


To evaluate the results of erectile function rehabilitation with sildenafil after laparoscopic radical prostatectomy (LRP).
Materials and methodsWe have evaluated on a retrospective way a subgroup of LRP with neurovascular bundles sparing that have followed a treatment schedule for erectile function rehabilitation based on sildenafil citrate. We defined the initial erectile function state as penetrate without drugs, with drugs and do not penetrate. A comparison with the erectile function after the treatment was performed. Data were analyzed at our biostatistics section.
ResultsWe selected a total of 33 patients, 7 with unilateral neurovascular bundles sparing and 26 with bilateral neurovascular bundles sparing treated with sildenafil citrate after surgery. The recuperation rate of erectile function with bilateral sparing was 80.7%. This success rate reaches 87.5% in patients <70 years old. In the unilateral sparing group the success rate was 85.7%. Two patients abandoned the treatment schedule.
ConclusionsLaparoscopic radical prostatectomy with neurovascular bundles sparing offers a high preservation rate of erectile function on expert surgeons. The maintenance treatment with phosphodiesterase-5 inhibitors may offer benefits for the erectile function rehabilitation and it has to be initiated as soon as possible.
Evaluar los resultados de la rehabilitación de la función eréctil con sildenafilo tras prostatectomía radical laparoscópica (PRL).
Material y MetodosHemos evaluado de forma retrospectiva un subgrupo de PRL con preservación de haces neurovasculares que han seguido una pauta de tratamiento para la rehabilitación de la función sexual con citrato de sildenafilo. Se ha definido el estado basal de la función eréctil como “penetra sin fármacos”, “penetra con fármacos” y “no penetra”. Se compararon los resultados antes y después del tratamiento. Los datos fueron analizados en nuestra sección de bioestadística.
ResultadosSe han seleccionado un total de 33 pacientes, 7 con preservación unilateral de haces neurovasculares y 26 con preservación bilateral. La tasa de recuperación de la función eréctil con preservación bilateral es del 80.7%. Esta tasa alcanza el 87.5% en pacientes<de 70 años. Para el grupo de preservación unilateral la tasa es de 85.7%. Dos pacientes han abandonado la terapia.
ConclusionesLa PRL con preservación de erectores ofrece una elevada tasa de conservación de la función eréctil cuando es llevada a cabo por cirujanos expertos. La terapia mantenida con iPDE5 puede ofrecer beneficios para la rehabilitación de la función eréctil y debe administrarse lo antes posible.
Since the development of radical prostatectomy there is significant interest from the urologist to indemnify and solve the deleterious effects of radical surgery in the treatment of prostate cancer: urinary incontinence and erectile dysfunction (ED).
With refinement of the surgical technique described by Walsh and Mostwin, the results in terms of potency markedly improved.1 However, the more demanding surgical procedures that improve the functional outcomes achieved a limited popularization in urologic community. Some single surgeon series reaches preservation of potency after radical prostate surgery in 70–86% of cases, but the average rates of erectile function preservation in the global urological community are 21–50%.2–4 Nowadays this situation continues despite the renewed interest in erectile function after radical prostatectomy with the advent of laparoscopic surgery.
Only a refined approach of neurovascular bundles sparing, and therefore the surgeon experience, allows greater preservation of sexual potency.
The last example of the interest to treat ED after radical prostatectomy surgery is defined by what is now known as post-surgical rehabilitation of erectile function. There are two lines of thoughts or schools on the beneficial effects of phosphodiesterase-5 (PDE5) inhibitors in this group of patients: the first is that PDE5 inhibitors produce an increase in penile tissue oxygenation, and the second is that PDE5 inhibitors are antifibrotic substances whose the main mechanism of action is to inhibit oxidative stress in cavernous tissue secondary to neurotomy.
The fundamental cause of ED is the damage to the neurovascular bundles during the surgical procedure which involves the disruption of normal neurotransmission during the erection. As consequence, several changes occurs in the corpus cavernosum: increased collagen content, decreased smooth muscle cells, decreased blood flow, hypoxia, fibrosis and finally cell apoptosis.
The cascade of events produced by penile denervation includes an increase of free radicals that induce apoptosis of vascular endothelium, a dramatic decrease in the activity of endothelial and neural NO synthetases, a decrease in the content of smooth muscle cells and their proliferation index (which explains the loss of weight of the corpus cavernosum), increased profibrotic factors (TGFβ1), and finally, a veno-occlusive ED is establish. All these changes are immediately started since cavernous nerve injury occurs, and therefore, time is a critical variable to be considered in terms of etiology and also in terms of treatment.
The goal of erectile function rehabilitation is to reverse the described cascade of events. There is sufficient pathophysiological basis for the rehabilitation of erectile function in an early stage: (1) in muscle cell cultures, cavernous hypoxia induces TGF – β1 and subsequent penile fibrosis, (2) The synthesis of phosphodiesterase-1 (which inhibits collagen synthesis dependent of TGF – β1) in the cavernous muscle is oxygen dependent, (3) in rats animal model is evidenced the overexpression of TGF – β1 and collagen after cavernous nerve injury by penile biopsy, (4) nocturnal erections have a protective role of hypoxia in penile flaccidity, so the absence of erections during the neurapraxia induce persistent penile hypoxia, (5) User et al. in the animal model demonstrates an important apoptotic index in the smooth muscle cell and a major replacement of erectile tissue by collagen and Iacono et al. obtained similar results in humans,5,6 and (6) Mulhall et al. and Montorsi et al. show that the veno-occlusive dysfunction increases with time after surgery and that early treatment could significantly reduce the incidence of venous leak7,8.
The aim of our study is to evaluate the results of erectile function rehabilitation with sildenafil after laparoscopic radical prostatectomy (LRP).
Materials and methodsWe retrospectively reviewed a subgroup of LRP with neurovascular bundles sparing performed in our institution in the period 2008–2012 which have followed a schedule of erectile function rehabilitation based on sildenafil citrate, a PDE5 inhibitor.
Preoperative and postoperative evaluation of erectile function was based on clinical history and is summarized in the following items: (1) penetrates without drugs, (2) penetrates with drug and (3) does not penetrate. For the final evaluation we conducted a telephone interview in order to update or confirm the data collected in the clinical history.
We have selected a total of 33 patients, in all cases we performed a transperitoneal LRP with a descending neurovascular bundle sparing technique as described previously.9 All patients were advised to take sildenafil citrate 50mg/night 2 days per week, allowing doses of 100mg independently of maintenance therapy during the attempt of sexual intercourse.
Descriptive data was analyzed at our biostatistics section by a certified statistician using the software SPSS 20. The results are reflected in terms of numbers, range and average.
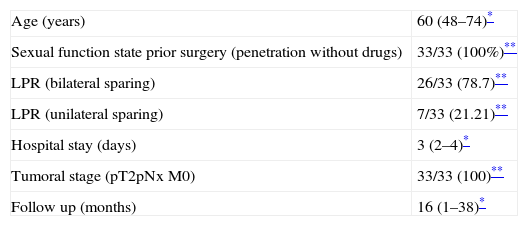
ResultsInstitutional Review Board (IRB) approval was obtained for this work. We have selected a total of 33 patients, 7 with unilateral neurovascular bundles sparing and 26 with bilateral neurovascular bundles sparing. All patients had good sexual function prior to surgery defined by penetration without drugs. Patients data is summarized in Table 1.
Patients data summarized.
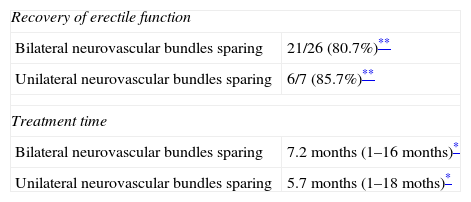
The recuperation rate of erectile function with bilateral neurovascular bundles sparing was 80.7%. Dividing the patients in a sub group of <70 years (26 patients), this success rate reaches 87.5%. In the unilateral neurovascular bundles group the rate was 85.7%. Two patients have abandoned the treatment schedule. Only 1 patient has discontinued treatment due to side effects (headache) and another patient due the cost and lack of interest, but he reflected that the response to treatment was positive. (See Table 2)
Recovery of erectile function.
The average time with sildenafil treatment for unilateral neurovascular bundles sparing group was 5.7 months (1–18 months) and for the bilateral neurovascular bundles sparing group was 7.2 months (1–16 months). The average follow-up time was 16 months (1–38 months).
DiscussionWe understand as erectile function rehabilitation after radical prostate surgery to all measures (drug or device) designed to maximize the recovery of erectile function. Schemes have been proposed for rehabilitation such as intracavernous injections, vacuum devices, intraurethral alprostadil, PDE5 inhibitors, and combination therapy.10
The erectile function rehabilitation after radical prostatectomy is a term used for the first time by Montorsi in 1997 after demonstrating the benefits of using intracavernous injections to restore erectile function in patients undergoing radical prostatectomy.8
Although the benefit of erectile function rehabilitation is widely proven, many gaps that have not been clarified still persist. We do not know if such therapies are effective in all cases or if there is a group of patients most likely to benefit, there is no evidence on which therapies are more or less effective. Regarding PDE5 inhibitors, there is no evidence showing the right moment to initiate therapy or the best dosage or the optimal treatment duration. There is controversy about the true benefit of treatment with PDE5 inhibitors when translated to clinical application.
Regardless of PDE5 inhibitor used for ED after radical prostatectomy, there are determinants factors in the response rate such as the erectile function prior to radical surgery, age and time of medical treatment initiation after surgical procedure.11
There are sufficient grounds based on animal studies for treatment with sildenafil after prostate radical surgery. Treatment with sildenafil in the animal model with rabbit smooth muscle cells decreases the formation of superoxide (free radical). Other studies have shown an increased release of cGMP that produces an overexpression of nitric oxide synthase and consequently the release of NO, which results finally in reduced penile fibrosis and less decrease of smooth muscle cell. From these studies it is concluded that sildenafil protects against apoptosis of smooth muscle cells. Also, it has been attributed to sildenafil a protective role of hypoxic damage at the adrenergic and cholinergic receptor and post-receptor systems that plays a role in erectile function, as well as a possible role in activating genes associated with cell proliferation factors in corpus cavernosum smooth muscle cells (like EREG and PDGF) and a possible inhibitory role of profibrotic related factors (such as CTGF and TGF β2) muscle genes.12–19
In clinical practice, the response rates to sildenafil after radical prostatectomy range between 50 and 80% depending on the time when the treatment is started and whether a unilateral or bilateral sparing is performed. The most important conclusion of different series is that a proper technique for neurovascular bundles sparing is essential for a better response to treatment with sildenafil citrate20–22. Our center experience in more than 1500 LRP reinforces the possibility of a positive outcome in terms of functional outcomes.
In initial series, sildenafil treatment starts late and the best response is found in the cases of bilateral sparing; also they report that the period between 18 and 24 months after surgery is the optimal to get the maximal response to treatment, corresponding to evidence of neurapraxia.23–25
In the series published by Ogura et al. in 2004 on the Japanese population is evidenced that up to 12.5% of patients treated with sildenafil, did not needed it later, suggesting the possibility of a rehabilitation effect of postoperative erectile dysfunction after sildenafil treatment.26 Equally illustrative work published by Raina et al. in 2003 on a population of responders of a series published 3 years before, in which 72% were treated with sildenafil, 31% doubled the dose to 100mg and up to 27% abandoned the treatment, 50% of them because they obtained sufficient erection to penetrate without the treatment27.
As consequence of the findings in animal models, the responses in clinical trials as those referred previously and due to the work done by Montorsi et al. in 1997, the possibility of a rehabilitation treatment of erectile function after radical surgery is real.8 In 2004 Schwartz et al. demonstrates that early and sustained treatment with sildenafil involves an increase in the content of smooth muscle cells of the corpus cavernosum, and no patient presented a content of smooth muscle cells below to 36%, which is clinically associated with the development veno-occlusive dysfunction (fundamental cause of ED after radical prostatectomy). These findings suggest a possible protective role of sildenafil by releasing NO and amplification of nocturnal erections.28
In 2008 Padma-Nathan et al., in a randomized double-blind study show that continuous and prolonged therapy with sildenafil citrate improves recovery of erectile function compared to placebo (27% vs. 4%).29 In a subsequent subanalysis in which plethysmography is performed to patients undergoing bilateral neurovascular bundles sparing surgery concludes that prolonged and continuous treatment with sildenafil facilitates the recovery of nocturnal erections and sexual function in a considerable percentage of patients.30
The evidence on the possibility of recovering erectile function up to 2 years after radical prostatectomy is very powerful. We may ensure that patients who are treated with some form of erectile function rehabilitation get better prognosis of postoperative erectile dysfunction regardless of the therapy chosen.31,32
It is not only important to know the period in which we may act to improve erectile function after radical prostatectomy, it is equally important the timing in which it is decided to initiate such treatment. Mulhall et al. in 2010 studied this aspect highlighting the importance of early treatment. They conclude that the delay in starting the rehabilitation treatment influences negatively the prognosis of erectile function after radical prostatectomy, so they advise starting the therapy in the first 2 months after surgery. Furthermore, starting treatment 10 months after surgery is associated with the development of moderate-severe ED in the long term.33
Because of all the previously exposed, we opted for a rehabilitation therapy of erectile function after LRP based on PDE5 inhibitors. Since most animals and clinical experience in this field is based on sildenafil citrate we chose to use it in our series although we could use any PDE5 inhibitor.
When we decided to conduct a rehabilitation treatment, we ran into a major stumbling block: to not know how to define the most suitable dosage. Since in the literature is evidence that the patient may benefit from therapy as early as possible, we started this treatment at the first visit after surgical discharge, approximately 4 weeks after LRP. Deciding the dosage, we wanted to find a balance between what may be therapeutic and what may be economically acceptable by the patient (Sildenafil citrate 50mg/night 2 days per week). It is essential to clearly explain to the patient and his partner the goal of maintenance therapy and realistic expectations they might wait, in a bid to ensure adherence to treatment. Finally, and in consideration of the urologist and the patient in function of the evolution, we offer the possibility to receive “demand” sildenafil in a maximum dose of 100mg without leaving the maintenance therapy except of the cases where we archived a recovery of the erectile function. We always do a review after a year of maintenance therapy to decide whether to abandon or extend it up to 18 months, as we understand that deadlines are reasonable to assess adequately to the response to treatment.
In this small series, our rate of erectile function recovery was 80.7% (21/26), and it reaches 87.5% (21/26) in patients <70 years for those undergoing bilateral neurovascular bundles sparing, and 85.7% (6/7) for those undergoing unilateral neurovascular bundles sparing. The recovery time is variable in different patients and goes from an almost immediate recovery a month after surgery until a recovery beyond the year of LRP. Clearly, with this small sample of maintenance therapy and following a personal and specific scheme, we may not draw firm conclusions about the benefits of maintenance therapy. However, as presented in the literature, we conclude that the imperative condition to obtain good results in erectile function after LRP is to provide a refined surgical technique, which is directly proportional to the surgeon experience. It is difficult to draw conclusions about the benefits of maintenance treatment since there are many factors that influence: the surgeon, the performance status of the patient, comorbidities, age, etc. However, we think there are two factors that we are able to control: surgical technique and postoperative erectile dysfunction, minimizing it by any method that promotes oxygenation of the corpus cavernosum and thus combat the deterioration of erectile tissue.
Unfortunately our series is too short to allow firm conclusions regarding our maintenance schedule with sildenafil for erectile function rehabilitation after radical prostatectomy. It would also be desirable to carry out a comparative analysis between the maintenance dose and the demand dose for a specific surgical technique.
ConclusionsLRP in experienced hands offers excellent functional results, being a guarantee when it is performed to patients <70 years.
There is sufficient evidence on the benefits of the erectile function rehabilitation after surgical treatment of prostate cancer. The pernicious effects of radical prostate surgery on erectile function are established from the time of surgery, so any rehabilitation therapy must be initiated as soon as possible. Maintenance therapy should be maintained until it takes effect at least during 1-year.
The pattern of sildenafil citrate 50mg/night 2 days a week may be a valid option when rehabilitation treatment for erectile function is opted.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestAuthors declare that there are not any competing financial interests in relation to the work described.