


















Nowadays, aesthetic demands are of interest to individuals. Smile is the gateway to human and labor relations, which is why so much importance is given to the care and dental alignment as well as facial harmony. The class II, Division 1 malocclusion is one of the greatest causes of facial disharmony generating a negative psychological impact on people and requires longer treatment periods. Etiology is due to a combination of skeletal, dental and extrinsic factors. This case describes the treatment of a 13-years-old female patient diagnosed with a class II division 1 malocclusion with a 7mm overjet, open bite, tongue thrust, severe crowding and facial disharmony. Treatment goals were to achieve dental and facial harmony in the shortest time possible. The treatment lasted for 15 months and was based on the extraction of upper and lower first bicuspids and placement of Tip-Edge appliances. A molar and canine Class I relationship was obtained, ideal overjet and overbite were established and cosmetic results were satisfactory and significant for the patient. These changes generate greater emotional security in themselves.
La exigencia estética en la actualidad es motivo de interés para los individuos. La sonrisa es la puerta de entrada a las relaciones humanas y laborales, por esta razón se le da tanta importancia al cuidado y a la alineación dental, así como a la armonía facial. La maloclusión clase II división 1, es una de las que causa mayor desarmonía facial generando un impacto psicológico negativo en las personas y requiere mayor tiempo de tratamiento. Este caso describe el tratamiento de una paciente femenina de 13 años de edad que presenta una maloclusión clase II división 1, con un overjet de 7mm, mordida abierta, proyección lingual, apiñamiento severo y desarmonía facial. Su etiología se debe a una combinación de factores esqueléticos, dentales y extrínsecos. Los objetivos del tratamiento fueron lograr una armonía dental y facial en el menor tiempo posible. El tratamiento duró 15 meses y se basó en extracciones de los primeros premolares superiores e inferiores y la colocación de aparatología Tip-Edge. Se obtuvo relación molar y canina clase I, un adecuado overjet y overbite. Los resultados estéticos fueron satisfactorios y signiicativos para la paciente. Estos cambios generan mayor seguridad emocional en ellos mismos.
Today, aesthetic treatments are more common worldwide. Within the current aesthetic demands is the desire to achieve an aesthetic smile and a pleasant facial harmony since they provide security to the people and is a gateway to human relations. Therefore, people seek orthodontic treatments that meet their needs in the shortest possible time more frequently.1,2
An inadequate position of the teeth that creates functional and aesthetic problems is known as malocclusion. One of the most difficult to treat malocclusions and that causes more severe facial and dental disharmony is class II division 1 malocclusion. This occlusal disharmony produces a negative psychological impact on the patients.
It is characterized by a distal position of the canines and molars with respect to the upper, as well as a protrusion of upper incisors. The facial muscles and tongue adapt to abnormal patterns of muscle contraction in this kind of occlusal disharmony.2,3
This malocclusion may also be associated with open bite, which may be related to environmental, skeletal factors and to neuromuscular alterations of the lips and/or the tongue. This disturbance causes the malocclusion to be more severe and a more unpleasant physical appearance for the patient.2–5
Treatment planning for this malocclusion should be individualized for each patient and must consider several factors to deal with, so as to achieve a successful treatment that provides stability, aesthetics and function of the occlusion and that also fulills the patient's expectations.3,5
CASE REPORTFemale patient, 13 years of age, who attended the clinic of the Department of Orthodontics at the DepeI, Faculty of Dentistry, UNAM. The reason for consultation was: «Because she noticed that she had very misaligned teeth» as referred by the mother in addition to commenting that this had caused the patient to show insecurity among other people. Upon medical and clinical interrogation, the patient did not refer any pathology and it was established that she was apparently healthy. The extraoral clinical analysis revealed a dolichofacial patient, proportionate facial thirds, medium-sized and incompetent lips (Figure 1A). The facial midline coincided with the upper dental midline and she presented crowding in the upper and lower arch (Figure 1B). Her profile was convex (Figure 2).
INTRAORAL ANALYSIS Initial facial frontal photograph. B) Initial smile photograph.")

In the intraoral analysis, it was observed that the upper and lower midlines did not match, an anterior open bite, healthy and complete periodontal tissues and an increased overjet (Figure 3). In the intraoral lateral photographs, a molar and canine class II was observed on both sides (Figures 4 and 5).



The upper arch presented a triangular shape, the dental organs #11, 12, 21 and 22 were labially inclined, #16 was rotated mesially, #14 showed a distal rotation and #15, 17 and 27 were partially erupted. The lower arch had a squared shape, the dental organs #33, 34, 43 and 44 had a mesial rotation (Figures 6A and 6B).
DIAGNOSIS Upper arch: triangular shape. B) Lower arch: squared shape.")
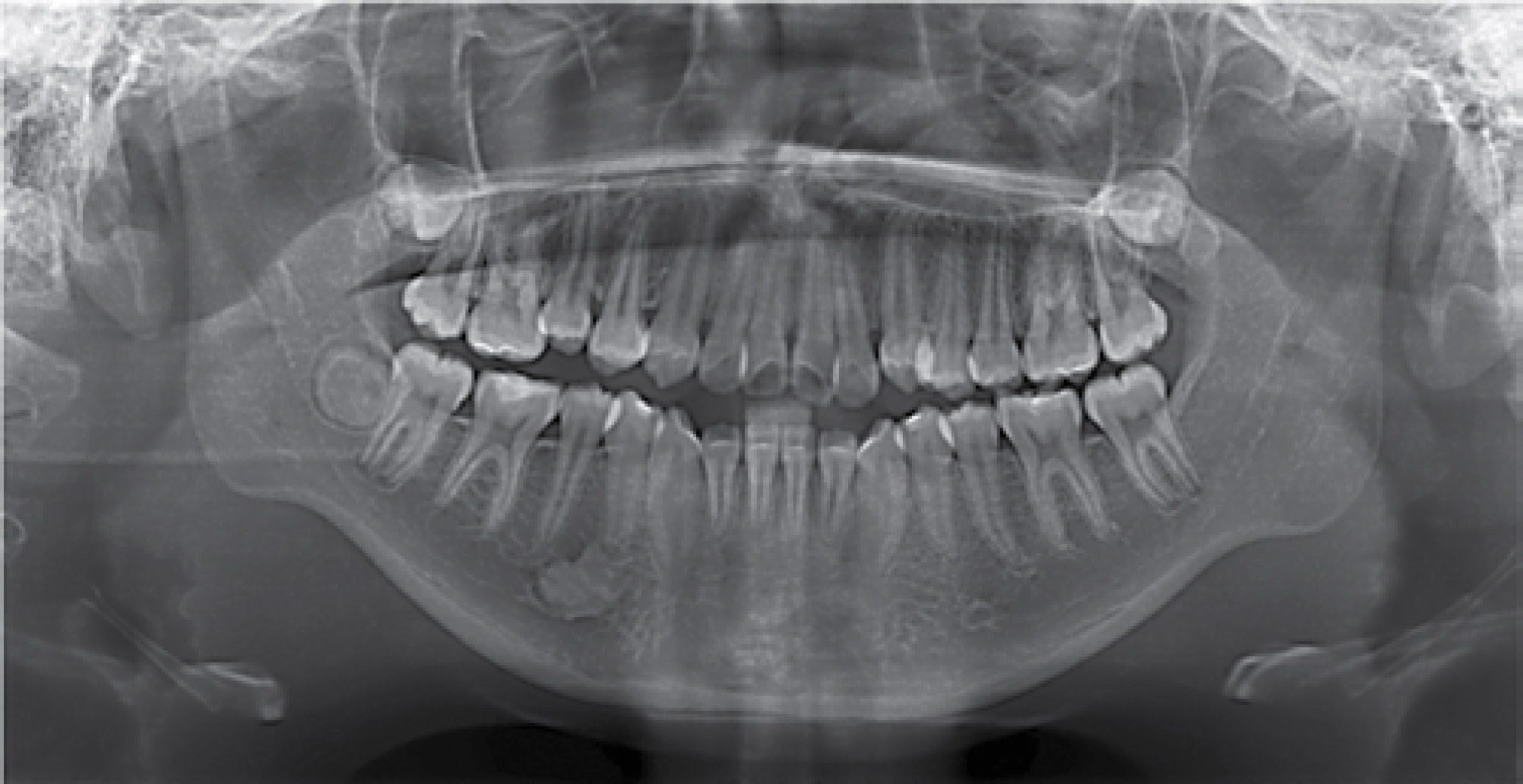
The diagnosis was made on the basis of the patient's clinical extraoral and intraoral analysis, study models’ and radiographic analysis (Figures 7 and 8), the following conclusion was made: Skeletal Diagnosis: skeletal class II due to a slight maxillary protrusion and a posterior position of the mandible, vertical growth, and incisor proclination (Figure 8).


