


A transversal descriptive study was conducted at the Stomatology Department of the Mexico Children’s Hospital «Dr. Federico Gomez» to determine if there is a relationship between maturational indicators according to Bjork in hand- wrist radiographs and cervical vertebrae indicators according to Lamparski. The total sample size was 213 patients, 105 females and 108 males, all were healthy and between the ages of 6 and 17 years old. Lateral head films and hand wrist radiographs were taken from each patient. A statistical analysis was applied for ordinal data. In general 66.61% of the females had similarities between hand wrist and cervical vertebrae and 57.3% of the males. The correlation index was 0.727 for females and 0.686 for females.
Se hizo un estudio descriptivo, comparativo y transversal en el Departamento de Estomatología del Hospital Infantil de México «Federico Gómez» para determinar si existe relación entre los estadios carpales de Bjork con los estadios de las vértebras cervicales según Lamparski. La muestra total fue de 213 pacientes, 105 mujeres y 108 hombres, todos fueron pacientes sanos entre los 6 y 17 años de edad. Se seleccionaron y analizaron las radiografías laterales de cráneo y carpales tomadas de los expedientes de los pacientes incluidos en la muestra. Se realizó un análisis estadístico para datos ordinales. En general encontramos 66.61% de correlación para el sexo femenino y para el sexo masculino coinciden el 57.3% de los casos. El coeficiente de correlación fue de 0.727 para el sexo masculino y de 0.686 para el femenino.
Growth is a process of dynamic changes which are valuable to the dentofacial management in benefit of the patient.1 The growth rates of the skeletal system suffer variation during childhood and adolescence. Each individual is characterized by having their own pace of growth. Some present their pace of growth more quickly, others more slowly and the rest, at a pace that could be called intermediate.2,3
The significant increase in speed of growth in puberty is subjected to a complex endocrine control. In the hypothalamus the secretion of the releasing factors begins, which reach to the pituitary gland. In the anterior lobe of the pituitary gland, the hypothalamic releasing factors stimulate the pituitary cells to produce various hormones called pituitary gonadotropins, whose function is to stimulate endocrine cells of the sexual organs in development phase to produce sexual hormones.2
In males testicular cells produce testosterone (male hormone) and female hormones. In women, pituitary gonadotropins stimulate the secretion of estrogen in the ovaries and afterwards, progesterone. Under the stimulus of pituitary gonadotropins testicular, ovarian adrenal cortical sex hormones pass to the blood circulation in sufficient quantities to induce the development of secondary sexual characteristics and accelerate the overall body growth and the decline of the lymphoid tissues observed during growth.2
Sex hormones have a double influence on the growth of the endochondral bone. First of all, sex hormones stimulate cartilage to grow faster, giving rise to the pubertal growth spurt. However, these hormones also accelerate the pace of skeletal maturation that in the long bones corresponds to the pace at which the cartilage is converted into bone. The acceleration of maturation is even greater than that of growth.
