








It is a challenge for the orthodontist to correct bilateral posterior telescopic cross bites, which are a rare but difficult to correct condition. In most of the patients with this kind of cross bite, the upper teeth erupt beyond their lower antagonists thus creating severe occlusal difficulties. The case hereby presented illustrates a way to correct a bilateral posterior telescopic cross bite with a TMA Goshgarian palatal arch and the aid of posterior bite turbos.
Es todo un reto para el ortodoncista el corregir mordidas cruzadas telescópicas posteriores, las cuales llegan a ser poco frecuentes, pero complicadas en su corrección. En la mayoría de los pacientes con mordidas cruzadas de este tipo, los dientes superiores erupcionan más allá de sus antagonistas inferiores, creando graves dificultades oclusales. En el siguiente caso se da a conocer una forma de corregir este tipo de mordidas cruzadas posteriores telescópicas con el uso de una barra palatina de TMA Goshgarian y la ayuda de topes oclusales.
Posterior labial crossbites, Brodie bites, scissor crossbites or telescopic bites are a rare condition but when present, they prove to be extremely difficult to correct. In most patients with telescopic crossbites, the upper teeth erupt more labially than their lower antagonists thus creating serious occlusal difficulties. This kind of bite is characterized by an alteration in the transverse normal relationship between the upper and lower arches.1,2
This condition may be associated with a skeletal compromise or it may occur due to abnormal dentoalveolar inclinations. Posterior cross bites may involve one, several or all posterior teeth, unilaterally or bilaterally. There are different methods for correcting this kind of telescopic crossbites among which is the Goshgarian palatal bar.
The Goshgarian palatal bar was developed in the 1950s by Dr. Goshgarian who combined in its design a passive anchorage resistance that maintains the position of first or second molars and an active anchorage since it also allows movement of such molars. This palatal bar crosses the palate from molar to molar with an open omega bend at the midline.1–3
The Goshgarian bar is usually made of stainless steel round wire but it may also use TMA (titaniummolybdenum and beta-titanium alloys) for its confection. Beta-titanium alloys were first used in 1980 in orthodontics since it has with a higher elasticity module than that of stainless steel thus offering moderate force levels; it is highly malleable and flexible for torque bends and facilitates movements with moderate forces.1,3,4
The Goshgarian bar is indicated in cases of any age either with unilateral or bilateral crossbite as well as in cases with molar rotation. Its use is also indicated for anchorage, bucco-lingual control and for upper molar expansion or narrowing if necessary to achieve labial root torque. In addition, it provides vertical control to counteract the excessive extrusion that occurs in certain cases and enables intrusion if necessary.1–3
In telescopic crossbite correction of the second molars, a treatment alternative may the placement of a Goshgarian palatal bar. For this treatment it is necessary to open the bite by placing bite turbos in the palatal cusps of the first upper molars to allow free movement of the maxillary second molars.5,7
CASE REPORTA male patient, 25 of age was referred to the Orthodontics Clinic at the Division of Postgraduate Studies and Research of the Faculty of Odontology of UNAM because he presented mild upper and lower moderate dental crowding as well as a telescopic crossbite of the second molars. Upon completion of the clinical chart it was determined that the patient was apparently healthy. No pathologic data was found when performing the intraoral assessment; pain or any symptom of temporomandibular joint disorders was not observed. The patient said he was constantly biting his cheek.