Facial diagnosis: dolichofacial, convex profile and lip protrusion.
Dental diagnosis: molar and canine class II on both sides, upper and lower dental proinclination, open bite, dental midlines do not match, increased overjet (Figure 9). The patient exhibited a triangular-shaped upper arch and a square- shaped lower arch with rotations in both (Figures 6A and 6B).

Articular and functional diagnosis: the patient did not refer any TMJ symptoms. The patient presented a tongue thrust habit and was not satisfied with her dental appearance.
Treatment objectives: the goals of treatment were: to correct the lingual projection, improve the profile, close the open bite, obtain molar and canine class I on both sides, correct the incisors’ axial axis, eliminate the crowding and achieve an adequate overjet and overbite.
TREATMENT PLANThe patient was first referred to the department of Oral surgery and Oral pathology for analyzing the radiopaque area that was observed apically of the dental organ #44 in the panoramic radiograph and for extraction of the first upper and lower premolars. Tip-Edge appliances were placed. There was an initial alignment and leveling phase with a 0.016” Australian archwire with a helix between the lateral incisor and canine of the four quadrants. The use of 5/16” lightweight class II elastics was indicated (Figure 10). Subsequently space closure was initiated with a 0.022” stainless steel archwire and the use of e-links in the four quadrants; 5/16” medium class II elastics were indicated (Figure 11). Finally, the final phase was carried out with 0.028 x 0.022” archwires and the use of springs for root straightening and 1/4” medium class II elastics (Figure 12). Treatment was finalized with 0.019 x 0.025” braided archwires and 3/8” medium elastics to achieve occlusal settlement. During treatment tongue exercises were prescribed.



At the end of the treatment an occlusal adjustment was performed and Hawley retainers were placed on the upper and lower arch.
RESULTSAll treatment goals were achieved in fifteen months. Facially, the profile, lip competence and facial harmony were improved (Figure 13). Canine and molar class I was achieved on both sides, the axial axis of the teeth were improved and the anterior open bite was closed (Figure 14). Aesthetics, function and stability in the occlusion were obtained for the patient.


The aesthetic dental results and facial harmony were satisfactory as well as the cephalometric changes where an improvement in dental inclinations may be observed as well as the preservation of anchorage to obtain the planned facial changes thus generating more security for the patient (Figures 15 to 17).
DISCUSSION


Class II Division 1 malocclusion is difficult to correct and causes an important facial and dental disharmony with a negative psychological impact on patients. This affects their self- conidence and security in relating with others.
A treatment that meets the patient's needs in the shortest possible time as the Tip Edge System offers, without risk to the dental and periodontal tissues and that provides stability, function and aesthetics in the occlusion will be a well-accepted treatment.
It should also be taken into consideration that orthodontic treatments must be individualized for each patient and type of malocclusion, considering several factors in order to achieve a successful treatment that fulfills the patient's expectations.
CONCLUSIONS- 1.
Today there are more people looking for an orthodontic treatment that provides dental aesthetics and harmony, in an easier way and less time so it is advisable to consider the use of techniques and systems in Orthodontics that provide such results in reduced times.
- 2.
It has been demonstrated in the literature that the Tip-Edge System is an option of fixed orthodontic treatment with reduced times that surpasses other conventional orthodontic systems.6–8
- 3.
Class II division 1 malocclusion patients usually have a severe facial and dental disharmony which produces a negative psychological impact on patients.
- 4.
These patients have a need for their problem to be solved in the shortest time possible and when this happens, they show a radical change in their personality.
- 5.
The patient was treated with Tip-Edge appliances for fifteen months and her four first premolars were extracted for crowding correction, anterior bite closure and profile improvement.
- 6.
The aesthetic dental results and facial harmony were satisfactory to the patient and these changes generated more emotional security in her.
- 7.
Orthodontic treatment planning must be individualized for each patient and consider several factors in order to achieve success, provide stability, dental aesthetics and function and also meet patient's expectations.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia