of physical exercise, a clear-cut success rate has not been described. However, a significant improvement has been demonstrated when compared with those leading a sedentary life and placebo. In another study, an increase in IIEF scores from 13.6 up to 17 was displayed with physical exercise while any change could not be detected in IIEF scores of the control group.13 However in our study, we observed increases in mean IIEF scores from 11.51±2.45 up to 20.38±3.12 in the medical treatment and from 12.31±3.21 up to 16.22±2.66 in the exercise group.
In another study, Maresca et al. collected 20 male patients affected by ED with metabolic syndrome and patients were subdivided into two groups. First group was maintained only on tadalafil therapy. The second group also continued tadalafil and furthermore they underwent a 2-month exercise training program. Although both groups showed at 2 months an improvement of the IIEF score, this was more evident in the tadalafil plus exercise group.14 However in our study physical treatment group did not receive additional medical therapy, still physical exercise statistically significantly increased IIEF-5 scores.
As in man; smoking and alcohol cessation, dietary modification, incorporation of stress-reducing techniques, routine physical exercise, and treatment of medical conditions such as diabetes and hypertension that may predispose women to female sexual dysfunction (FSD) are essential lifestyle modifications that have been reported to improve female sexual functioning.15 In one of the studies related to the correlation between exercise, and female dysfunction, in patients with sexual dysfunction who had practiced pelvic floor exercises because of incontinence, a significant improvement was observed in their FSD after physical exercise.16
Restrictive elements of our study are the small number of participants and the absence of tadalafil plus exercise group. There is a need for further prospective studies on this issue. All in all, it has been understood that physical activity induces increases in both pelvic blood supply and penile oxygenation (improvement in endothelial function), and exercise capacity achieved secondary to weight loss, these all have favorable effects on the maintenance and recovery of penile erectile function.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestWe have no conflicts of interest to declare.