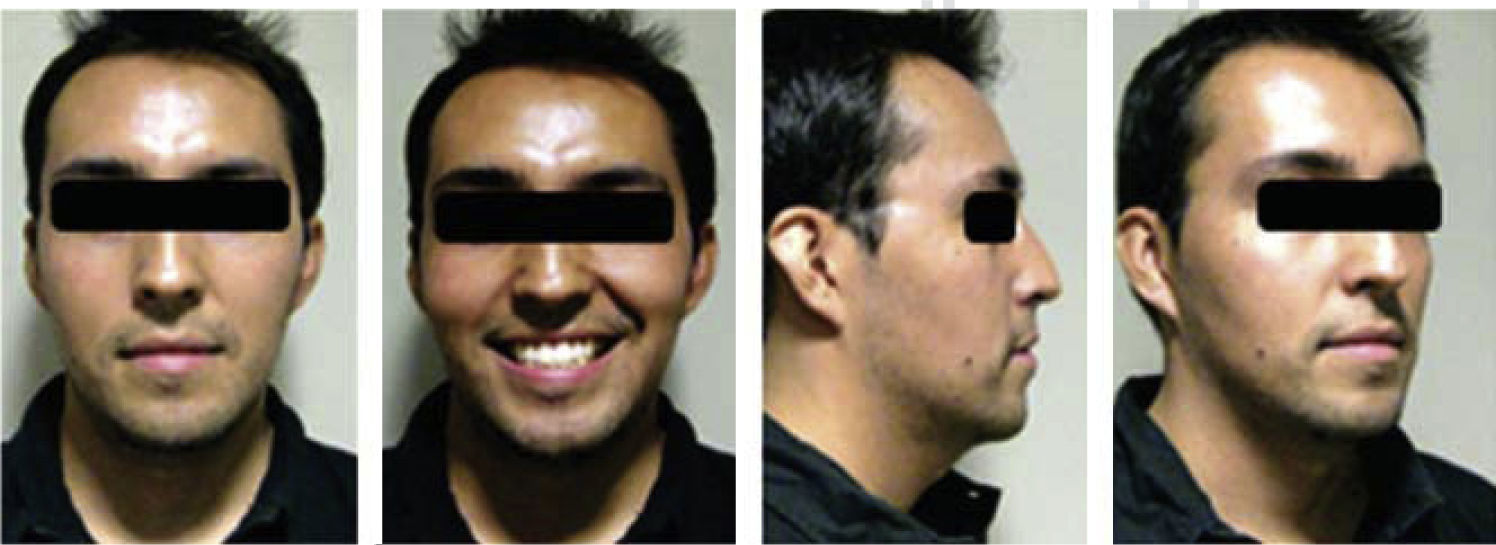
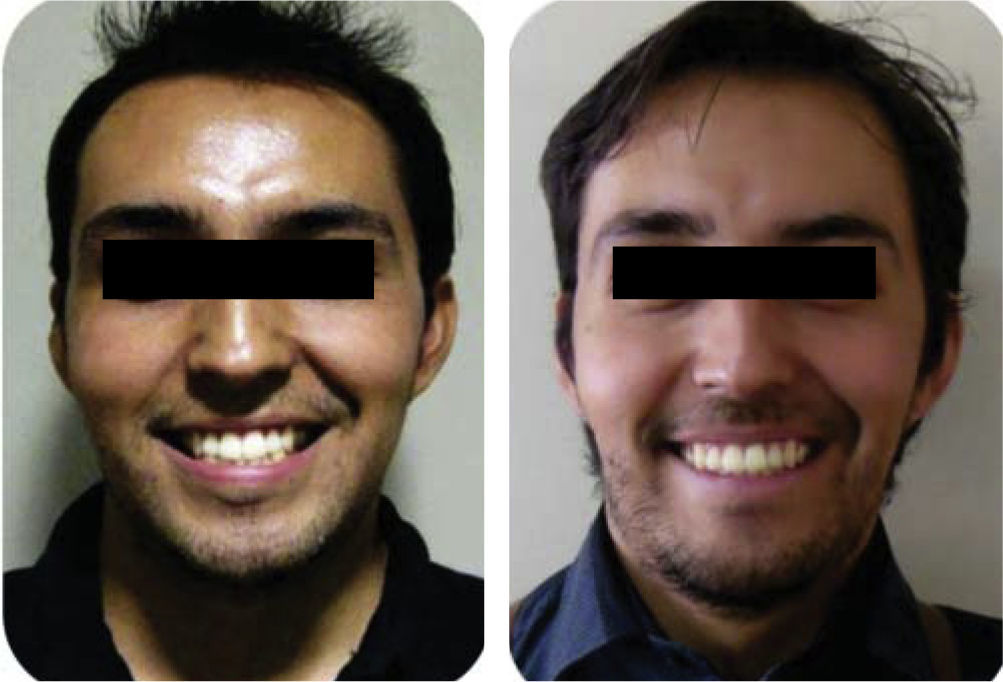
Extraoral photograph analysis revealed a mild dolichofacial patient with an oval-shaped face, straight profile and gibbous nose; thin, competent lips, positive smile and a facial midline that did not coincide with the dental midline (Figure 1).

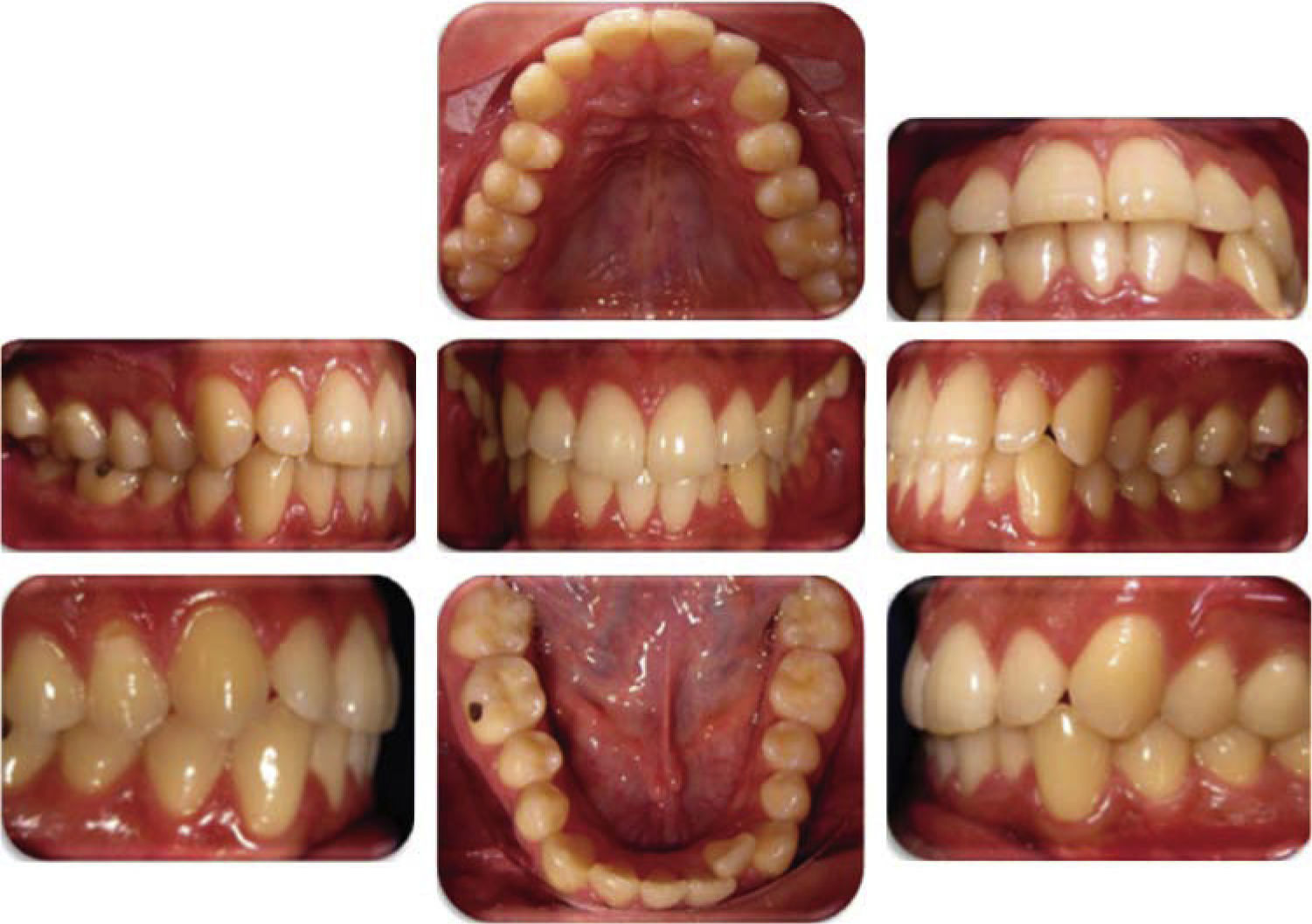
Upon intraoral clinical examination it was noted: that the upper dental midline was deviated to the right and the lower, to the left; a mild upper dental crowding and moderate lower dental crowding, labially inclined upper second molars, lingually positioned lower second molars, bilateral molar class III and canine class I; 2mm overbite and 1.5mm overjet and curve of Spee of 3.5mm on both sides (Figure 2).

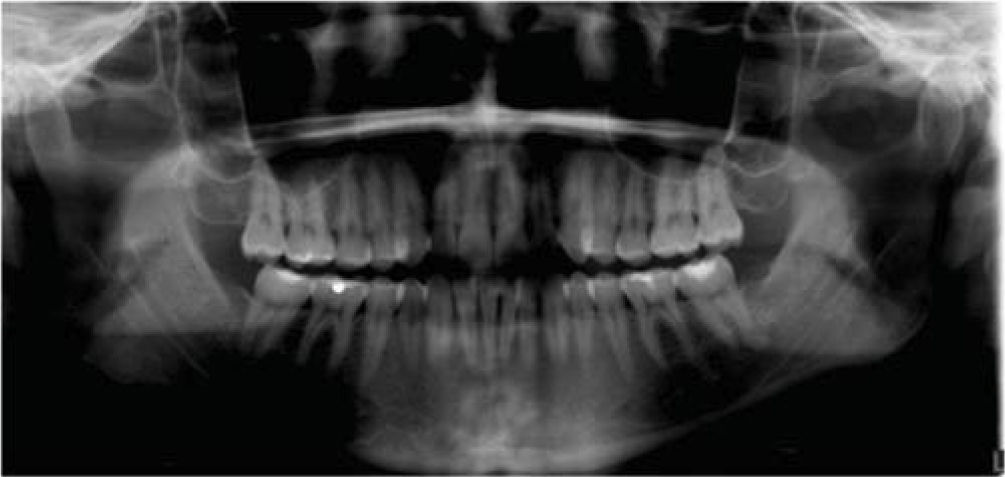
The orthopantomography revealed that the condyles and mandibular ramus were asymmetrical, maxillary sinuses were permeable; 28 teeth, restorations teeth #16, 36, 37, 46, 47, absence of radicular parallelism, mild loss of the alveolar crests and a crown-root ratio of 1:2 (Figure 3).

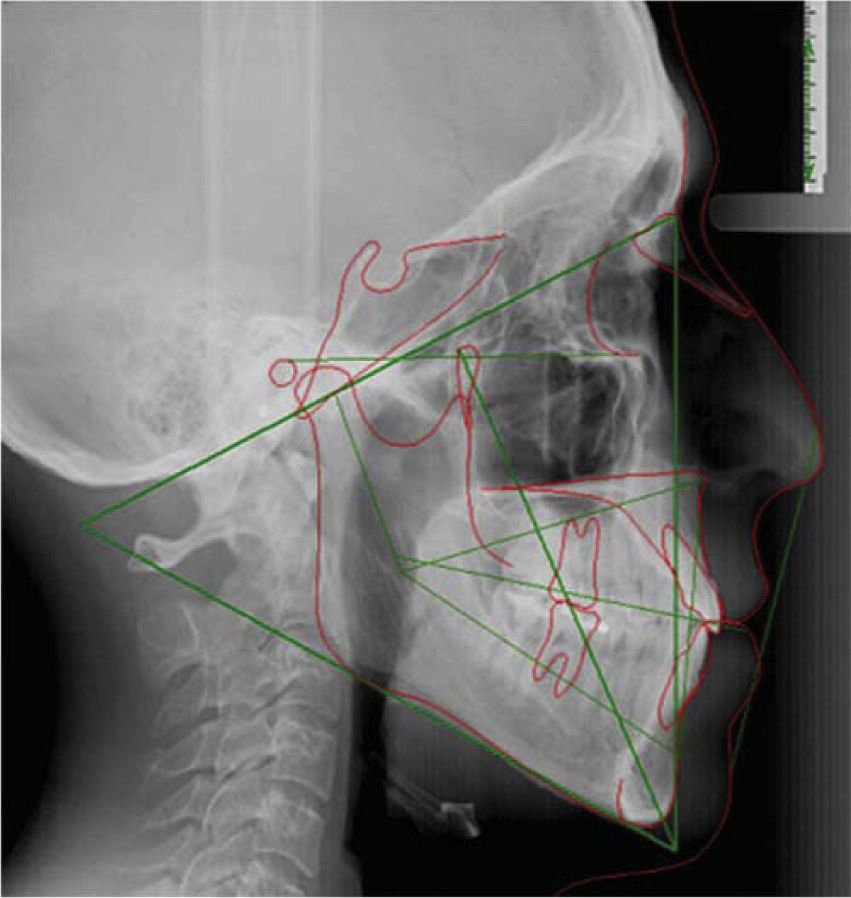
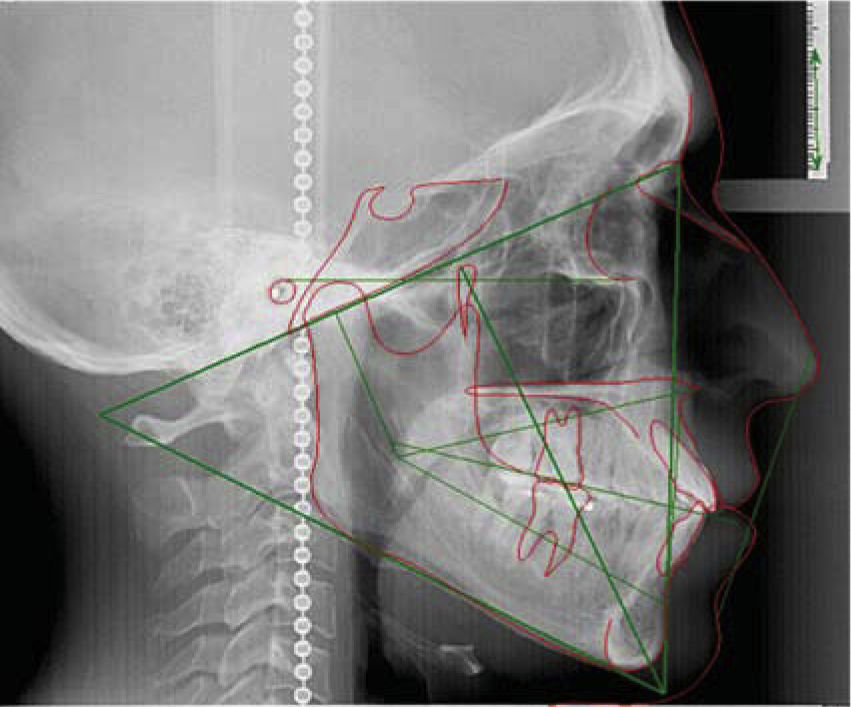
Cephalometric data revealed a skeletal class I with a soft dolichofacial growth direction, upper incisor protrusion and normally inclined incisors (Figure 4).

In accordance with the diagnosis, the following treatment goals were established: to obtain bilateral molar class I, bilateral canine class I, maintain overbite and overjet, align teeth, correct the crossbite of teeth No. 17, 27, 37 and 47; to correct midline deviation and decrease the curve of Spee.
Treatment planTwo treatment options were suggested to the patient. One of them involved using 0.022” x 0.025” Roth GAC In-Ovation®R self-ligating appliances and 2 mini-implants, either with or without corticotomies. The second treatment option was 0.022” Roth GAC In-Ovation®R appliances and for the correction of the upper second molars, a 0.036” TMA removable palatal bar. The patient did not accept the mini-implants or the corticotomies, so the second option was chosen.
Treatment progressBefore orthodontic treatment was initiated an informed consent was signed. Self-ligating 0.022” In- Ovation®R Roth fixed appliances were placed with bands in the upper and lower first molars. 0.014” NiTi round archwires were used in the upper arch and 0.012” NiTi in the lower arch. After three months of leveling 0.022 Roth tubes were placed in the lower second molars and bands with lingual boxes in the upper second molars for placing the 0.036” TMA palatal bar. Glass ionomer bite turbos were placed in the palatal cusps of the first molars in order to open the bite and allow the second molars to move. Transverse measurement of these molars was taken and it was 61.5mm.
The patient attended the orthodontics clinic in the course of the same month referring that he had worn down the bite turbos and fractured the palatal bar due to eviction caused by dental contacts resulting from the loss of the bite turbos. Treatment continued by placing again the turbos in the same place but manufacturing them this time with fotocurable resin. A new 0.036” TMA palatine bar was also fabricated (Figure 5). The next step in treatment was the alternate activation on each side of the palatal bar and after eight months of activation we managed to bring the second molars into their basal arch obtaining a 54mm transverse distance. At the same time, the archwire sequence indicated by Roth philosophy was followed in both arches until the final stage of treatment was completed with 0.019” x 0.025” stainless steel archwires and a transverse measurement of the upper and lower second molars of 50mm. The use of ¼ inch and 3.5 oz class III elastics was instructed for a better intermaxillary relationship (Figure 6). An adequate occlusion of the second molars and of the rest of the teeth was maintained and the appliances were removed. Retention consisted in the placement of a lower fixed retainer from canine to canine and an upper circumferential retainer with acrylic in the labial surface of the incisors (Figure 7).
RESULTS


Extraoral photographs: in the smile photographs, a change in tooth display was observed and buccal corridors were improved. The dental midline deviation was centered with the facial midline and crowding was corrected while maintaining the profile and improving the nasolabial angle which decreased 10° (Figure 8).

Intraoral photographs: the goals set at the beginning of treatment were accomplished. The upper and lower arches were aligned, the initial overjet and overbite was maintained, molar class I was achieved and the canine class I remained. The telescopic posterior crossbite was corrected (Figures 9 and 10).


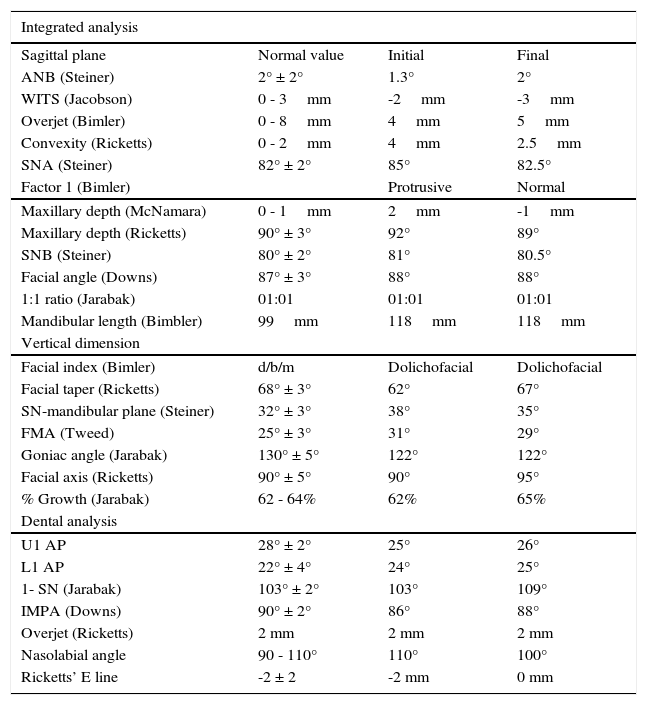
Cephalometric analysis: there were no significant changes regarding the maxillomandibular relationship. The skeletal class I remained only improving the ANB angle and Ricketts’ convexity. In the vertical plane, there was a change in the vertical dimension due to the transverse correction of the second molars which were in telescopic bite. Dental analysis revealed an increase in upper and lower proclination but still within normal values and in the soft tissue, an improvement was noted in the nasolabial angle which decreased 10o(Figures 11 and 12, Table I).