Therefore, during the growth spurt of adolescence, more cartilage is consumed than what is replaced. Towards the end of adolescence, what is left of cartilage is converted into bone and the epiphyseal plates close. At that time, the potential for grow this lost and the individual ceases to grow. The growth plates that involve sexual maturity are also more complete in girls.2
Pituitary gonadotropin stimulates the gonads to perform the final maturation of the reproductive tract. This period of growth and maturation is called puberty. Puberty strictly defined is the period in which the endocrine and gametogenic functions of the gonads have arrived for the first time to the point of making reproduction possible. In girls, the first phenomenon is the thelarche, the development of mammary glands, followed by the pubarche, the development of pubic hair, and later, the menarche. The first menstrual period is an excellent indicator for the onset of sexual maturity. Sexual maturity is accompanied by an acceleration of growth.2
In children ages 7 to 10, a slow increase in the secretion of estrogens and androgens precedes a more rapid increase in the early years of the adolescence. In recent years in the United States’ population puberty appears between 8 and 13 years in girls and between 9 and 14 in boys.4 Ruiz in a study conducted at the Mexico Children’s Hospital «Dr. Federico Gomez», found that the peak of growth in children is 13.27 years and that in girls is 11.33 years.1
In sexual development, puberty is a combination of morphological and physiological changes that occur in children during the period of testicular maturation and growth of the penis in males and ovaries in women. Menarche, unlike the outbreak of growth and breast development, is often a late event during puberty. Menarche almost always happens after the peak of growth, therefore if it is known that when a girl reaches menarche, it is possible to assume with enough certainty that she leaves behind her maximum growth speed and that it will be slower.1,5
The maturation process can be affected by genetic, hormonal, nutritional and pathological factors. The degree of alteration that nutrition and pathologies cause on the maturation and physical growth will depend on the duration, intensity and time of occurrence.6
Marshall and Tanner have shown that none of the physical changes related to gender shows a relationship with the appearance of the peak of growth. Therefore knowing the stage of development of any of these sexual characteristics does not enable us to accurately predict the maturation stage.1,3,6,7
Haag and Taranger created a method using a hand and wrist radiograph to determine the correlation of the maturation indicators in pubertal growth acceleration.8
Several bone events have been related to the peak of growth. One of these events is the appearance of the sesamoid bone, which has been regarded as a signal for pubertal growth. Flory in 1936 indicated that the sesamoid bone calcification is a good guide for determining the period immediately prior to puberty. Some authors suggest that the peak of speed in height occurs one year after the calcification of the sesamoid bones.3,9-12
When planning the orthodontic treatment, it is important to know how much remains of skeletal growth, so it is often necessary to assess bone age, in order to determine if the treatment is orthopedic (when there is still potential for growth), orthodontic- orthopedic (when there is little growth remaining) or surgical-orthodontic (when there is no growth).2
Skeletal age assessment should be based on the maturation of a series of bone indicators. Although different indicators may be used, the standard reference for assessing skeletal development is the ossification of the hand and wrist bones. An X-ray of the hand and wrist allows visualization of approximately 30 small bones, all with a predictable order of ossification. This order was represented in growth stages that are assessed according to the relation epiphysis-diaphysis. Three different stages are described:
- •
The epiphysis has the same width as the diaphysis.
- •
The diaphysis surrounds the epiphysis as cap.
- •
Ossification of the epiphysis with the diaphysis.
It is more common to determine maturity in hand wrist radiographs and on the lateral head film because these radiographs are easy to take and require a minimum of patient radiation.1,4,9
In 1929, Pyle and Gruelich formulated the first group of maturity indicators using a hand-wrist radiograph.6,9
The appearance of each epiphysis, its increase in size, the degree of remodeling, the obtaining of a mature size and its merger with the corresponding diaphysis are maturity indicators that have been organized and systematized in different methods of bone maturation. Among the more relevant due to its chronologically speaking effectiveness, the following are listed:3,10
- 1)
Fishman developed a system of skeletal maturity indicators on hand and wrist using four stages of bone maturation in six anatomical sites which also includes eleven maturation stages of the carpal bone and showed that the acceleration and deceleration in the rate of craniofacial growth is associated with alterations in the development and maturation.1,9
- 2)
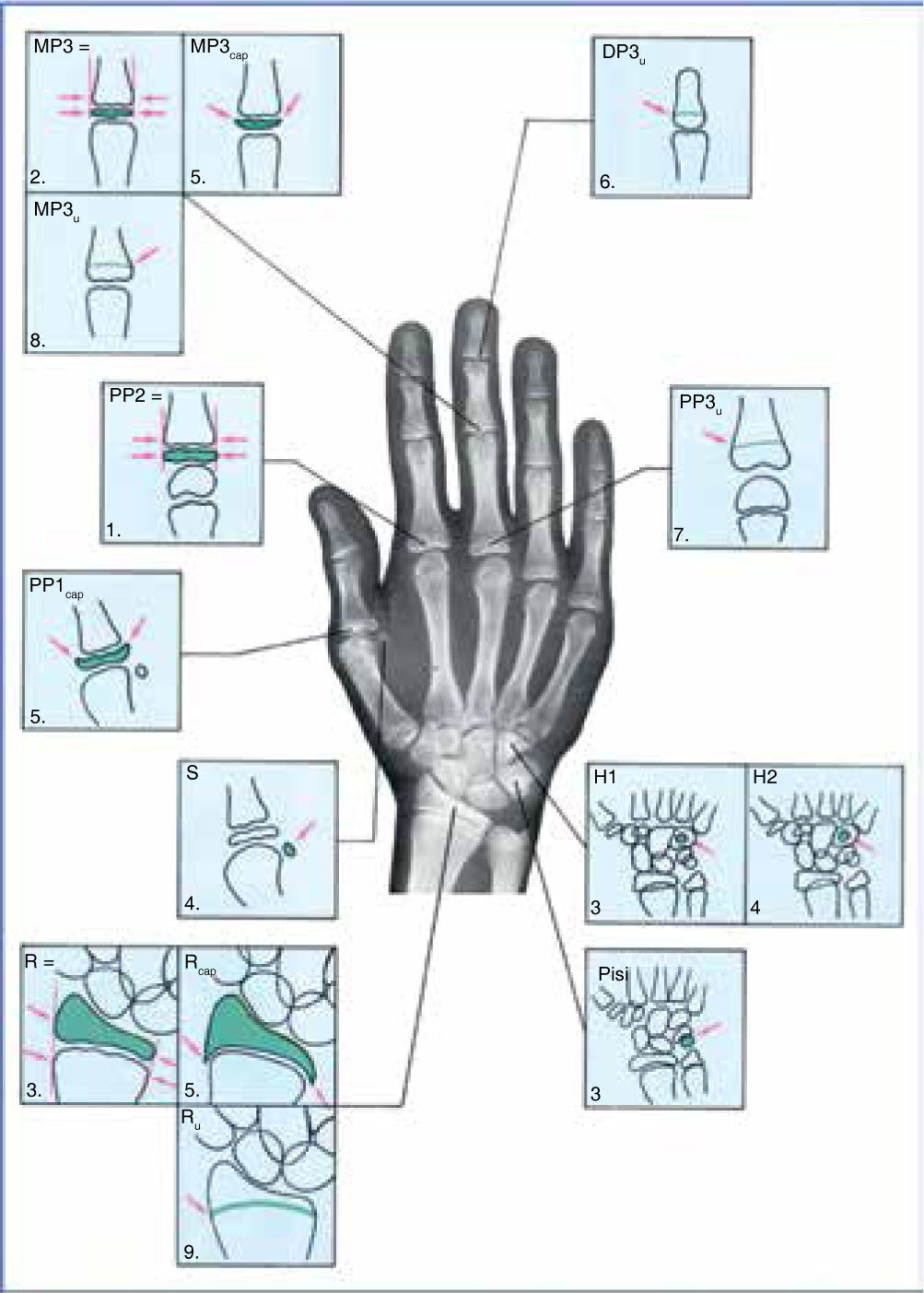
In 1972, Björk divided the process of maturation of carpal bones in nine stages between the ages of 9 to 17 years. The 16 indicators of skeletal maturity according Björk are detected at the fingers (they are assessed according to their relation between the epiphysis and the diaphysis), carpal bones and radius. In the phalanges three signs of ossification are described:
- •
The epiphysis has the same width as the diaphysis.
- •
The diaphysis surrounds the epiphysis as cap.
- •
Ossification of the epiphysis with the diaphysis.
- •
Fingers are described with a number from 1 to 5 starting at the thumb. The Björk analysis divides the process of maturity in nine stages.
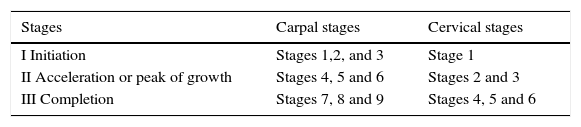
Björk’s analysisBjörk’s nine stages of maturation are divided into three growth intervals (Figure 1):
- I.
Initiation: It comprises the following stages:
- 1.
PP2 (proximal phalanx of the second finger, the epiphysis is equal in width to the diaphysis).
- 2.
MP3 (middle phalanx of the third finger, the epiphysis is equal in width tothediaphysis). dig
- 3.
H-1 (apophysis of the hamate bone (phase 1), Pisi (appearance of the lentiform bone), R (Radius, the epiphysis is equal in width to the dia- physis).
- 1.
- II.
Acceleration (peak of growth): It includes following stages:
- 4.
S (emergence of the sesamoid bones), H-2 (apophysis of the hamate bone (phase 2).
- 5.
MP3 cap (middle phalanx of the third finger, the epiphysis is located in cap in relation to the diaphysis), PP1 cap (proximal phalanx of the first finger, the epiphysis is located in cap in relation to the diaphysis), R cap (Radius, the epiphysis is located in cap in relation to the diaphysis).
- 6.
DP 3U (distal phalanx of the third finger, complete ossification).
- 4.
- III.
Completion: It covers the following stages:
- 7.
PP 3U (middle phalanx of the third finger, complete ossification).
- 8.
MPRU (middle phalanx of the third finger, complete ossification).
- 9.
RU (radius, complete ossification).
- 7.

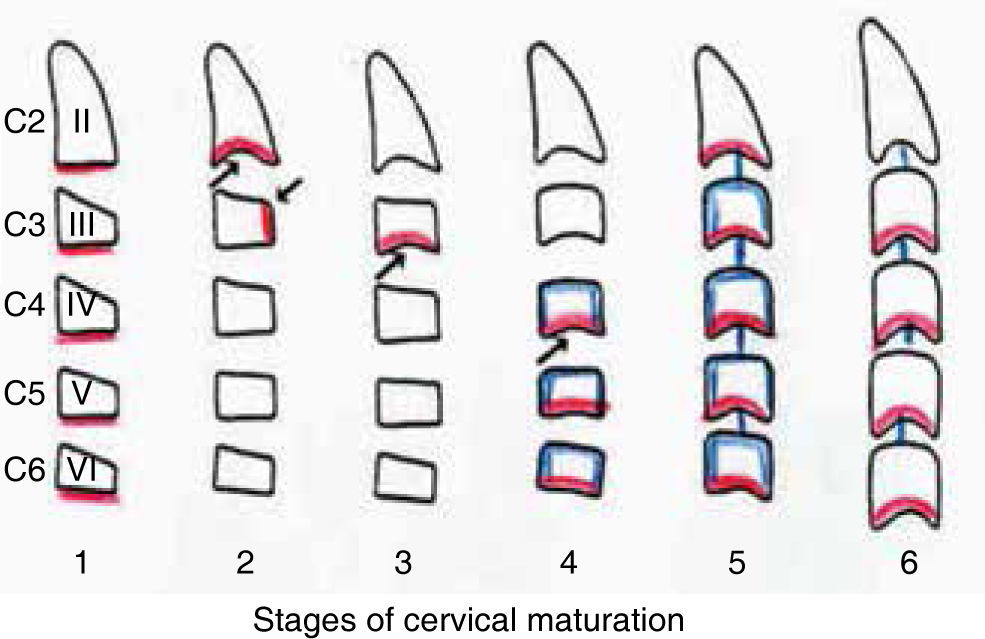
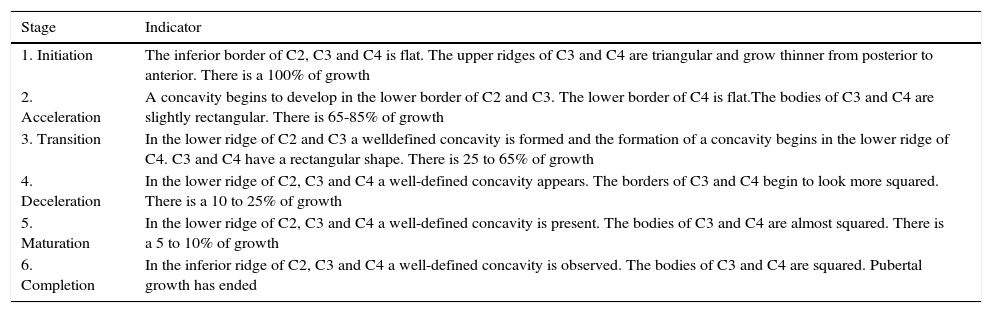
The maturation stages of the cervical vertebrae were described by Lamparski and were modified by Hassel and Farman (Figure 2).13–15

The six stages of maturation of the cervical vertebrae are the following:
| Stage | Indicator |
|---|---|
| 1. Initiation | The inferior border of C2, C3 and C4 is flat. The upper ridges of C3 and C4 are triangular and grow thinner from posterior to anterior. There is a 100% of growth |
| 2. Acceleration | A concavity begins to develop in the lower border of C2 and C3. The lower border of C4 is flat.The bodies of C3 and C4 are slightly rectangular. There is 65-85% of growth |
| 3. Transition | In the lower ridge of C2 and C3 a welldefined concavity is formed and the formation of a concavity begins in the lower ridge of C4. C3 and C4 have a rectangular shape. There is 25 to 65% of growth |
| 4. Deceleration | In the lower ridge of C2, C3 and C4 a well-defined concavity appears. The borders of C3 and C4 begin to look more squared. There is a 10 to 25% of growth |
| 5. Maturation | In the lower ridge of C2, C3 and C4 a well-defined concavity is present. The bodies of C3 and C4 are almost squared. There is a 5 to 10% of growth |
| 6. Completion | In the inferior ridge of C2, C3 and C4 a well-defined concavity is observed. The bodies of C3 and C4 are squared. Pubertal growth has ended |
The population who attends the Department of Stomatology of the Mexico Children’s Hospital ranges from 6 to 17 years of age which means that their treatment may be orthopedic and orthodontic. Such treatment will depend in the first place of the diagnosis which is determined by a set of studies containing the following: study models, intraoral and extraoral photographs, panoramic and lateral head films, and secondly, on the stage of bone maturation. To determine the stage of bone maturity an extra radiograph is required, the carpal radiograph.
In orthodontics it is more common to determine bone maturity on the bones of the hand and wrist through carpal radiographs, where bone maturity is determined in the epiphysis and diaphysis of the bones of the hand and the carpal bones. Maturity is determined with the sequential changes that occur in these structures. Currently, the degree of bone maturity is diagnosed on the cervical vertebrae of the same cephalogram (lateral head film), so it is important to determine the relationship of the size and shape of the cervical vertebrae (C2, C3 and C4) in relation to the Bjork’s maturational stages described in the carpal radiograph, in order to determine the maturation stage and thus avoiding that the patient is radiated again and a greater economic cost.
Growth potential is an important indicator for the orthodontist because it provides valuable information for diagnosis and orthodontic and surgical treatment planning, as well as in the corrections of the orthopedic dentofacial discrepancies. Therefore it is important to take into consideration the stage of bone maturation of each patient.
Materials and methodsAt the Department of Dentistry of the Children’s Hospital of Mexico «Federico Gomez» attend for consultation patients from 6 to 17 years of age. To conform the study sample, records from 1999 to 2003 from patients of both genders and diagnosed as healthy were selected.
The radiographs were obtained according to the following criteria:
- •
The cephalogram and the carpal radiograph should be taken the same day.
- •
Radiographs of patients of both genders between 6 and 16 years of age.
- •
The cervical vertebrae in the cephalograms must clearly be seen.
- •
On carpal radiographs of the left hand the bony structures of hand and carpal should be observed.
- •
Radiographs of patients without any craniofacial syndrome.
- •
- •
Radiographs from patients who received treatment in the Department of Dentistry of the Mexico Children’s Hospital «Dr. Federico Gomez»
- •
Radiographs of patients diagnosed as healthy.
The radiographs that presented one or more of the following features were eliminated from the study according to the following criteria:
- •
Radiographs from patients with congenital or acquired disorders.
- •
Radiographs from patients with abnormalities in cervical vertebrae.
- •
Radiographs from patients with reports of severe trauma in face or hands.
- •
Radiographs from patients with true precocious puberty.
- •
Radiographs from patients with alterations in somatic development.
- •
Radiographs from patients with cleft lip and palate associated or not with syndromes.
All X-rays were taken by the same radiologist technicianandwith thesamemachinewhich belongs to the Department of Stomatology of the Mexico Children’s Hospital «Dr. Federico Gomez» (Cranex TOME multifunctional 3 Ceph, model PT-11 SA/C Soredex).
All the radiographic films were 8 x 10, Agfa brand.
A chassis for radiographic film Kodak brand-X Omatic Cassettes was used. A letter of informed consent was given to the patients’ parents where the name, importance and risk of the study were declared.
The cephalograms and the carpal radiographs of apparently healthy patients of both genders between 6 and 17 years of age who were admitted at the Department of Dentistry of the Mexico Children’s Hospital «Dr. Federico Gomez» during the period 1999 to 2003 were observed.
A record sheet was filled by all patients. The radiographs were labeled by number without specifying age, sex or name. The measurement of the stage of bone maturation in the carpal radiograph was carried out according Bjork’s analysis.
In the cervical vertebrae the measurements were performed according to the analysis of Lamparski on the cephalograms: The measurements were carried out by two orthodontists of the Department of Dentistry of the Mexico Children’s Hospital «Dr. Federico Gomez».
The methods for the identification of carpal bone stages as described by Bjork and the vertebral bones according to Lamparski were given in writing with the following instructions:
The periphery of the cervical vertebrae was observed.
The stage on which the cervical vertebrae were was recorded.
On the carpal radiograph the growth stage was analyzed according to the stages of Bjork and it was also recorded.
A first group of carpal radiographs and cephalograms was given to each of the orthodontists who measured and filed the results.
In the following week another group of radiographs was given to the same orthodontists and the discrepancy with the first group was compared. In the event that major differences exist, a third analysis was made to eliminate bias in the identification of the stages.
The relationship between the size and shape of the cervical vertebrae and the maturational stages was analyzed according to the following table I:
Due to the fact that the study was conducted on radiographs taken to patients routinely for orthodontic treatment and that the radiation exposure was minimal, there was no need for emphasis on this matter.
Statistical analysisThe total of obtained radiographs were 426,213 carpal radiographs and lateral head films. After being analyzed by two orthodontists from the Department of Stomatology at the Mexico Children’s Hospital a comparative analysis was carried out in agreement with table I.
To assess the relationship between the two maturational stages a series of association measures for ordinal data were constructed in order to know not only the intensity but also the direction of such relationship.
The measure for correlation used was gamma because if the relationship between two variables is perfect and positive gamma equals 1. If the relationship between the variables is perfect but negative gamma is equal to -1. If the variables are independent gamma is equals 0. In this case, the relation between vertebral and carpal stages is positive, but it is not perfect because the obtained value is around 0.7, slightly higher for males.
ResultsThe obtained results by maturational analysis were the following:
The gamma correlation coefficient was 0,727 (p < 0.001) for males and 0.0686 (p < 0.001) for females.
DiscussionIn order to provide an ideal diagnosis and orthodontic treatment, it is of the utmost importance to know the patient’s status of bone maturation. In order to know the stage of maturation several studies can be performed in different parts of the body such as shoulder, knee, cervical vertebrae, hip, hand and wrist. The aid of diagnostic tools is necessary to assess biological age, since many times the patient‘s chronological age does not match the osseous age.
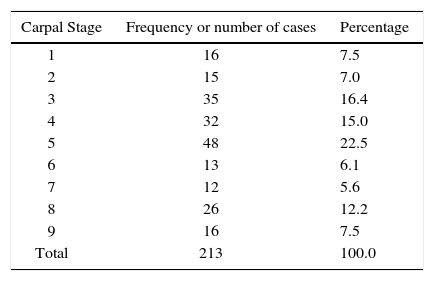
The sample used in this study was grouped by gender and cervical and carpal bone stage. The age range was from 6 to 16 years of biological age so when we look at our data it may be observed that the percentage of relationship presented by each stage varies according to the number of patients in each stage.
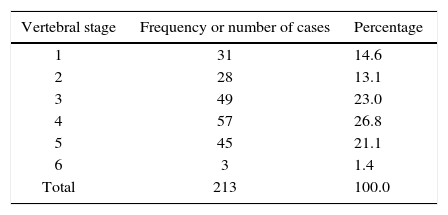
While analyzing the data of both genders, with an average age of the 12.35 for females and 12.42 years for males, the carpal stage that prevailed was stage number five with 22.5%; the cervical stage that prevailed was stage number four with 26.8%. It can be said that 44.13% of the sample is in the acceleration phase of growth, 30.99% is starting growth and 24.88% is in completion stage (Table IIyIII).
Comparing the cervical and carpal stages analyzed, we found that in females, in 66.62% of the cases there is a correlation for both maturational stages and for males, the relation exists in 57.3% of the cases. For the purposes of being able to recommend cervical stage as a 100% reliable maturation sign, it would have been desirable to find an ideally exact relationship stage by stage.
With regard to our study’s research problem, we can state that there is a good relationship between the size and shape of the cervical vertebrae in relation to the carpal stage of bone maturation. It can be declared that the hypothesis has favorable evidence to be accepted.
It was important for our study to ensure that the two radiographs, carpal and cephalogram were taken the same day and by the same radiologist technician.
ConclusionsThe correlation was slightly higher for females. We can assume that this is due to the fact that the males’ sample size was slightly smaller.
Taking into consideration previous research and the results obtained in this study, it can be observed that there is a reliable relation between cervical and carpal stages of maturation (57.3% of reliability for males and 66.6% for females). On this basis the lateral head film may be used as diagnostic means to assess the patient’s maturational stage in order to provide a reliable diagnosis and treatment plan.
Carpal radiographs may be discarded only if a 100% certainty is not required (especially in the stages of initiation and completion of growth).
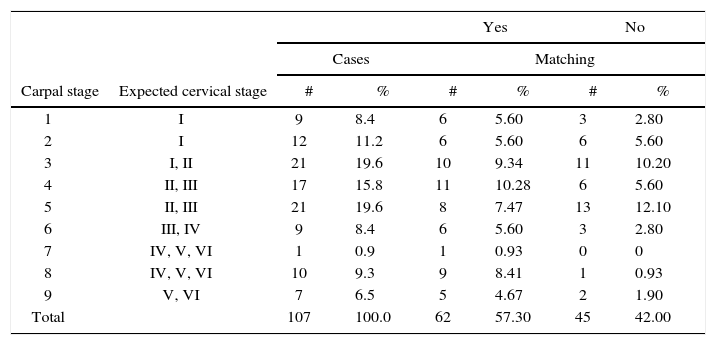
Obtained data from correlation in males.
| Carpal stage | Expected cervical stage | Yes | No | ||||
|---|---|---|---|---|---|---|---|
| Cases | Matching | ||||||
| # | % | # | % | # | % | ||
| 1 | I | 9 | 8.4 | 6 | 5.60 | 3 | 2.80 |
| 2 | I | 12 | 11.2 | 6 | 5.60 | 6 | 5.60 |
| 3 | I, II | 21 | 19.6 | 10 | 9.34 | 11 | 10.20 |
| 4 | II, III | 17 | 15.8 | 11 | 10.28 | 6 | 5.60 |
| 5 | II, III | 21 | 19.6 | 8 | 7.47 | 13 | 12.10 |
| 6 | III, IV | 9 | 8.4 | 6 | 5.60 | 3 | 2.80 |
| 7 | IV, V, VI | 1 | 0.9 | 1 | 0.93 | 0 | 0 |
| 8 | IV, V, VI | 10 | 9.3 | 9 | 8.41 | 1 | 0.93 |
| 9 | V, VI | 7 | 6.5 | 5 | 4.67 | 2 | 1.90 |
| Total | 107 | 100.0 | 62 | 57.30 | 45 | 42.00 | |
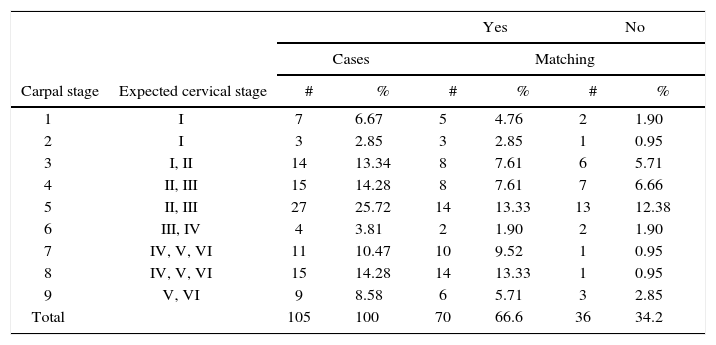
Obtained data from correlation in females.
| Carpal stage | Expected cervical stage | Yes | No | ||||
|---|---|---|---|---|---|---|---|
| Cases | Matching | ||||||
| # | % | # | % | # | % | ||
| 1 | I | 7 | 6.67 | 5 | 4.76 | 2 | 1.90 |
| 2 | I | 3 | 2.85 | 3 | 2.85 | 1 | 0.95 |
| 3 | I, II | 14 | 13.34 | 8 | 7.61 | 6 | 5.71 |
| 4 | II, III | 15 | 14.28 | 8 | 7.61 | 7 | 6.66 |
| 5 | II, III | 27 | 25.72 | 14 | 13.33 | 13 | 12.38 |
| 6 | III, IV | 4 | 3.81 | 2 | 1.90 | 2 | 1.90 |
| 7 | IV, V, VI | 11 | 10.47 | 10 | 9.52 | 1 | 0.95 |
| 8 | IV, V, VI | 15 | 14.28 | 14 | 13.33 | 1 | 0.95 |
| 9 | V, VI | 9 | 8.58 | 6 | 5.71 | 3 | 2.85 |
| Total | 105 | 100 | 70 | 66.6 | 36 | 34.2 | |