


Several studies have suggested empathy impairment in psychopathy. It has been highly associated to violent and criminal behavior. Empathy is not a univariate concept; however, studies about the role of empathy components in this population are inconclusive and they are mostly made in forensic samples.
ObjectiveTo explore the relationships of psychopathy with the empathy dimensions and to probe if there is a continuum considering general population and forensic groups.
Material and methodsEighty adult males were recruited and divided into three groups: control group (healthy man from general population; n=21), violent group 1 (violent men from general population; n=24) and violent group 2 (criminal offenders; n=35), who were case files of inmates in high security prisons in Mexico. All subjects were assessed with an aggression questionnaire (RPQ), a Psychopathy checklist (PCL-R; SV) and an empathy scale (IRI). One-way analyses of variance (ANOVAs) were carried out to compare age, education years, empathy factors and psychopathy scores between groups; we also conducted regression analyses to probe the effect of psychopathy on each empathy subscale.
ResultsWe found psychopathy differences between groups where violent group 2 obtained the highest scores, followed by the violent group 1 and the controls with the lowest scores. The perspective taking subscale showed differences between the control group and the two violent groups; the violent groups did not differ. Additionally, there were significant differences in the personal distress subscale between the three groups where violent group 2 had the highest scores. Moreover, we found a positive association between personal distress sand psychopathy; meanwhile, perspective taking scores were negatively associated with psychopathy.
ConclusionsPsychopathy and violent behavior are known for a lack of empathy; however, the empathy dimensions provide a better understanding of the mechanism underlying this non-prosocial behavior.
Estudios han sugerido que la empatía está afectada en la psicopatía. La psicopatía ha sido asociada con la conducta criminal y violenta. La empatía no es un concepto unitario, sin embargo, los estudios acerca sus componentes en este tipo de poblaciones han sido controversiales; además la mayoría se han hecho en poblaciones institucionalizadas.
ObjetivoExplorar la relación entre la psicopatía con los componentes de la empatía y probar si existe un continuo considerando grupos institucionalizados y de la población general.
Materiales y método80 adultos del sexo masculino divididos en 3 grupos: grupo control (hombres sanos de la población general; n=21), grupo violento 1 (de la población general; n=24) y grupo violento 2 (criminales en reclusión; n=35). Los sujetos se evaluaron con un cuestionario de agresión (RPQ), una escala de Psicopatía (PCL-R; SV) y otra de empatía (IRI). Para las comparaciones entre los grupos se llevaron a cabo ANOVAs, así como análisis de regresión para probar los efectos de la psicopatía y las subescalas de empatía.
ResultadosSe encontraron diferencias significativas los niveles de Psicopatía entre los grupos donde el grupo violento 2 obtuvo los puntajes más altos, seguido por el grupo violento 1 y el grupo control. Las diferencias en la “empatía perspectiva” fueron entre el grupo control y los dos grupos violentos; en “angustia personal” entre los tres grupos, donde el grupo violento 2 obtuvo los puntajes más altos. Se encontraron correlaciones significativas con la psicopatía: una positiva con la angustia personal y otra negativa con la “toma de perspectiva”.
ConclusionesLa psicopatía y la conducta violenta se caracterizan por una falta de empatía, los factores que componen a la empatía proveen mayor información para el entendimiento de los mecanismos que subyacen este tipo de conductas.
Empathy has been defined as the capacity to understand and appreciate the emotional states and needs of others in reference to oneself.1 However, currently there is no unified concept since several authors have recognized empathy as a multidimensional phenomenon. Some authors2 have made the initial differentiation between instinctive sympathy (or empathy), which he described as a quick, involuntary, seemingly emotional reaction to the experiences of others, and intellectualized sympathy, or the ability to recognize the emotional experiences of others without any vicarious experiencing of that state. A vicarious activation is defined as the neural activation that occur automatically by witnessing the emotions of others,3,4 so witnessing what others do and sense recruits one's own motor and somatosensory cortices.5–8 Spencer,9 a hundred years before, drew the same distinction, and the instinctive/intellectual or cognitive/emotional partitioning of empathy has continued to this day.
According to Davis10 empathy measurement should provide separate assessments of (1) the cognitive, perspective-taking capabilities or tendencies of the individual, and (2) the emotional reactivity. He proposed 4 empathy subscales that include: (1) fantasy, which denoted a tendency of the respondent to identify strongly with fictitious characters in books, movies, or plays; (2) perspective-taking, which reflected a tendency or ability of the respondent to adopt the perspective, or point of view, of other people; (3) empathic concern, these items assessed a tendency for the respondent to experience feelings of warmth, compassion and concern for others undergoing negative experiences; and (4) personal distress, which indicated that the respondent experienced feelings of discomfort and anxiety when witnessing the negative experiences of others. The providence of different empathic components in each individual will allow a better understanding of their effects on behavior.
It has been pointed out that the experience of empathy can lead to sympathy or empathic concern for another based on the apprehension or comprehension of the other's emotional state or condition; however, it could also be aroused by personal distress, i.e. an aversive, self-focused emotional reaction to the emotional state or condition of another. Feelings of personal distress (i.e. alarmed, upset, worried, disturbed, distressed, troubled, etc.) seem to evoke egoistic motivation to reduce one's own aversive arousal; thus, personal distress evokes egoistic motivation to have one's own vicarious emotional arousal (distress) reduced, whereas empathy evokes altruistic motivation to have the other's need reduced.11
Importance of empathy in pro-social behaviorEmpathy is a crucial component of human emotional experience and social interaction. The ability to share the affective states of both our closest ones and complete strangers allows us to predict and understand their feelings, motivations, and actions.12
Some developmental psychologists have hypothesized that empathy and sympathetic concern for others is an essential factor inhibiting aggression toward others.13,14 Empathy may be regarded as a proximate factor motivating pro social rather than antisocial behavior.15 It is commonly defined as an affective reaction that is appropriate to someone else's situation rather than one's own. Some researchers have theorized that there should be a relation between aggressive behavior and a lack of empathy.16
The propensity for aggressive behavior has been hypothesized to reflect a blunted empathic response to the suffering of others.17,18 Such a lack of empathy in aggressive individuals may be a consequence of a failure to be aroused to the distress of others.19 In line with this hypothesis, it has been suggested that aggressive behavior arises from an abnormal processing of affective information, resulting in a deficiency in experiencing fear, empathy, and guilt, which normally would inhibit the acting out of violent impulses.20,21
A hallmark characteristic of adults with psychopathy (PCL-R) and youths with conduct disorders of the limited pro social subtype (DSM-V) is reduced empathy. Considering then that empathy is not a unitary concept, Keysers and Gazzola22 asked the question: Are Psychopaths unable to empathize, or are they simply less likely to empathize in certain situations? Psychopathic criminals can be charming and attuned while seducing a victim, thereby suggesting empathy and cognitive components from empathy, but at the same time later they become callous while raping a victim, or killing it thereby suggesting impaired empathy related to the emotional components of empathy. In order to characterize empathy accurately it may be necessary to measure empathy in multiple representative situations and to determine where empathy might be abnormal and where it is preserved.
Neurobiology of empathy and psychopathyDeep analysis of how neurons contribute to the ability and propensity for vicarious activation, and how these shape the ability and propensity for empathy, has not been an easy job. However, replacing a univariate notion of empathy for each facet with a more multivariate landscape of capacities and propensities shaped by attentional and motivational factors will be necessary to capture the complexity of disorders where empathy is thought to be impaired like in psychopathy and autism.22
Emotion recognition deficits in psychopathy are thought to be the result of amygdala hypoactivity, and are believed to be at the core of psychopaths’ callous lack of empathy.23 Alternatively, similar findings in autism may stem from more general impairments in the processing of facial stimuli, including abnormal functioning of the fusiform face area in the fusiform gyrus,24–26 an essential structure for the cognitive representation of facial stimuli.27
Keysers et al.28 based on these facts proposed that separate systems support the capacity to think what another is thinking (cognitive empathy) and to feel what another is feeling (emotional empathy) and analyzing the individual variability in empathy in disorders like autism, who are impaired in cognitive empathy, whereas others like psychopathy, are impaired in emotional empathy. These forms of empathy should recruit partially distinct neural substrates. Since specific lesions can impair specific domains of empathy, they suggested that neuroscientific data support that empathy is indeed composed of partly separated modalities.
The neural markers for empathy have been investigated in several psychiatric disorders, autism in particular, but surprisingly not directly in psychopaths. Researchers29 have argued that because vicariously experiencing (i.e. empathizing with) the negative emotional reactions of victims may inhibit aggression. The increased instrumental aggression in psychopathy might be related to their reduced vicarious experience of the other's emotions. They conducted a study comparing brain activity of 18 psychopathic offenders with 26 control subjects while viewing video clips of emotional hand interactions in the conditions of love (hands caressing), pain (one hand hitting the other), social exclusion (one hand pushing away the other friendly hand), and neutral videos (approaching hand touching the other and getting a non-emotional response). They found that brain regions involved in experiencing these interactions were not spontaneously activated as strongly in psychopaths while viewing the video clips. However, this group difference was markedly reduced when they specifically instructed participants to feel with the actors in the videos. They concluded that psychopathy is not a simple incapacity for vicarious activation but rather reduced spontaneous vicarious activation co-existing with relatively normal deliberate counterparts. These data suggest that empathy factors can be psychiatrically and neurologically relevant by how deliberately one empathizes.
Regarding general population and the associations between empathy dimensions and psychopathy, researchers30 evaluated one hundred and twenty-four adult males from the community. They administered the Self-Report Psychopathy Scale 4 Short Form, and a wide battery of affect, empathy and morality tasks and questionnaires. Their findings indicate that both core affective-interpersonal, and lifestyle-antisocial features of psychopathy are associated with weaker empathic responses to fearful faces. However, only the unique variance of the affective-interpersonal features is associated with weaker empathic response to happy stories, lower propensity to feel empathic concern and less difficulty in making decisions on moral dilemmas. In contrast, the unique variance of the lifestyle-antisocial features is associated with a greater propensity to feel empathic concern. These findings suggested that, while the joint variance between affective-interpersonal and lifestyle-antisocial features might drive some ‘deficits’ associated with psychopathy, there also appears to be unique deficits associated to the core affective-interpersonal features, particularly in relation to affective aspects of moral processing.
Del Barrio et al.31 analyzed the dimensions of the IRI (Interpersonal Reactivity Index10). The sample was constituted by 721 subjects between 9 and 16 years old. Different exploratory factor analyses were conducted as base on the final confirmatory factor analyses through self-report. The results supported a coherent relationship among empathy, depression, aggression and pro social behavior. The correlation between empathy and pro social behavior was positive and negative with the others variables. Aggression correlated positively with “impassability” a factor referred for Davis as “empathic concern” and the correspondent items related to “lack of empathy” and found no relation to “intellectual empathy” or “perspective taking” in the Davis scale. The authors conclude that cognitive empathy is inversely related to aggression level and somehow compatible with emotional empathy making these individuals worse at emotional adjustment and therefore more prone to aggression since they have fewer sources to be able to stop their impulsivity and pro social behavior.
Since all the results provide non-consistent conclusions, some authors have proposed that psychopathic traits are best viewed as existing on a continuum, thus providing an empirical basis for studying individuals in terms of level of psychopathic traits rather than limiting studies to extreme groups.32 The strength of this dimensional perspective has led to a growing number of community studies on psychopathy and findings from these studies often mirror those observed in clinical/forensic samples,33,34 further strengthening the view that there are continuities between community and forensic populations in the mechanisms underlying psychopathy.30
Based on the review of the literature, the aims of the present study was first to investigate if there are differences in empathy dimensions proposed by Davis10 between a group of violent man from the general population and a group of violent criminals (incarcerated), both compared to a control group. Furthermore, the aim is also to probe if psychopathy scores can predict empathy scores in order to observe a continuum considering general population and forensic groups.
Material and methodsParticipantsEighty adult males were recruited from two different scenarios: one group (n=45) from a community sample that were divided into two different groups: control (n=21) and violent group 1 (n=24); the other group (n=35) were case files of non-psychiatric inmates detained in high security prisons in Mexico (violent group 2).
The control group21 healthy individuals from the community were included in this group if they did not apply for the cutoff point in the Reactive and Proactive Aggression Questionnaire (RPQ)34,35 (scores above eight points in the reactive aggression subscale), and/or in the Hare Psychopathy Checklist-Revised: SV (PCL-R:SV; less than 18 points). In reference to violent behavior, individuals with history of physical violence or criminal record were excluded from this group; moreover, subjects with any psychiatric or neurological disorder were excluded from the study.
MaterialsAssessment of violenceIn order to determine violent behavior within inmate offenders, files were consulted and a semi-structure interview was conducted in order to explore criminal records, social, family and occupational aspects. Individuals were classified as violent if violent crimes were reported such as injury, attempted murder and first degree murder. Any report of physical violence inside and/or outside the institution was also considered.
The general population sample were also interviewed and completed a screening questionnaire, the Spanish version of the Reactive and Proactive Aggression Questionnaire (RPQ)34,35; subjects with scores above eight points in the reactive aggression subscale were classified as violent (cutoff adjusted for Mexican population36). Within the interview, we reported any previous episodes of violence as well as the existence of a criminal record (checked online by name of each subject). In the case of violent individuals, we considered the cutoff point of the RPQ scale and the number of violent episodes and/or criminal record.
Assessment of psychopathyPsychopathy in inmates was assessed by two different raters independently, using the standardized version in Mexican inmate population of PCL-R.37 This is a 20-item, three-point scale (0–2); total score can range from 0 to 40 and reflect the degree to which the person matches the psychopathy construct. Based on Hare's Psychopathy Check List38 the interview is focused on family history, education, personal relationships, work history, juvenile delinquency, criminal career and other psychopathic traits. Also in the case of the inmates, detailed review of files provided by the prison authorities was carried out.
For the assessment in the general population sample we used the Hare Psychopathy Checklist-Revised: SV (PCL-R:SV) recommended for forensic and clinic samples (non-criminal psychopaths). The original screening version39 was later validated for Spanish population.40
Assessment of empathyThe standardized version in Spanish41 of the Interpersonal Reactivity Index10 (IRI) was used. The IRI is a 28-item measure of general empathic tendencies that assess both cognitive and affective empathy. Items are evaluated on a 5-point Likert scale ranging from 0 (does not describe me well) to 4 (describes me very well). This scale yields four subscales (Perspective Taking, Fantasy, Empathic Concern, and Personal Distress), and each includes seven items: Perspective taking that measures the ability to take another person's point of view; Fantasy that assesses the ability to share the feelings of fictitious characters in books, plays, movies, etc.; Empathic Concern examines a tendency to feel sympathy and concern for others who are experiencing misfortune, whereas Personal Distress measures the individual's own negative emotions as they relate to stressful or complicated interpersonal situations. The IRI has demonstrated good intrascale, test–retest reliability, and convergent validity.10
ProcedureAll subjects provided written informed consent for this study and were guaranteed confidentiality of the information they provided. Subjects with a history of neurological conditions, mental retardation, psychotic symptoms, or drug abuse were also excluded from this study. Ethics Committees of the participant institutions approved the study. In inmates cases it was assured that this process would not interfere with their judicial trial or sentence.
A quiet area was assigned within the prison for the assessment of the Inmate group (V2); guards were in charge of accompanying participants to the assessment room and back to their cells. The Control group and the violent group from general population (V1) were assessed at the Laboratory of Neuropsychology and Psychophysiology in the Faculty of Psychology at the National Autonomous University of Mexico. Assessments were carried by 5 psychologists previously trained and it consisted of three sessions of 2.5h each. In the first session, a clinical history was applied to obtain details about the life history of the participant and/or to dismiss those with neurological and psychiatric conditions. In the second session, a neuropsychological evaluation was carried out, and in the third session, a psychophysiological assessment was conducted using EEG and Event Related Potentials recording. For the aims of the present study, only the data from the first session were analyzed.
Data analysesThe program SPSS 19 for Windows (SPSS, Chicago, IL) was used for all the statistical analyses. A descriptive characterization of the sample by mean and range was obtained. One-way analyses of variance (ANOVAs) were carried out to compare age, education years, empathy factors (perspective taking, fantasy, empathic concern and personal distress) and psychopathy scores between groups. To further assess differences between groups in all our measures, Bonferroni post hoc correction tests were carried out. For these analyses, the significance level was established at p≤0.05.
To probe the effect of psychopathy scores on each empathy factor (perspective taking, fantasy, empathic concern and personal distress) we conducted regression analyses controlling the effects of age and education years. The significance level was established at p≤0.05.
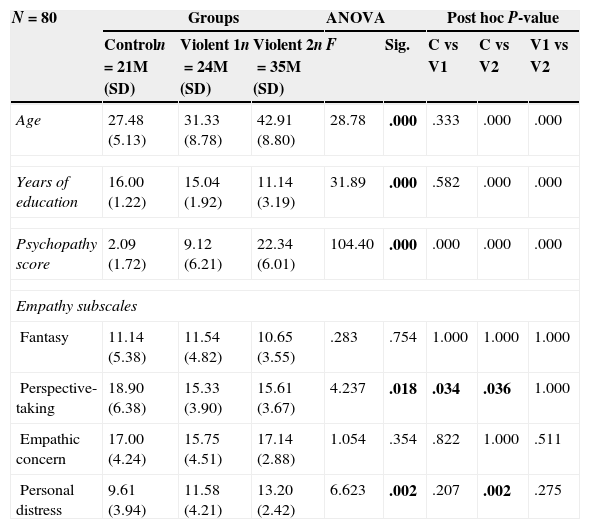
ResultsDescriptive statistics by age, years of education of the groups are presented in Table 1. Overall, the average age of the sample was 35.39 years (±10.45), and range of 21–62. The average years of education was 13.59 (±3.26), range of 6–18, and equivalent to high school.
Demographic and clinical characteristics of the groups.
| N=80 | Groups | ANOVA | Post hoc P-value | |||||
|---|---|---|---|---|---|---|---|---|
| Controln=21M (SD) | Violent 1n=24M (SD) | Violent 2n=35M (SD) | F | Sig. | C vs V1 | C vs V2 | V1 vs V2 | |
| Age | 27.48 (5.13) | 31.33 (8.78) | 42.91 (8.80) | 28.78 | .000 | .333 | .000 | .000 |
| Years of education | 16.00 (1.22) | 15.04 (1.92) | 11.14 (3.19) | 31.89 | .000 | .582 | .000 | .000 |
| Psychopathy score | 2.09 (1.72) | 9.12 (6.21) | 22.34 (6.01) | 104.40 | .000 | .000 | .000 | .000 |
| Empathy subscales | ||||||||
| Fantasy | 11.14 (5.38) | 11.54 (4.82) | 10.65 (3.55) | .283 | .754 | 1.000 | 1.000 | 1.000 |
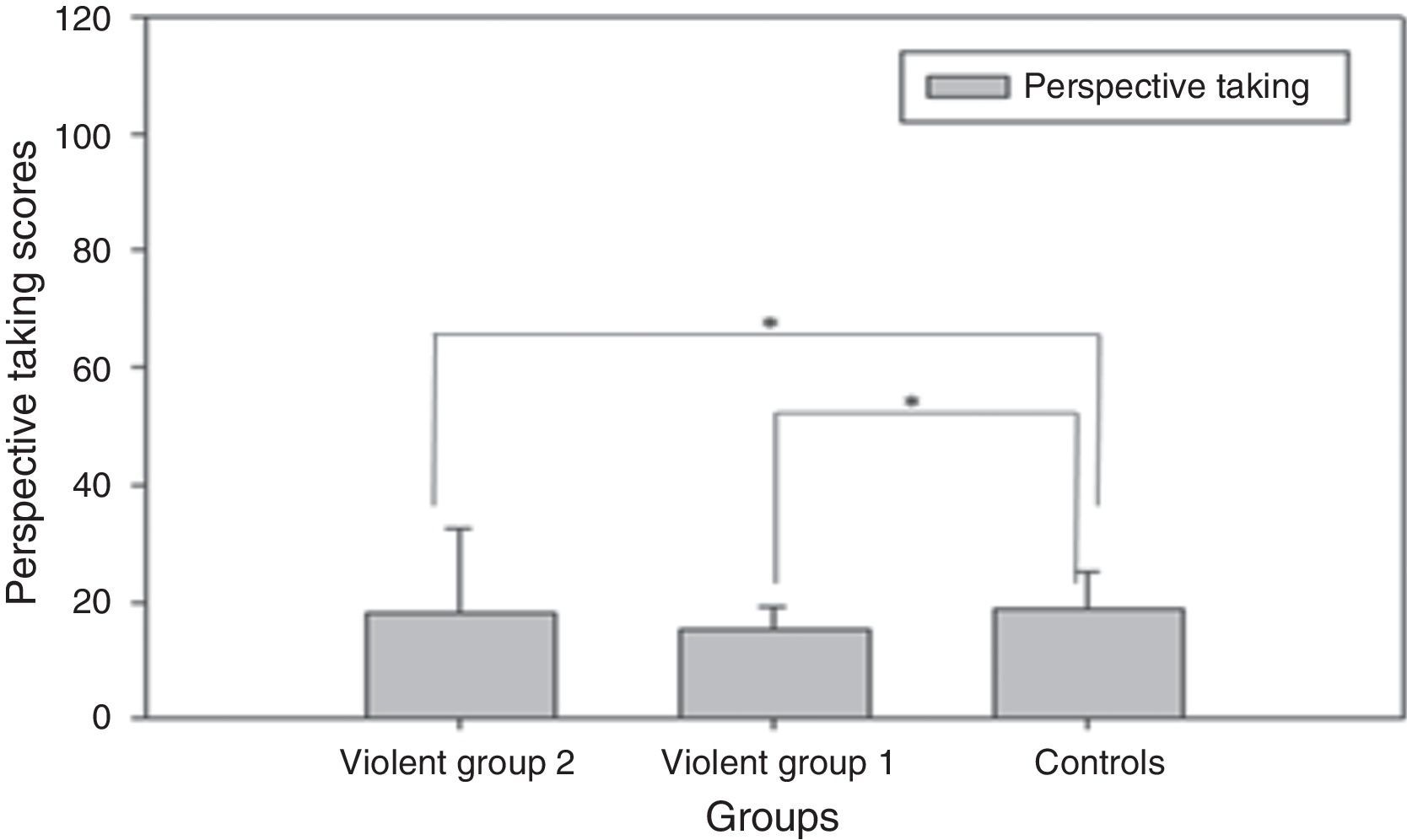
| Perspective-taking | 18.90 (6.38) | 15.33 (3.90) | 15.61 (3.67) | 4.237 | .018 | .034 | .036 | 1.000 |
| Empathic concern | 17.00 (4.24) | 15.75 (4.51) | 17.14 (2.88) | 1.054 | .354 | .822 | 1.000 | .511 |
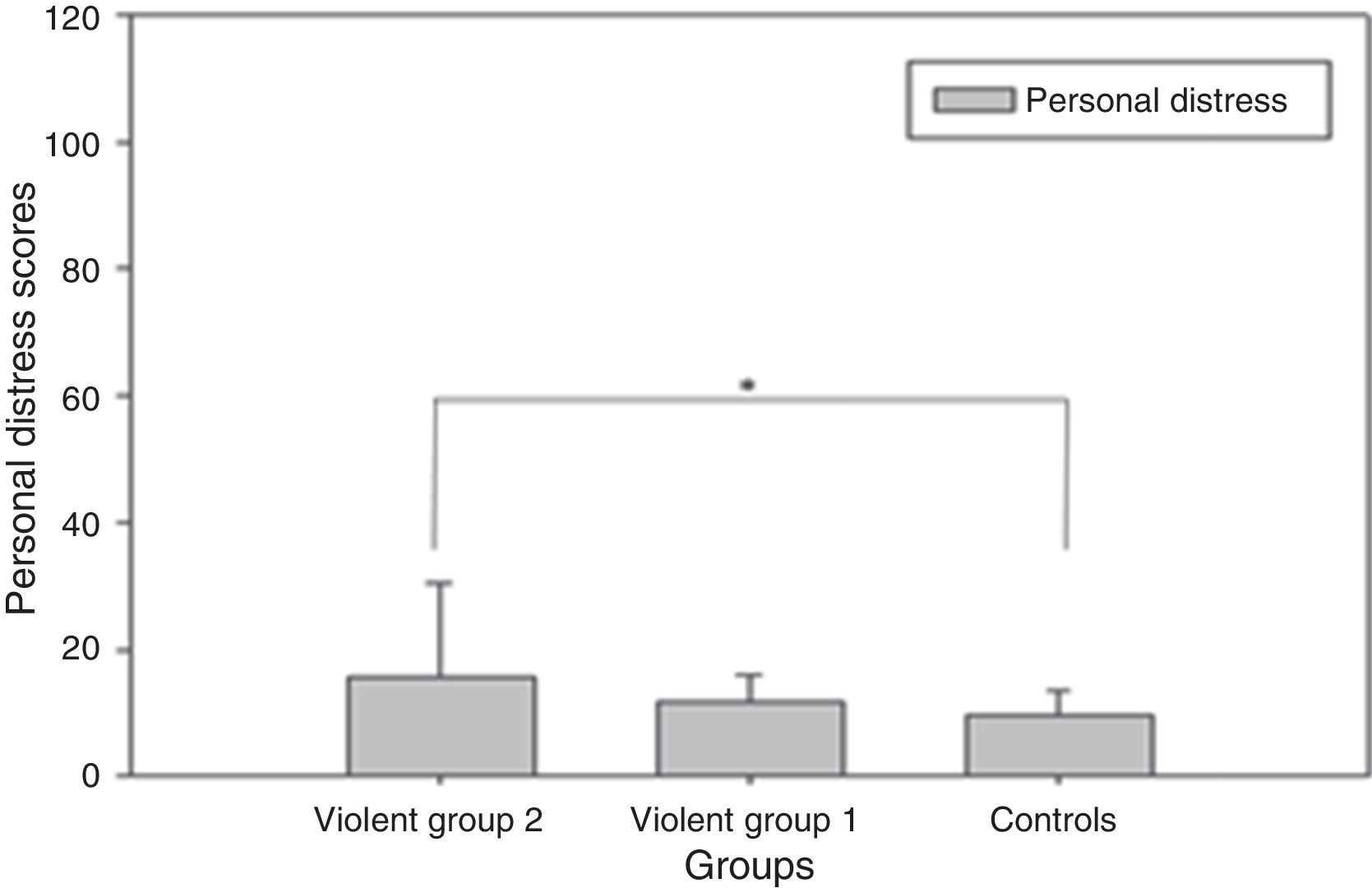
| Personal distress | 9.61 (3.94) | 11.58 (4.21) | 13.20 (2.42) | 6.623 | .002 | .207 | .002 | .275 |
The inmate group scored significantly higher on the total score (M=22.34; SD=6.01) comparing to the violent group from the community sample (M=9.12; SD=6.01) and the control group (M=2.09; SD=1.72) see Table 1.
Empathy assessmentIn the empathy subscales analysis we found significant differences between groups in the perspective taking subscale (F=4.237; p=0.018) and in the personal distress subscale (F=6.623; p=0.002). In the perspective taking subscale we found that the control group had the highest score (M=18.90; SD=6.38) compared to the violent group 1 (15.33; SD=3.90) and the violent group 2 (M=15.61; SD=3.67). No significant differences were found between the two violent groups in the perspective subscale (see Fig. 1). In the personal distress subscale we found that the group with the highest scores was the violent group 2 (M=13.20; SD=2.42) followed by the violent group 1 (M=11.58; SD=4.21) and the control group (M=9.61; SD=3.94) which obtained the lowest scores. Within this subscale the significant differences were found between the violent group 2 and the control group (M=6.623; SD=0.002) (see Fig. 2). No significant differences were found in the fantasy subscale or the empathic concern between the control group, the violent group 1 or the violent group 2 (see Table 1).


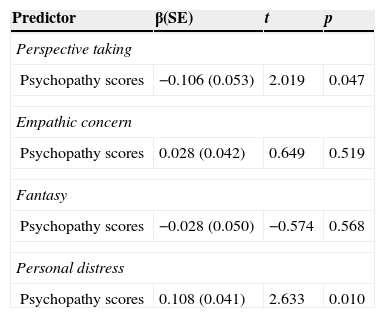
In order to explore the effect of psychopathy scores on each empathy factor we conducted regression analyses including age and years of education in the model for controlling its effects.
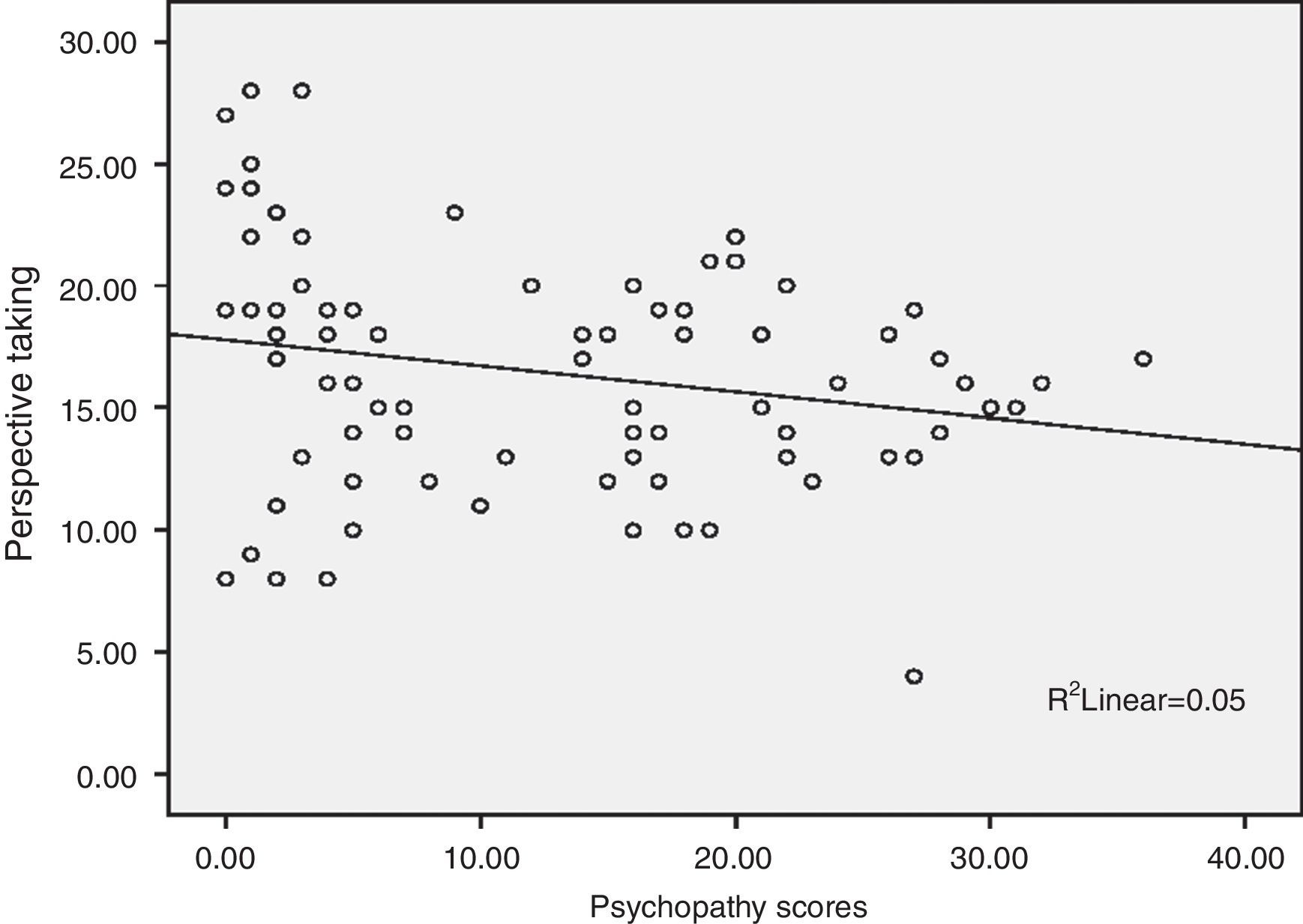
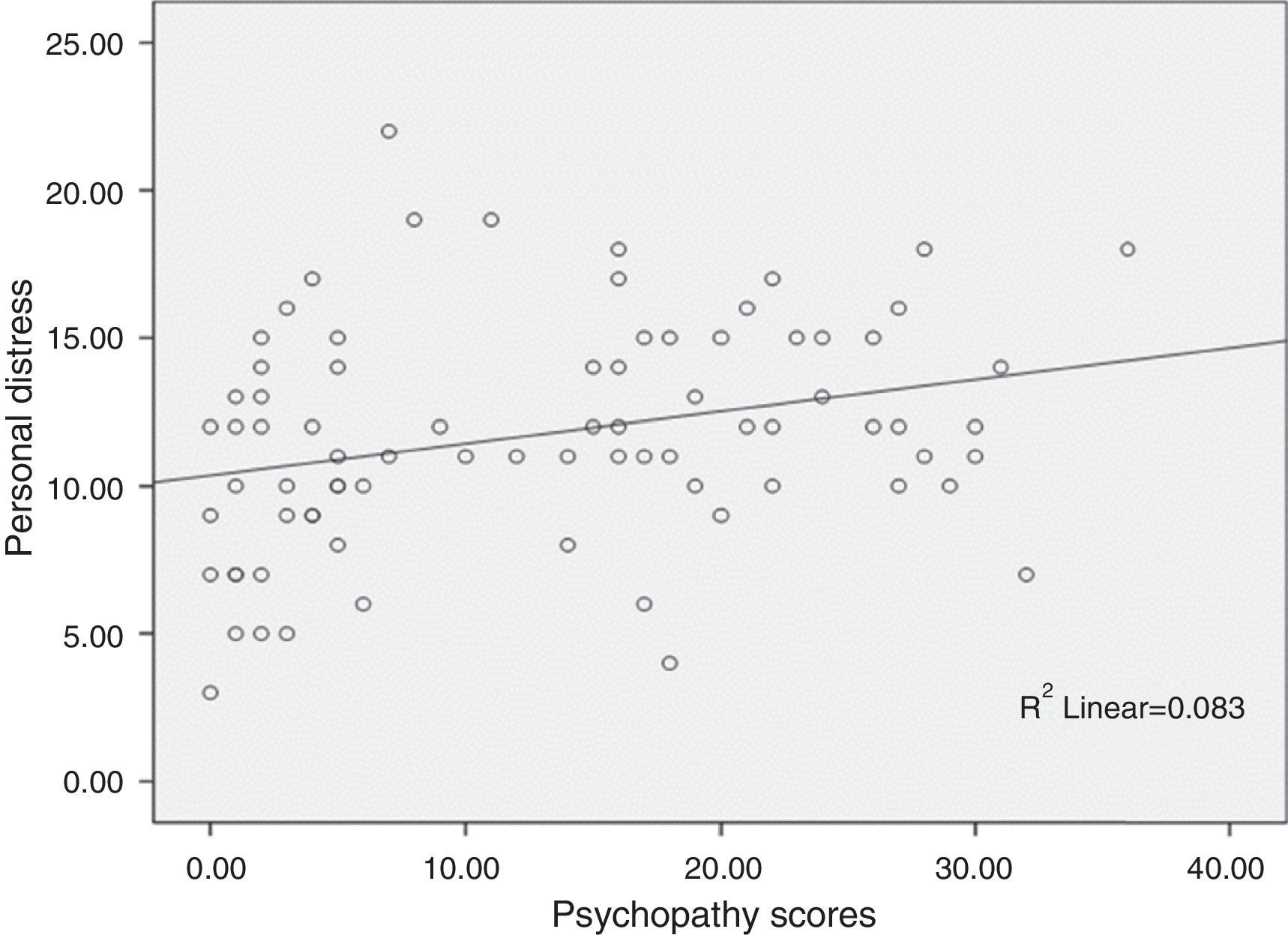
We found that psychopathy scores significantly predicted perspective taking scores and were negatively associated (Fig. 3). Personal distress scores were also predicted by psychopathy scores but were positively associated (Fig. 4). There were no significant predictions found for fantasy or empathic concern made by psychopathy scores (Table 2).


Relationship between psychopathy scores and empathy subscales.
| Predictor | β(SE) | t | p |
|---|---|---|---|
| Perspective taking | |||
| Psychopathy scores | −0.106 (0.053) | 2.019 | 0.047 |
| Empathic concern | |||
| Psychopathy scores | 0.028 (0.042) | 0.649 | 0.519 |
| Fantasy | |||
| Psychopathy scores | −0.028 (0.050) | −0.574 | 0.568 |
| Personal distress | |||
| Psychopathy scores | 0.108 (0.041) | 2.633 | 0.010 |
The aim of the present study was first to investigate if there were differences in empathy dimensions proposed by Davis10 between a group of violent man from the general population and a group of violent criminals (incarcerated), both compared to a control group. Rather than comparing extreme groups, we seek to explore if there is a continuum in the contribution of the different empathy dimensions and we included a violent non-incarcerated group. First, we compared psychopathy scores between the three groups: violent group 1 (violent group from a community sample), violent group 2 (violent inmate group) and a control group and we found the highest scores in the incarcerated inmate group which has been reported before and it has been associated to a higher propensity for violent behavior and recidivism.42–44 Despite the fact that violent group 1 did not reach scores for psychopathy, we observed that psychopathy scores were higher in this group compared to controls augmenting the probability for these individuals to engage in violent acts like felonies or aggression.
In regard to empathy scores, we found that the control group had the highest scores in the perspective taking subscale compared to both violent group 1 and violent group 2. Reduced empathy in violent groups has been extensively reported before.45,46 However, the dimensions of the empathy construct have not been widely studied,22 and up to date research has found that adults and children with high levels of psychopathic traits have a selective impairment in the recognition of others’ distress, particularly fear and sadness,47–49 which would be more related to the emotional component of empathy. However, this impairment does not appear as consistent in community samples.50 In the present study, we found that both violent groups had a very similar score in the perspective taking subscale, which would imply that both violent groups had a similar impairment in the ability to adopt the perspective or point of view of other people.10 Perspective taking is related to the cognitive component of empathy.
Several studies have found that perspective taking is both a potential inhibitor of interpersonal aggression51 and of acting out violent impulses.20,21 Recently other authors30 proposed that if you consider community and forensic populations there is a continuum in this component. Our findings do not support their speculations.
Interestingly in the personal distress component (an emotional empathy related trait), we found significant differences between the three groups, where the violent group of incarcerated inmates obtained the highest scores. Apparently, this component reflects a continuum. The control group had the lowest scores, followed by the violent group 1 and finally the violent group 2, and there was positive correlation with levels of psychopathy, thus the higher personal distress scores the higher was the level of psychopathy.
To our knowledge, there are currently no studies that related levels of psychopathy and the empathy subcomponents. Recently, in other populations authors52 have reported a correlation between high levels of IRI “Personal Distress Scale” and outward personality, defined as subjects who are more focused on a frame of references and that predominantly uses an externally anchored coordinate system to discriminate among own internal emotional states. Other authors53 have found that personal distress is unrelated or negatively related to pro social behaviors both in adults54 and in children.55 Therefore, negative emotional arousal, especially for reflective affective states such as sadness, is associated with a focus on the self. According to Eissenberg,56 the people who exhibit higher physiological arousal and who reported more distress show decreased sympathy.
In our study the personal distress subscale evaluated if the respondent experienced feelings of discomfort and anxiety when witnessing the negative experiences of others10 and it has been proposed that these feelings of personal distress (alarmed, upset, worried, disturbed, distressed, troubled, etc.) seem to evoke egoistic motivation to reduce one's own aversive arousal. Thus, personal distress evokes egoistic motivation to have one's own vicarious emotional arousal (distress) reduced, whereas empathy evokes altruistic motivation to have the other's need reduced. Then, if empathy is kept low, distress will be the predominant vicarious emotion produced by witnessing the other's suffering. This distress should produce egoistic motivation to reduce one's own aversive arousal and as a result, when empathy is low, then there should be less helping (assuming helping involves some cost). However, when empathy is high, it should be the predominant vicarious emotion, evoking altruistic motivation and this should mean that when empathy is high, if escape is easier, then there should be no reduction in helping.11
Some researchers have argued that psychopathic individuals are able to distinguish between right and wrong (using cognitive empathy) but do not care (not having emotional empathy).22 Then, although moral knowledge appears to be intact, their moral emotions appear deficient and thus failing to motivate moral behavior.31–58
Until now, research has focused mainly on the link between cognitive empathy and psychopathy. Researchers45,59 reported intact theory of mind in high-trait psychopathic individuals. In contrast Brooke and Kosson60 observed impaired empathic accuracy in criminal high-trait psychopaths.
Considering that perspective taking has been considered a prerequisite for emotional empathy,11 in the present study it is reflected that not only in how it affects violent behavior but also as mentioned by other studies,31 cognitive empathy is inversely related to aggression (and psychopathy) level. Therefore, emotional empathy disturbances affect adjustment and since the subjects have fewer sources to be able to stop their impulsivity and to have pro social behavior, they are more prone to exhibit aggressive behavior.
Decety and Lamm61 proposed a neurobiological model, in which bottom-up (i.e. direct matching between perception and action) and top-down (i.e. regulation, contextual appraisal, and control) information processes are fundamentally intertwined in the generation and modulation of empathy. In this model, bottom up processes account for direct emotion sharing which is automatically activated (unless inhibited) by perceptual input. On the other end, executive functions implemented in the prefrontal and cingulate cortex serve to regulate both cognition and emotion through selective attention and self-regulation. This meta-cognitive level is continuously updated by bottom-up information, and in return controls the lower level by providing top-down feedback. Thus, top-down regulation, through executive functions, modulates lower levels and adds flexibility, making the individual less dependent on external cues. The meta-cognitive feedback loop also plays a crucial role in taking into account one's own mental competence in order to react (or not) to the affective states of others. This model should be supplemented by top-down processes that are not classically associated with executive function and the associated neural structures, in particular those in the medial and dorsolateral prefrontal cortex.
If people can modulate their emotions as needed, their dispositional emotionality should not be an important contributor to empathy-related responding. In contrast, people high in intensity of negative emotions would be expected to be prone to personal distress if they lack the ability to regulate themselves because they will become overwhelmed by their vicariously induced negative feelings.56
Since specific lesions can impair specific domains of empathy62 the suggestion that neuroscientific data make about empathy being indeed composed of partly separated modalities should be considered. We believe that the answer to this question may be the explanation of the difference between being a violent individual who somehow manage no to engage in criminal behavior and someone who does. Even though we have no certainty that individuals from the community sample had no criminal record, we think that high psychopathy scores along with high personal distress scores both contribute to a greater propensity for violence and criminal behavior and both cognitive and emotional components of empathy would provide valuable information to be taken into account in the study of psychopathy and pro social behavior.
We recognize that it is highly important to understand the different components of empathy and its repercussions in the affected disorders. In the case of violent behavior and psychopathy, we propose to make more studies highlighting focus on the neurobiological factors and its contributions for a better designing of prevention and rehabilitation programs.
Limitations and further researchThe present study showed the possible role of psychopathy and empathy factors on violent behavior; however our design can be interpreted methodologically as biased because it is not a randomized sample since we recruited violent man from the community sample and inmates from high security prisons. Therefore we recommend taking take these results carefully for generalizing these data. Regarding this issue we propose to make future research in which a control group of inmates is included to minimize the biased effect of the sample and so the results become widespread.
FundingThis work was partially supported by PAPIITIN305313, “Conducta violenta y sus bases biológicas: neuroimagen, neuropsicología y electrofisiología”.
Conflict of interestThe authors declare that they have no conflict of interests.
This work was partially supported by PAPIIT IN305313, “Conductaviolenta y sus bases biológicas: neuroimagen, neuropsicología y electrofisiología” project. Genotyping analyses were done at Instituto Nacional de Psiquiatría Ramón de la Fuente. The authors are grateful to Dra. Alicia Vélez for contacting the University that collaborate in this study. They are also grateful to all the authorities and undergraduates from the University as well as to all the collaborators and advisors in this study.