Integrated cephalometric analysis: initial and final values.
| Integrated analysis | |||
|---|---|---|---|
| Sagittal plane | Normal value | Initial | Final |
| ANB (Steiner) | 2° ± 2° | 1.3° | 2° |
| WITS (Jacobson) | 0 - 3mm | -2mm | -3mm |
| Overjet (Bimler) | 0 - 8mm | 4mm | 5mm |
| Convexity (Ricketts) | 0 - 2mm | 4mm | 2.5mm |
| SNA (Steiner) | 82° ± 2° | 85° | 82.5° |
| Factor 1 (Bimler) | Protrusive | Normal | |
| Maxillary depth (McNamara) | 0 - 1mm | 2mm | -1mm |
| Maxillary depth (Ricketts) | 90° ± 3° | 92° | 89° |
| SNB (Steiner) | 80° ± 2° | 81° | 80.5° |
| Facial angle (Downs) | 87° ± 3° | 88° | 88° |
| 1:1 ratio (Jarabak) | 01:01 | 01:01 | 01:01 |
| Mandibular length (Bimbler) | 99mm | 118mm | 118mm |
| Vertical dimension | |||
| Facial index (Bimler) | d/b/m | Dolichofacial | Dolichofacial |
| Facial taper (Ricketts) | 68° ± 3° | 62° | 67° |
| SN-mandibular plane (Steiner) | 32° ± 3° | 38° | 35° |
| FMA (Tweed) | 25° ± 3° | 31° | 29° |
| Goniac angle (Jarabak) | 130° ± 5° | 122° | 122° |
| Facial axis (Ricketts) | 90° ± 5° | 90° | 95° |
| % Growth (Jarabak) | 62 - 64% | 62% | 65% |
| Dental analysis | |||
| U1 AP | 28° ± 2° | 25° | 26° |
| L1 AP | 22° ± 4° | 24° | 25° |
| 1- SN (Jarabak) | 103° ± 2° | 103° | 109° |
| IMPA (Downs) | 90° ± 2° | 86° | 88° |
| Overjet (Ricketts) | 2 mm | 2 mm | 2 mm |
| Nasolabial angle | 90 - 110° | 110° | 100° |
| Ricketts’ E line | -2 ± 2 | -2 mm | 0 mm |
Telescopic bites or Brodie bites are rare but difficult to correct. In the majority of patients with telescopic crossbites, the upper teeth erupt in a mostly labial direction in comparison with their antagonists thus creating serious occlusal problems. This kind of bites are characterized by an alteration in the transverse relationship between the upper and lower arches.1,2
It is important to consider that in order to correct this anomaly it will be necessary to open the bite to allow free movement of the teeth in crossbite. This may be performed with a removable bite plane and the patient's full cooperation, or with bite turbos or occlusal pads placed in the palatal cusps of the upper molars. The latter option has the advantage of being stable and that it allows movement of the teeth in crossbite without any occlusal interference which may cause bracket fracture or debonding.2,5,6
Among the palatal Goshgarian bars advantages are: simple design, easy placement and removal, low cost; versatility for solving various molar problems such as rotation, extrusion, overexpansion, torque, distalization and anchorage.4
In a study conducted by Gunduz and Harrison the palatal bar effectiveness for correcting molar rotation and achieving maxillary expansion was demonstrated.8,9 Hoederath stated that the palatal bar may be used passively for anchorage as well as actively in order to achieve dental movements of first, second and third order; additionally it provides expansion and compression, distal rotation, unilateral distal tipping and root torque.10 The palatal bar may also be used to correct unilateral crossbites through the application of labial root torque to the anchorage molar and lingual root torque to the contralateral crossbite molar, combined with expansion or compression.11
CONCLUSIONSOrthodontic treatment improves occlusal function and aesthetics, prevents future periodontal problems and brings teeth to their ideal positions through the use of proper appliances. In the present case, the TMA palatal bar allowed us to obtain adequate torque and tipping of the second molars thus proving to be an excellent and economic alternative for telescopic crossbite correction.
The Goshgarian palatal bar has many advantages during orthodontic treatment. In addition to actively moving teeth individually, it is an element of easy construction and manipulation for the orthodontist; likewise, it is comfortable and aesthetic for the patient. The Goshgarian palatal bar is a versatile appliance that provides quick and excellent results through its multiple uses and combinations.
Graduate of the Orthodontics Department.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia