













The main objective of the present article is to report a parallelization method for a retained lower second molar.
MethodA mini-implant was placed in order to use a spring with an uprighting bend which was directed to the dental organ #47 towards its correct position.
ResultsAn adequate parallelization of the lower right second molar was achieved.
ConclusionsThe presented case shows an option for molar parallelization that attempts to maintain long-term stability which is one of the objectives of contemporary orthodontics.
El objetivo principal del presente artículo es reportar el método de la paralelización de un segundo molar inferior retenido.
MétodoSe colocó un miniimplante, para luego emplear un resorte en un doblez de la paralelización mediante el cual se dirigió el órgano dental 47 hacia su posición correcta.
ResultadosSe logró la adecuada paralelización del segundo molar inferior derecho.
ConclusiónEl caso presentado muestra una opción de paralelización de un molar, que procura mantener la estabilidad a largo plazo, lo cual es uno de los objetivos de la Ortodoncia contemporánea.
Aretained tooth is one that has not erupted in the dental arch in the expected time.1 the prevalence of second molar impaction is usually 0.3%, it is more frequent in the mandible than in the maxilla, and it occurs unilaterally. There is a slight preference for the female sex, and tipping towards mesial is more common.2,3 In a study carried out by Choo s it was stated that retention of the second molar is between a 0.1 and 0.06% prevalence.4,5 Bondemark et al observed disturbances in the eruption of the second molar in 2.3 per cent of the patients.6
The teeth that more frequently suffer from retention are: maxillary and mandibular third molars, maxillary canines and secondmandibular molars.7–10
When seconds molars retentions are found, they usually present a challenge both for the orthodontist and the surgeon. Unilateral impaction is more common than the bilateral kind, and it is more frequent in the mandible, more frequent in men than in women, and usually on the right side. Second molars are usually found mesially tipped.11
Second molars erupt as a result of the remodeling changes of the anterior border of the mandibular ramus after a self-adjustment of their pre-determined mesial tipping. However, lack of space in the arch due to an inadequate mandibular growth, a non-desirable axial inclination or orthodontic mechanics for distalizing irst molars may interfere with the self-correction of the mesial inclination resulting in a retention.
CASE REPORTMale patient, 14 years 8 month of age attends the Orthodontics clinic at the Postgraduate Studies and Research Division of the Faculty of Dentistry, UNAM, with a chief complaint «my parents brought me here and I want straight teeth».
An increased lower facial third is observed in the facial analysis, as well as a convex proifle, hypertonic perioral muscles and a facial midline that coincides with the upper dental midline (Figure 1).
 Frontal view, B) smile frontal view, C) Proile, D) three-quarters.")
Lower dental midline deviated to the left was observed in the intraoral analysis, as well as severe upper and lower anterior crowding, proclined upper left central incisor, upper right lateral incisor edge to edge with the lower canine, overjet 6mm and overbite 1mm (Figure 2). Mesial inclination and infraocclusion of the lower second molar was also observed. Right side and left side molar and canine Class I as well as palatal inclination of the upper left lateral incisor was observed.
 Right view, B) Frontal view, C) Left view, D) Upper occlusal view, and e) Lower occlusal view.")
Symmetric maxillary sinuses were observed in the radiographic analysis, and loss of interproximal alveolar crests, short roots of the dental organs #31, 32, 41 and 42, absence of the third molars, only dental organ #48 and mesial inclination of the lower right second molar (Figure 3).

The cephalometric diagnosis was skeletal Class I patient with a brachifacial pattern and horizontal growth (CCW 71.6%) (Figure 4).
TREATMENT
The main objective that this article presents is the parallelization of the lower right second molar which was conducted in the patient; however the complete objectives of the orthodontic treatment that the patient received are hereby mentioned: improve the profile, decrease the lower facial third, maintain molar class I, obtain canine class I, eliminate anterior upper and lower crowding, coordinate arches, correct the axial axis of the upper and lower teeth and correct the midline. MBT prescription fixed appliances were placed. Upper and lower first premolar extractions were performed. A supper anchorage, a transpalatal bar was used and on the lower, a lingual arch (Figure 5).
 Right side, B) Frontal, C) left side, D) upper and E) Lower.")
Phase I. Alignment and leveling with 0.016” NiTi, 0.019” x 0.025” NiTi archwires and passive lacebacks.
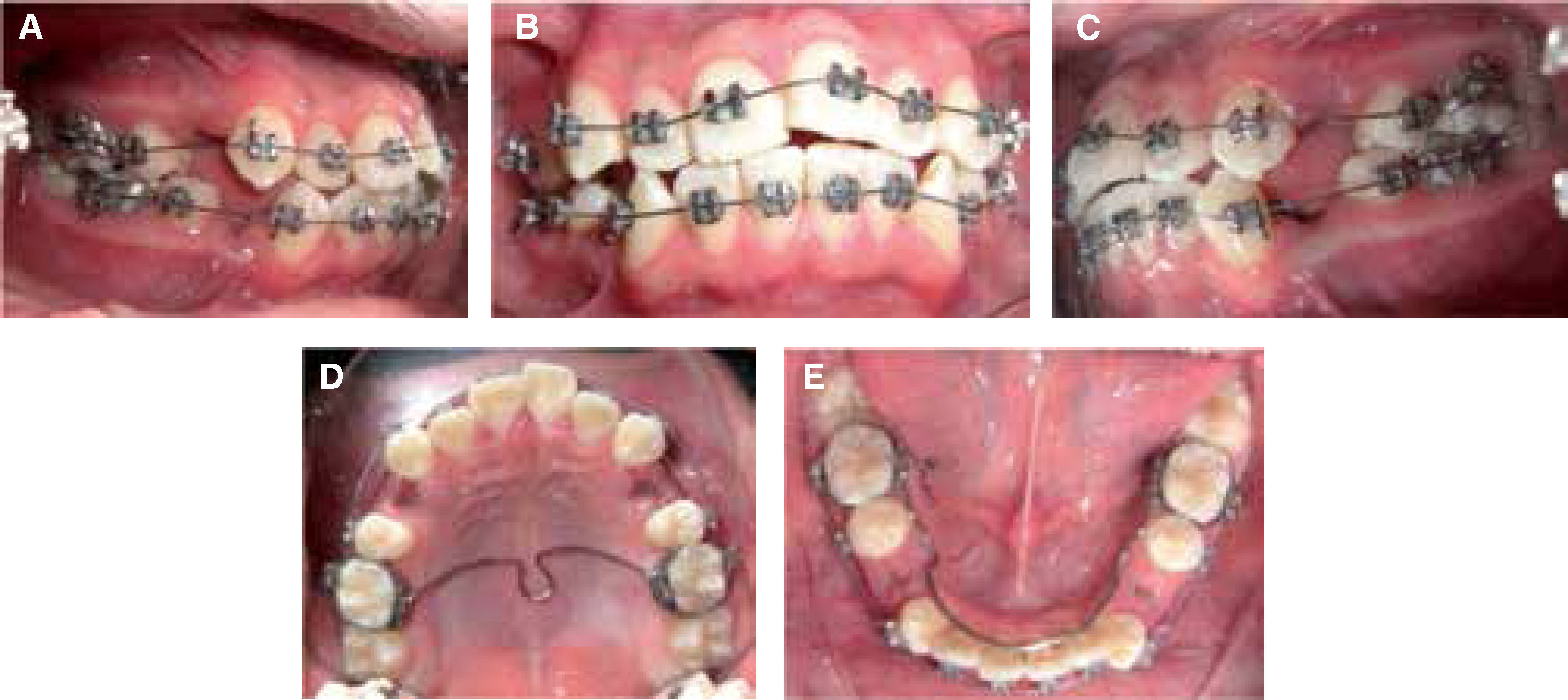
Phase II. 0.019” x 0.025” SS archwires. Activelacebacks. During this phase, an 8 mm-length mini-implant was placed in the buccal area between the roots of the lower right first and second molars (Figure 6). After a month from the placement of the mini-implant a spring was used with a parallelization bend to direct the crown of the dental organ #47 (D.O. distally (Figure 7).


