





Pigmented iris epithelial cysts are the most common type of iris cysts. Generally they are located behind the iris and they have a benign clinical course. A complete ring cyst of the pigmented iris epithelium is an extremely rare entity. We report such a case in a Mexican patient that caused acute secondary angle-closure glaucoma as the main clinical feature. Ultrasound biomicros-copy (UBM) imaging was used for diagnosis and to guide management. Nd:YAG laser iridotomies were performed to successfully break the acute attack of angle-closure glaucoma. Follow-up over 18-months was documented and revealed long-term success of our therapeutic approach.
Los quistes del epitelio pigmentado del iris, son los tipos más comunes de quistes. Generalmente están localizados por detrás del iris y tienen un curso clínico benigno. Un quiste en anillo completo del epitelio pigmentado del iris, es una entidad en extremo rara. Nosotros reportamos un caso clínico con este diagnóstico, en un paciente mexicano, el cual tuvo como manifestación clínica un glaucoma agudo de ángulo cerrado. Se utilizó una ultrabiomicroscopía para realizar el diagnóstico y observar la extensión del tumor iridiano. El diagnóstico diferencial más importante a considerar para este tumor pigmentado es el melanoma. Se realizaron iridotomías Nd:YAG para romper el ataque agudo de glaucoma, causado por la ruptura del quiste. El seguimiento se realizó por 18 meses y las iridotomías se han mantenido eficaces a lo largo del tiempo.
Introduction
A primary cyst of the iris is defined as an epithelial-lined space which involves a portion of the iris and has no recognizable etiology.1 Most of these cysts are derived from the pigment epithelium and are localized to the ciliary sulcus.2 Shields and colleagues have classified primary cysts of the iris pigment epithelium as central (at the pupil margin), midzonal, peripheral (iridociliary) and dislodged (free-floating anterior chamber or vitreous cysts).1 A complete ring cyst of the iris epithelium is extremely rare and is formed when an abnormal membranous sac arises from the posterior aspect of the iris. The wall is composed of iris pigment epithelium and the cavity contains clear serous fluid in a single confluent space extending for 360° around the pupil.3
Case report
A 48-year old Mexican male presented with sudden onset of a red painful left eye with gradual decrease in vision over two days. The patient's medical history was otherwise unremarkable.
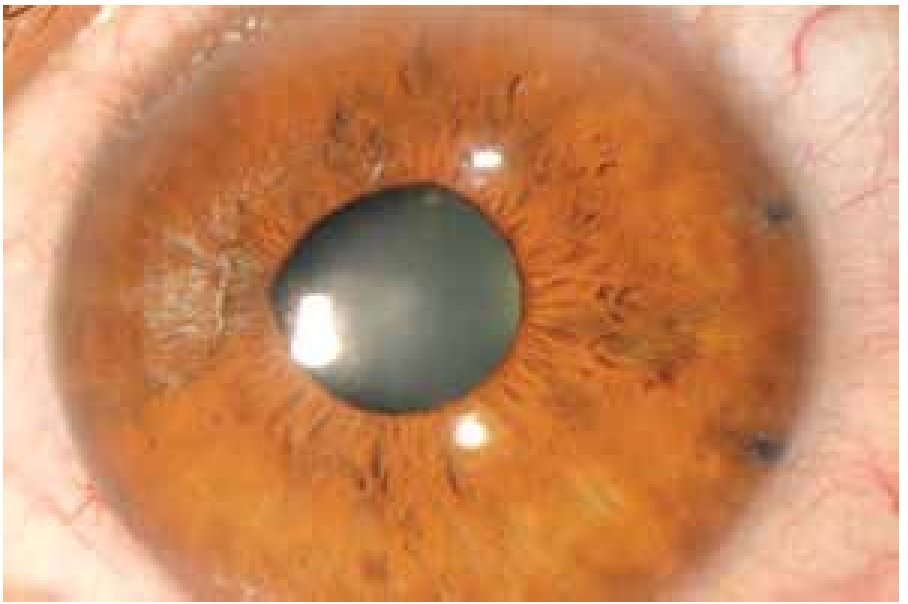
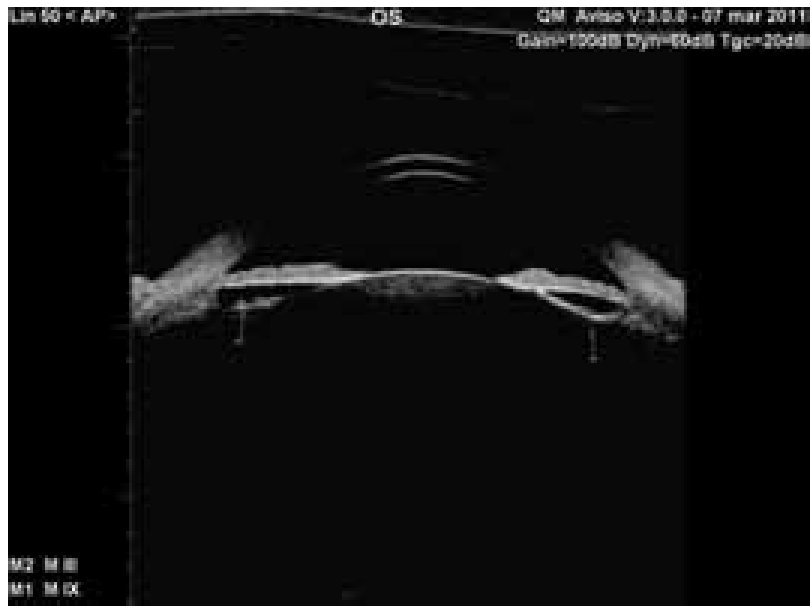
Best corrected visual acuity in the left eye was counting fingers at 1 meter. Intraocular pressure (IOP) was recorded at 63 mmHg by Goldmann applanation. On slit lamp examination, we noted conjunctival hyperemia with ciliary injection, clear cornea and shall owing of the anterior chamber with a mild dilated pupil. A pigmented mass was noted through the pupil behind the iris at the 9-o'clock (Figure 1). The optic nerve cup-to-disc ratio was 0.4 with healthy appearing neuroretinal rim. Ultrasound biomicroscopy (UBM) imaging of the left eye revealed iris thickening associated with a cystic lesion extending 360° on the posterior surface of the iris (Figure 2). The anterior chamber depth was 2.89 mm with a completely closed angle for 360 degrees. These findings suggested angle-closure glaucoma secondary to a complete ring cyst of the iris pigment epithelium. The right eye exam was completely normal.

Figure 1. Anterior segment before treatment.

Figure 2. UBM before treatment.
As initial treatment, the patient received topical and oral ocular hypotensive therapy (Acetazolamide 125 mg PO QID and a fixed combination of Brimonidine, Timolol and Dorzolamide BID topically), which lowered IOP to 32 mmHg. Subsequently, we performed Nd:YAG laser iridotomies at 2 and 4-o'clock targeting the peripheral third of the iris (Figure 3) to achieve cyst rupture. Immediately after the laser treatement was completed, the IOP decreased to 8 mmHg. Pinhole Snellen visual acuity at distance improved to 20/40. Follow-up UBM imaging demonstrated slight deepening of the anterior chamber (2.94 mm) and angle opening for 360° after treatment. We observed a loss of continuity of the iris epithelium at the site of the peripheral iridotomies near the iris root (Figure 4). A repeat UBM was performed eighteen months after treatment (Figures 5 and 6). A large posterior iris cyst was still noted without signs of angle closure or anterior chamber narrowing. Best corrected visual acuity was 20/20, intraocular pressure was 14 mmHg without use of medications and the optic nerve remained free of pathology.

Figure 3. Neodinium: YAG iridotomies at 2 and 4 o'clock meridians.

Figure 4. UBM right after treatment.
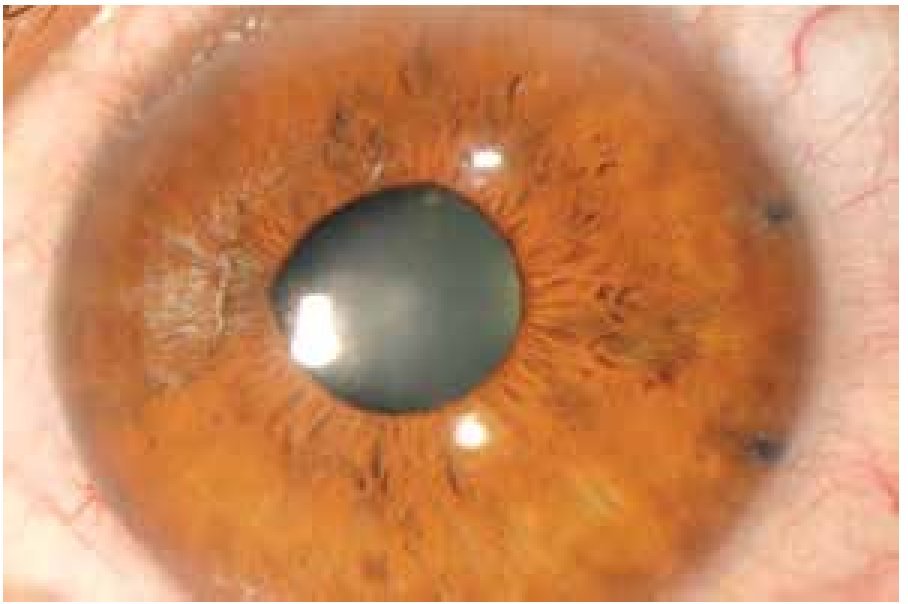
Figure 5. Eye 18 months after treatment.
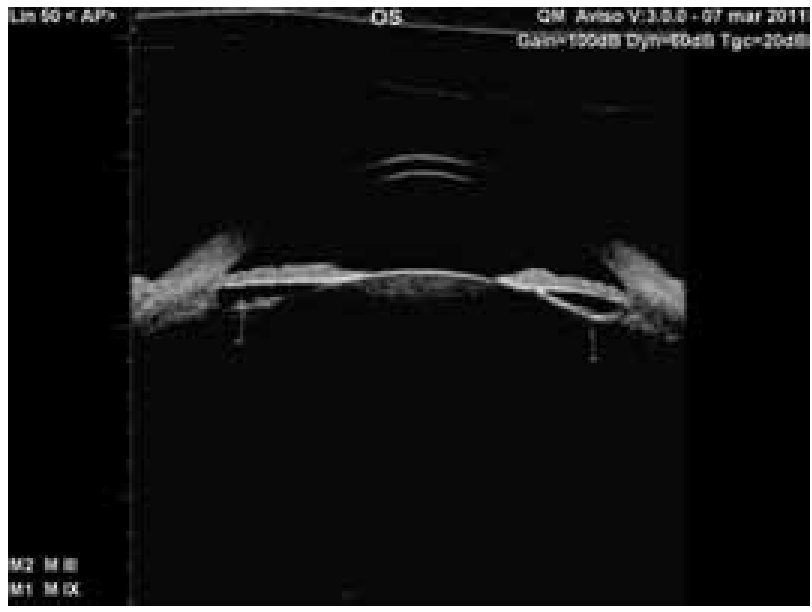
Figure 6. UBM 18 months after treatment.
Discussion
Primary cysts of the iris pigment epithelium are rare developmental anomalies resulting from cystic expansion of the potential space between the pigment epithelial layers of the posterior iris. They are fluid-filled structures lined by cells of neuroectodermal origin, which occur along the posterior surface of the iris, anywhere from the pupilary margin to the anterior ciliary body.3
Some of the typical "primary" epithelial cysts may be acquired as a result of local ocular events; they have been described to arise in aphakes, in response to topical administration of ecothipate iodide and prostaglandin analogs, and trauma. The most common reason for such cystic formations is a history of intraocular surgery and inflammation.4,5 The current case history did not include any of these common associations and the true reason behind the cystic formation remains unknown.
A literature review reviewed only two cases of a ring cyst of the iris epithelium. Like our case, the clinical presentation in one patient was an episode of angle-closure glaucoma treated with a Nd:YAG laser peripheral iridotomy leading to resolution of symptoms.5 The second patient had dull eye pain of three weeks duration and an ocular history of intracapsular cataract extraction with visual acuity of no light perception.4 The differential diagnosis of focal anterior bulging of the peripheral iris includes any solid or cystic tumor of the iris, ciliary body, or both. Differentiation of such lesions is facilitated by echography.3 In this case, the main differential diagnosis for a complete ring cyst of the iris pigment epithelium includes ring melanoma of the iris and multifocal abutting cysts of the iris pigment epithelium simulating a confluent ring cyst.4
Clinical features that should raise the suspicion of iris or ciliary body melanoma include a variably pigmented lesion arising from within the iris stroma, abnormal or prominent vasculature within the lesion, and failure of the lesion to transilluminate. With melanoma, the iris stroma is replaced by the malignancy, rather than stretched over the lesion as with primary iris pigment epithelial cysts.2 UBM is an important tool for assessing anterior segment tumors. The UBM features of a primary neuroepithelial cyst include a highly reflective, smooth cyst wall < 0.2mm thick; an anechoic center and no evidence of a solid component. On the other hand, an iris melanoma appears as a solid irregular iris mass with variable internal reflectivity, distortion of surrounding structures and irregularity or convex bowing of posterior iris plane. If there were multifocal abutting cysts of the iris pigment epithelium extending 360° around the pupil, UBM confirms multiple discrete cysts in such cases.4 Ocular complications due to the presence of iris cysts are uncommon. They typically exhibit limited and slow growth and frequently undergo spontaneous involution.3 But in rare instances, the cysts can cause acute secondary angle-closure glaucoma as highlighted in this case report.2
Conclusion
Iris ring cysts are a very rare condition to the best of our knowledge and after performing an exhaustive search in PubMed-MEDLINE, there are only three other cases reported in the literature. This diagnosis is one to have in mind when unilateral acute angle closure glaucoma is present without pupillary block. A careful slit lamp examination and gonioscopy with the complement of ultrabiomicroscopy are needed to perform a correct diagnosis and determine the localization and extention of the cyst. Once we have a correct diagnosis we will be able to decide which the best treatment option is. In the present case Nd:YAG laser iridotomies were performed which drained the cyst fluid, flatened the iris, opened the angle, lowered the intraocular pressure and also improved the visual accuity; both IOP and visual accuity returned to normal and fortunately due to prompt and correct diagnosis and treatment, the optic nerve remained undamaged. It is important a close clinical follow-up, including ultrabiomicroscopy to detect changes if present in the clinical course.
Conflict of Interest Statement
The authors declare that there is no conflict of interest.
Financial Support
There was no financial support involved in relation to this article.
Acknowledgements
UBM Performed by Mariana Mayorquin-Ruiz and Edurado Moragrega- Adame.
Corresponding author:
Mauricio Turati, MD.
Vicente García Torres N° 46, San Lucas Coyoacán,Z.P. 04030, Mexico City, Mexico.
Phone number: 1084 1400.
E-mail: mturati@gmail.com