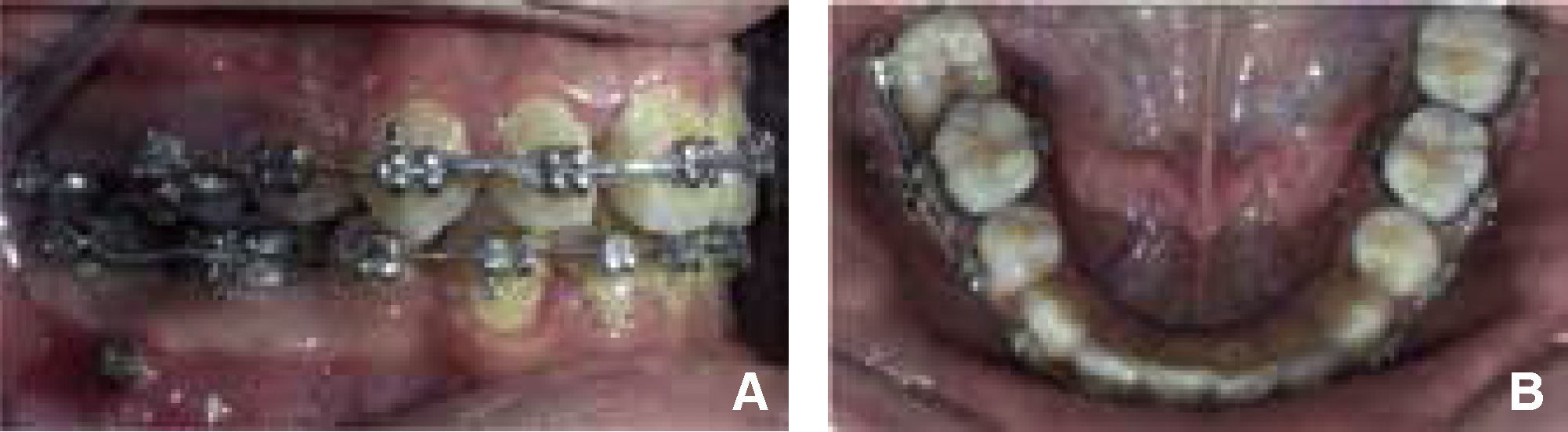
In May 2013, the spring was removed and a continuous 0.016” x 0.022” NiTi archwire was used for aligning and leveling the D.O. 47 (Figure 8).
 Right lateral view, B) Lower occlusal view.")
Phase III. Treatment continued with the finishing and detailing of the case using the final sequence of archwires from the MBT technique.
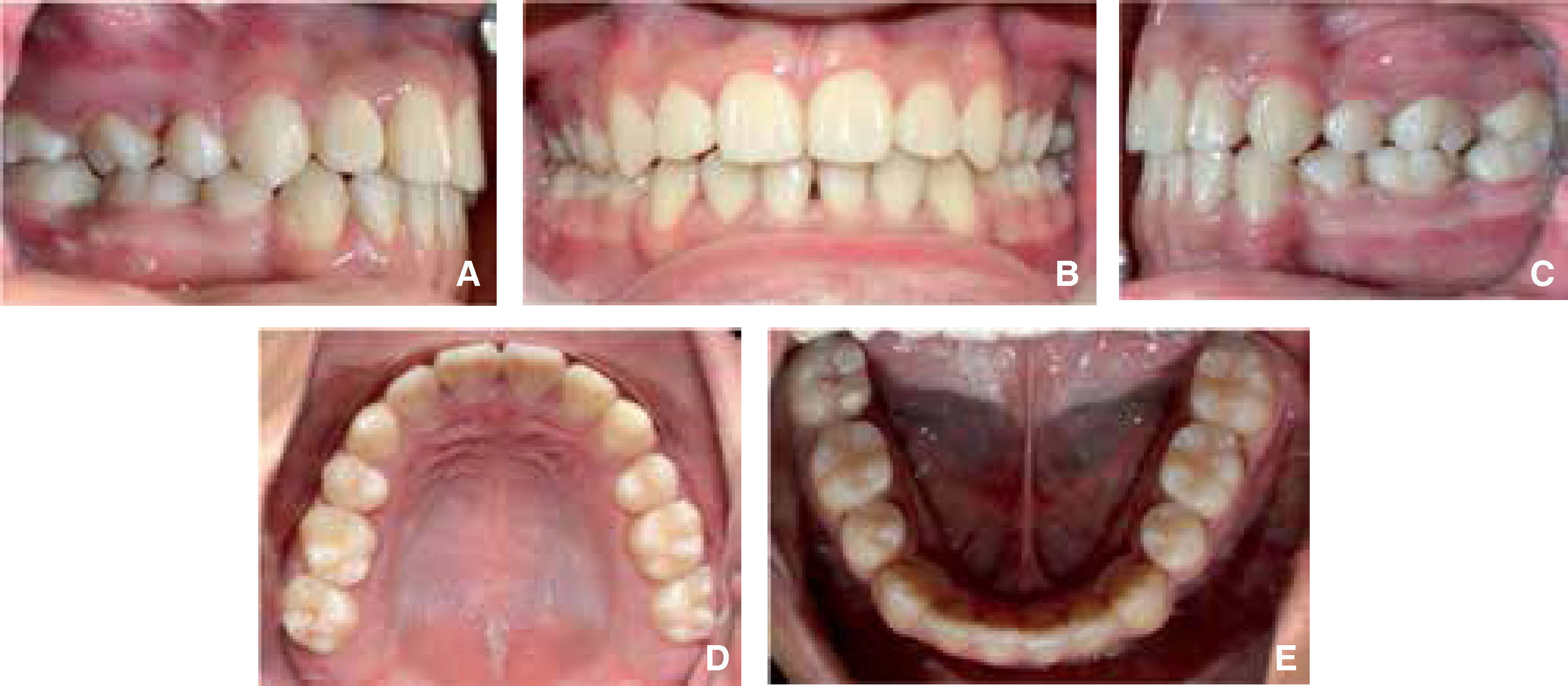
Fixed appliances were removed in January 2014 (Figures 9 and 10). It may be observed that the overall goals of treatment were met, as well as the particular aim of parallelization of the lower right second molar (Figures 11 and 12).
 Right, B) Frontal, C) Left, D) Upper occlusal view and e. lower occlusal view.")
 Frontal view, B) smile, C) Proile and D) three quarters view.")


For post-treatment retention, circunferential retainers were indicated and a bimaxillary positioner at nights (Figures 13 and 14).


A wide range of treatments for the second molar impactionhas been published being mostly a combination of orthodontic and surgical techniques with the goal of placing the tooth in the correct position. Some of these techniques include: surgical removal of the second molar and letting the third molar erupt in the place of the second, surgical removal of the second molar and transplanting the third molar in place of the second, surgical exposure of the second molar and reposition through orthodontic techniques.13–15 However, in the case hereby presented the patient no longer had the lower right third molar so it was important to choose a suitable alternative.
In the present article a viable alternative for the parallelization of a second lower molar is suggested which results in an option to fullfill the objectives of the orthodontic treatment.
CONCLUSIONIt is important to identify the needs of each patient as well as to provide a treatment that maintains the pulp and periodontal health of both the teeth to be treated and the adjacent structures. The case presented shows an option that seeks to maintain long-term stability which is one of the objectives of the contemporary Orthodontics.
Graduates of the Orthodontics Specialty.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia