










Anterior open bite is a malocclusion in which one or more teeth do not make contact with its antagonists. The malocclusion occurs in the incisors zone and can spread even to posterior teeth. Molar intrusion is one of the main treatment mechanisms, but the methods used to achieve it have been ineffective, mainly because they depend on dental structures resulting in anchorage loss. On the other hand, mini-implants are easy to place, remove and a low-cost alternative to treat anterior open bite. They are an efficient tool to provide anchorage without patient cooperation. This article explains how closure of an anterior open bite was achieved using mini-implants in the maxilla (buccal and palate area with an acrylic button with hooks) and mandible (buccal area). It aims to explain that mini-implants are efficient in causing molar intrusion because they provide more options to correct malocclusions without patient’s cooperation.
La mordida abierta anterior es una maloclusión donde uno o más dientes no establecen contacto con sus antagonistas, se presenta en la zona de los incisivos y puede extenderse hasta los molares. La intrusión molar es uno de los mecanismos principales para tratarla, los medios que se han utilizado para este fin han sido poco eficaces, pues se basan en estructuras dentales dando como resultado la pérdida del anclaje. En contraparte, los mini-implantes proporcionan una fácil colocación, remoción y bajo costo para tratar la mordida abierta anterior y son una herramienta más para obtener un anclaje sin la colaboración del paciente. Este artículo explica cómo se logró el cierre de mordida abierta anterior, por medio de mini-implantes en maxila (zona vestibular y palatina con un botón de acrílico con ganchos) y mandíbula (zona vestibular). Se pretende explicar que los mini-implantes son eficientes para el tratamiento de la intrusión molar, porque ofrecen más opciones para la corrección de las maloclusiones sin depender tanto de los pacientes.
Open bite results from an obvious lack of contact between the upper and lower teeth, in the incisor area or in the posterior segments of the arches.1
Vertical dimension control has been a very important factor in open bite treatment and molar intrusion. There are several methods to solve this problem depending on the etiology of the malocclusion2 whether it is due to genetic factors, unfavorable growth patterns, thumbsucking, mouth-breathing and atypical swallowing habits, among others. For the correction of less severe problems, there are functional orthopedic appliances such as the high-pull headgear, posterior bite-planes and appliances to correct tongue thrust.2–4
The more severe cases usually end up being corrected with combined surgical-orthodontic treatment.
The need to provide absolute anchorage in orthodontics has caused the development and evolution of mini-implants, perfect alternative treatment for anterior open bite correction by molar intrusion. Mini-implants are pyramidal, self-drilling screws, with a slightly tapered profile which come in different heights, diameters and lengths. They are biocompatible, do not suffer expansion, and are small in order to be placed in any area of the mouth. Mini-implants must with stand orthodontic loads (up to 300 g) in all planes of the space and can be placed and removed with ease under local anesthesia upon completion of the biomechanical therapy.5–7
Recently, some case reports of molar intrusion have been published as a method for correcting open bites through titanium plates which are invasive, expensive and require an operating room for their placement. In the 2008 Sakai et al. reported a case of open bite corrected with molars intrusion through mini-implants.8
The great diversity in mini-implant designs that are available nowadays has facilitated the construction of appliances that can be applied on them. Björn Ludwig suggested placing a lingual button to counteract the force applied to the mini-implants on the buccal thus obtaining a vertical force vector and avoiding buccal crown torque on the molars.9
Orthognathic surgery was, until recently, the only alternative to treat severe bite open bites but now there are mini-implants, which have revolutionized orthodontic treatments into more conservative ones, without putting the patient’s life at risk.
Case reportDiagnosis21-year-old female patient referred to the Orthodontics Clinic of the Postgraduate Studies and Research Division of the National Autonomous University of Mexico for treatment of moderate upper and lower dental crowding and anterior open bite. Upon medical history, the patient was declared to be healthy. Upon intraoral clinical examination, no pathological data was found nor any pain or TMJ symptoms.
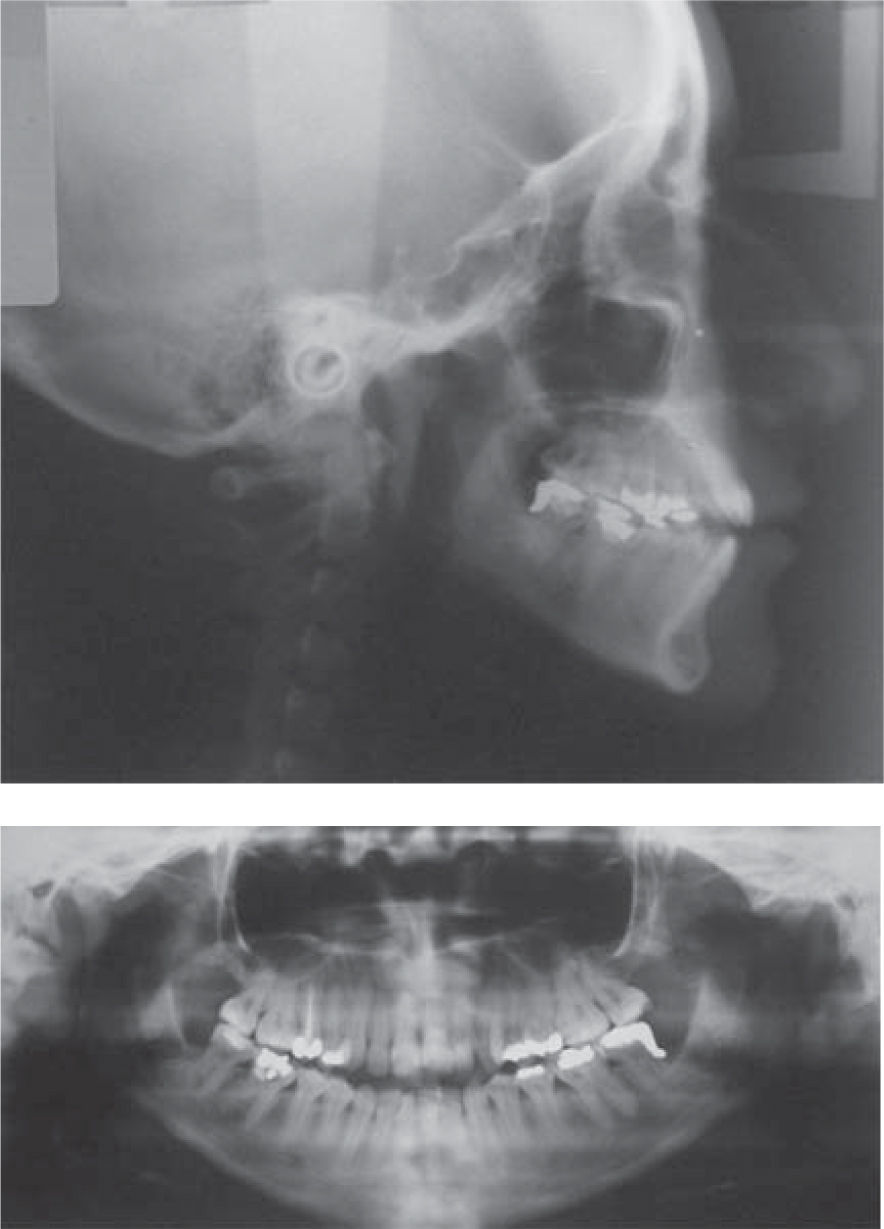
The facial photographs analysis showed a dolichofacial patient, straight profile, straight nose, competent lips, positive smile and the dental midline matched the facial midline. In the intraoral photographs, anterior open bite, posterior cross bite, non-matching upper and lower midlines, Angle molar class I, canine class I, a parabolic arch form and mild upper and lower anterior crowding was observed (Figures 1 to 3).



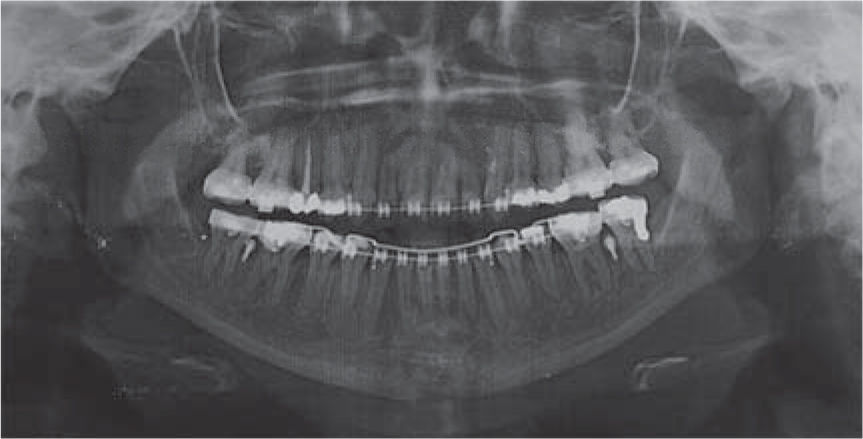
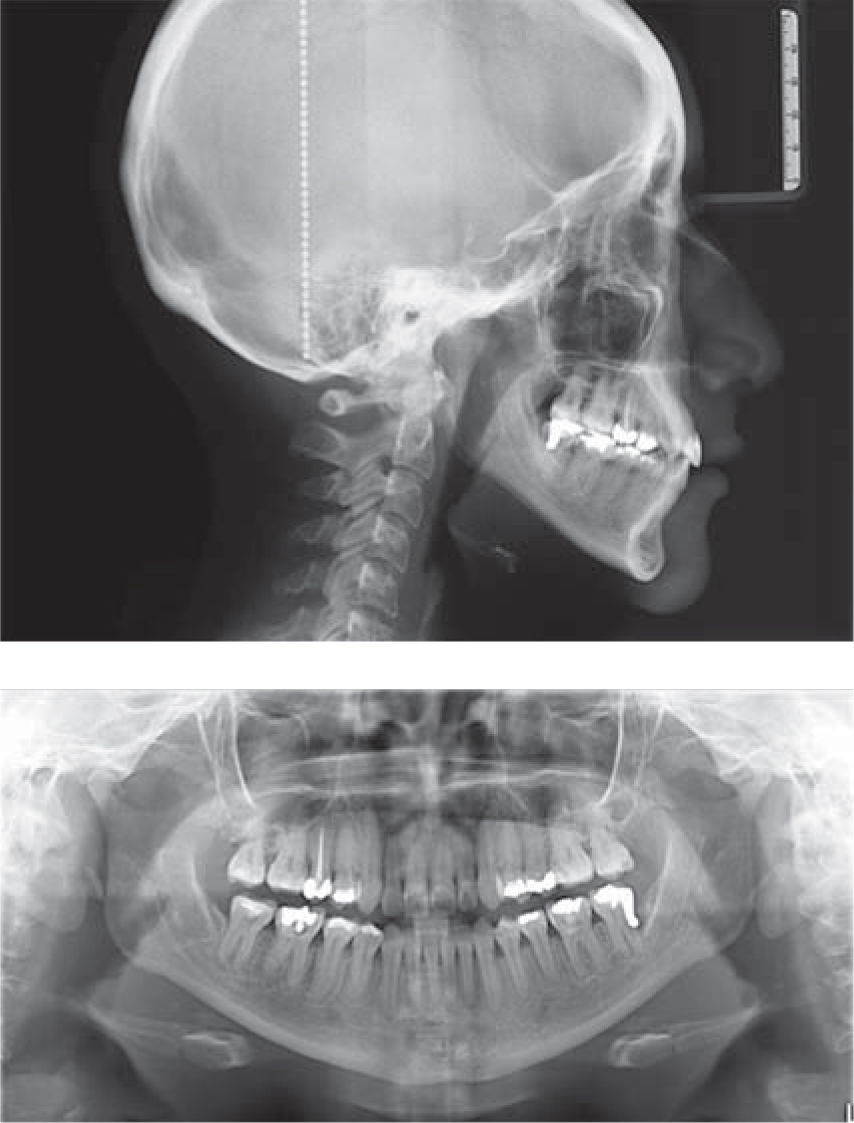
In the panoramic radiograph (Figure 2) it was observed: symmetrical condyles and mandibular ramus, maxillary sinuses without any obstruction, leveled alveolar crests, 28 teeth, 2:1 root-crown ratio, root canal treatment in the upper right premolar and a poorly adjusted dental filling on the lower left second molar.
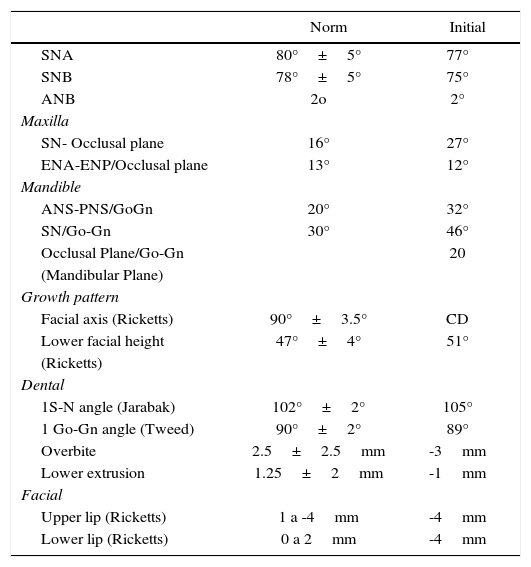
The cephalometric data showed that the patient was skeletal class I with open bite, vertical growth pattern and incisors within their basal bones. The data suggested by Acuña et al.10,11 and Argüelles et al. for open bites were considered (Table I).
Cephalometric data.
| Norm | Initial | |
|---|---|---|
| SNA | 80°±5° | 77° |
| SNB | 78°±5° | 75° |
| ANB | 2o | 2° |
| Maxilla | ||
| SN- Occlusal plane | 16° | 27° |
| ENA-ENP/Occlusal plane | 13° | 12° |
| Mandible | ||
| ANS-PNS/GoGn | 20° | 32° |
| SN/Go-Gn | 30° | 46° |
| Occlusal Plane/Go-Gn | 20 | |
| (Mandibular Plane) | ||
| Growth pattern | ||
| Facial axis (Ricketts) | 90°±3.5° | CD |
| Lower facial height | 47°±4° | 51° |
| (Ricketts) | ||
| Dental | ||
| 1S-N angle (Jarabak) | 102°±2° | 105° |
| 1 Go-Gn angle (Tweed) | 90°±2° | 89° |
| Overbite | 2.5±2.5mm | -3mm |
| Lower extrusion | 1.25±2mm | -1mm |
| Facial | ||
| Upper lip (Ricketts) | 1 a -4mm | -4mm |
| Lower lip (Ricketts) | 0 a 2mm | -4mm |
According to the diagnosis, it was decided to perform upper and lower molar intrusion to correct the open bite and obtain an adequate overbite and overjet, avoiding at the same time, the extrusion of the teeth adjacent to the molars and facial vertical changes.
Treatment planThree alternative treatment plans were suggested to the patient; one of them was to correct the open bite with a combination of orthodontics (conventional treatment with MBT prescription brackets) and orthognathic surgery (posterior maxilla impaction). The second one was conventional orthodontic treatment with of upper and lower premolar extractions, 0.022” MBT brackets, maximum anchorage (with a low transpalatalbar and high-pull headgear), (lower anchorage with lingual arch). And the third was molar intrusion with mini-implants in the upper and lower arch in addition to placing a lingual button with hooks and placement of 0.022” slot MBT bracket prescription fixed appliances. The patient chose the latter option because it was the more conservative, economic and less risky.
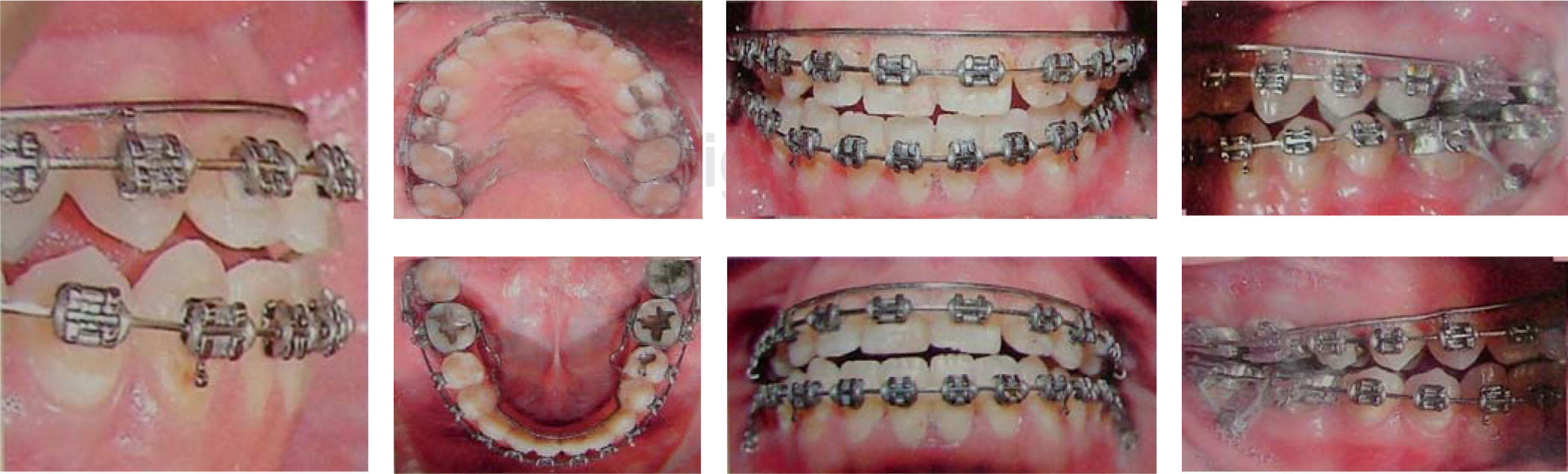
Treatment progress0.022” slot MBT brackets, first and second molar maxillary bands with a lingual button soldiered in the palatal surface of each band and mandibular bands with lingual sheaths were placed. To solve the crowding, align and level, 0.016” upper and lower NiTi archwires were placed. The archwire sequence suggested for the MBT prescription was applied until finishing with 0.019×0.025” SS archwires (Figure 4).

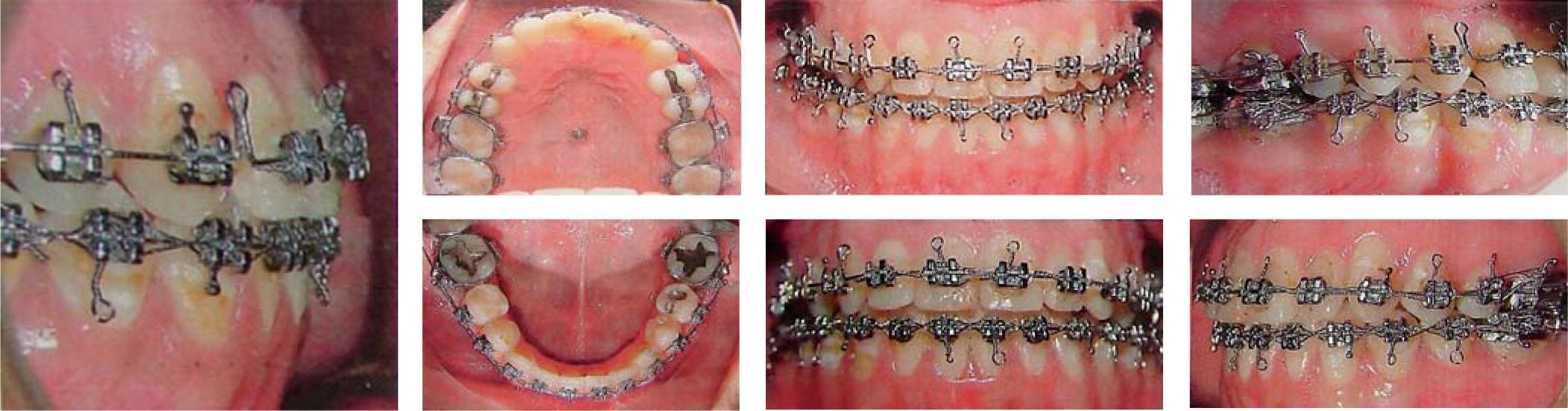
Self-drilling and self-tapering 2.5×1.6×6mm diameter mini-implants from the brand O.S.A.S Dewimed® were placed at the mucogingival line on the buccal surface between the first and second premolars, and in the palate, two mini-implants were placed, one on each side of the palatal suture.5–7,10–13 An acrylic button with four 0.036” stainless steel wire hooks, one on the distal portion of the button, one on the mesial, and in close proximity to the first and second molar crowns was made. A groove was made on palatal area of the acrylic button with the purpose of being bonded with resin (Transbond XT 3M Unitek) for molar intrusion from the buccal as well as the palatal side simultaneously to obtain a vertical force vector. The mini-screw was inserted with a certain angle to increase the cortical anchorage surface7,10 according to the model suggested by Ludwig9(Figures 5and6). The palatal button remained in the mouth for 8 months.

 intrusion movement activation with a closed elastomeric chain.")
It was necessary to place mini-implants on the buccal surface of the mandible to intrude the lower molars and to correct the anterior open bite and obtain anterior guidance. The appliance was activated with an elastomeric chain from the hook on the second molar to the mini-implant and from the mini-implant to the first molar hook both on the right and left side with an approximate force of 150-200 g5,10 to prevent apical root resorption (Figure 7).

To counteract the intrusion force and avoid buccal crown torque on the lower molars, a contracted lingual arch was made as suggested by Umemori14(Figure 8).

For a better intermaxillary relationship, class III elastics were placed (3/16” 6 oz, GAC Thailand) during this procedure. For overbite consolidation, intermaxillary box elastics were used (1/8 of 3mm and 6 oz, GAC Fiji), in the anterior and posterior segments.4,1
In the upper arch, the lingual button and a mini-implant were removed, since they detached when removing the appliance. On the one that remained, elastomeric chain was placed directly to continue the intrusion of the upper molars. An over-expanded 0.036” accessory stainless steel arch was also constructed above the main archwire to prevent the molars moving lingually. Additionally, stripping was performed from dental organ 35 to 45 to obtain overjet. After thirteen months (eight on the maxilla and five in the mandible) the mini implants were removed, ties and intermaxillary box elastics were placed in each of the anterior teeth for overbite consolidation (Figure 9).

The system of force that was used to get the vertical and horizontal overbite, focused mainly on the intrusion of the maxillary and mandibular molars with the help of the mini-implants, the button palatino and lingual arch, the arches used in this moment of force (0.019×0.025” of NiTi), which contributed to the slight extrusion in anterior teeth and premolar teeth as a result of the alignment and leveling of the same, producing as a whole the closure of the previous bite.
This system, in addition to providing a molar intrusion mechanics, worked as skeletal anchorage, so while the anterior segment suffered mild extrusion, the molars were maintained in their position, isolating the reciprocal force toward them.
ResultsThe results were obtained with the analysis and comparison of the initial and final photographs, study models and cephalometric analysis.
Extraoral photographs: The facial smile photograph showed significant aesthetic improvement. The midline was corrected the deviation and the dental crowding was solved. No difference was observed in regard to dental exposure compared with the initial photograph. The profile was maintained as it was at the beginning of treatment (Figure 10).

Intraoral photographs: When comparing the initial and final photographs, the alignment and leveling of the upper and lower arches, the closure of the anterior open bite that resulted in a 3mm overbite and 4mm overjet, molar and canine class I, and cross bite of the seconds upper molars may be observed (Figures 11and12).


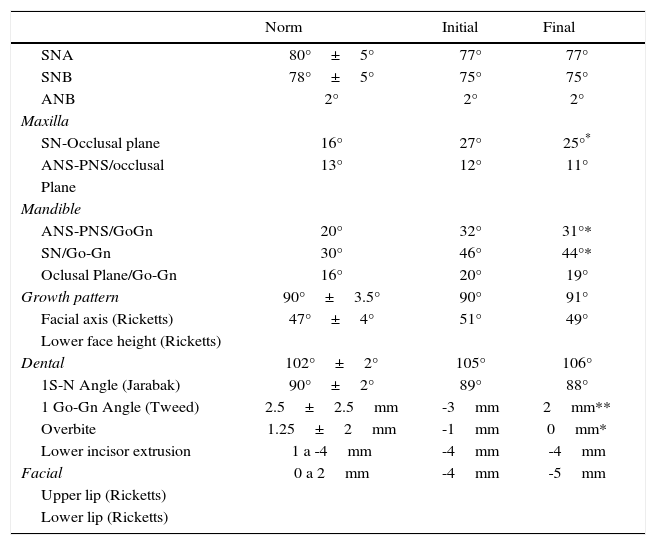
Lateral head film: There were no significant changes with regard to theSNA, SNB and ANB angles.
The angles that were considered for determining a change in the open bite with respect to the maxilla were: SN-occlusal plane that decreased 2° as well as ANS-PNS/occlusal plane which decreased 1°. This is favorable for the open bite correction. To assess the changes that occurred in the mandible, the SN/ Go-Gn Angle which decreased 2° and the occlusal plane/ Go Gn angle that decreased by 1° were considered (Figure 13).

To determine the closure of the open bite the Ricketts lower facial height which decreased 2° and the Ricketts facial axis which increased 1°, were considered. It can be assumed that the mandible had a slight counter-clockwise rotation, thanks to the molar intrusion which contributed to the open bite correction.
The incisor inclination was determined by the 1 S-N angle which increased 1°. This caused a dentoalveolar modification of the upper incisors and the 1 Go-Gn angle decreased 1°. This was interpreted as retroclination of the lower incisor that combination with the upper incisor resulted in an overjet.
The overbite increased by +5mm and the lower incisor extrusion was +1mm, which contributed to obtaining an appropriate overbite. In conclusion, the main goal of our problem list was satisfactorily achieved.
No changes were noted in the Ricketts facial line determined by the upper lip of and the lower lip which decreased 1mm (Table II).
Final cephalometric data.
| Norm | Initial | Final | |
|---|---|---|---|
| SNA | 80°±5° | 77° | 77° |
| SNB | 78°±5° | 75° | 75° |
| ANB | 2° | 2° | 2° |
| Maxilla | |||
| SN-Occlusal plane | 16° | 27° | 25°* |
| ANS-PNS/occlusal | 13° | 12° | 11° |
| Plane | |||
| Mandible | |||
| ANS-PNS/GoGn | 20° | 32° | 31°* |
| SN/Go-Gn | 30° | 46° | 44°* |
| Oclusal Plane/Go-Gn | 16° | 20° | 19° |
| Growth pattern | 90°±3.5° | 90° | 91° |
| Facial axis (Ricketts) | 47°±4° | 51° | 49° |
| Lower face height (Ricketts) | |||
| Dental | 102°±2° | 105° | 106° |
| 1S-N Angle (Jarabak) | 90°±2° | 89° | 88° |
| 1 Go-Gn Angle (Tweed) | 2.5±2.5mm | -3mm | 2mm** |
| Overbite | 1.25±2mm | -1mm | 0mm* |
| Lower incisor extrusion | 1 a -4mm | -4mm | -4mm |
| Facial | 0 a 2mm | -4mm | -5mm |
| Upper lip (Ricketts) | |||
| Lower lip (Ricketts) | |||
The effectiveness, simplicity of placement and removal, stability and low cost has been some of the advantages that mini-implants provide for bone anchorage. They provide a solution to several problems of anchorage loss caused by the reciprocal force that is exerted to perform movements such as retraction of the anterior segment, molar distalization, extrusion and intrusion.
The literature reports several methods for molar intrusion. One of them is used in growing patients and consists in myofunctional appliances that must be used before the eruption of the second molar with the disadvantage that relapse may occur and that the treatment’s success depends on the patient’s growth.4
Iscan and Sarisoy14 studied the effects of passive posterior bite planes for the early treatment of open bite in growing patients through molar intrusion produced by masticatory muscle pressure and upward and forward mandibular rotation. Satisfactory results were obtained. The disadvantage of this treatment is that many times this malocclusion is not timely diagnosed. Regularly, the patient arrives at the clinic with the problem when growth has finished, the patient hereby presented was such a case.
Sakai Y. et al.,8 mentioned a method for open bite closure through the use of headgears, intermaxillary elastics or multiloops, which resulted in extrusion of the anterior teeth compromising function, stability and aesthetics if they are not well managed by the specialist.
Another commonly used procedure for open bite closure with upper crowding is the first or second molar extraction or first or second premolar extraction, where the open bite closes with the aid of extrusion of the anterior segment and incisor retroclination, since the center of rotation is at the apex. This procedure is ideal for patients with severe crowding, and not the treatment of choice for the patient presented in this case report.1
Orthognathic surgery for correction of the anterior open bite causes a major impact in the patient. Facial changes, post-surgical pain and complications, hemorrhage, infection, tooth vitality loss, long posttreatment time and costs must be explained to the patient. In sight of this, other treatment options must be offered to the patient as Lin J.C.Y. et al.15 suggest. In the case report hereby presented, it was explained to the patient all of the abovementioned and she refused «such a radical» surgery.
One of the advantages of mini-implants is that they do not require patient’s cooperation besides from the fact that reciprocal forces do not exist among the teeth that are wished to be moved and the anchorage teeth. Chang Y. et al. mentioned that it is one of the most ideal force systems for molar intrusion without side effects.16
Sakai Y.8 reported a clinical case that was satisfactorily resolved with the intrusion of upper and lower molars through mini-implants, one of the most conservative options for the solution of the problem posed by the patient in this article.
Chun et al. mentioned that the importance applying forces of molar intrusion is that they must be applied simultaneously, both towards the buccal and towards the lingual aspect of the molar.17
De Cleerk and Timmerman18 suggested that in order to prevent the molar intrusion force applied from the buccal from having a tipping effect on the crowns, an attachment in the palatal area must be placed at the same time. Jong-Suk Lee et al.13 considered the palatal area to be the most stable zone as it is formed from dense cortical bone. They mentioned that it is the best area for mini-implant’s placement and that it creates an opposite force moment towards that direction, which will help the intrusion movement. The use of buccal-palatal mechanics introduced by Park H.S. et al.19 to prevent rotation and inclinations was used to correct the case presented here.
Taking into consideration all the previous recommendations, a device was made according to the design by Lee et al13 and also, an attachment to perform the intrusion with vertical vectors. Some modifications were needed in the case hereby presented. An acrylic palatal button with four hooks bonded to two mini-screws placed at each side of the palatal suture was made to serve the same function as the one designed by Lee et al. Modification such as described by Björn Ludwig9 were performed resulting in an applied intrusion force close to the center of resistance.
Mini-implants were also placed in the mandible for intrusion of the mandibular molars. A lingual arch with torque was placed to compensate for the tipping caused by intrusionforces, as recommended by Mikako Umemori et al.10
The combination of molar intrusion with miniimplants and alignment and leveling with the NiTi arches caused a slight extrusion of the anterior segment and produced an appropriate vertical overbite. Maku, Kawai, Koseki et al21 reported a similar case where multiloop arches were used, which, unlike the case presented in this article shows to be a more complicated mechanic due to the loop realization.
Closure of the anterior open bite was achieved with the combination of molarintrusion in upper and lower molars in addition to a slight extrusion of the incisors obtained by means of intermaxillaryelastics as suggested by Quiros and Nanda for the consolidation of the overbite and overjet.4,1
Open bite is one of the most difficult malocclusions to treat, so a more accurate diagnosis should be performed since the success or failure of treatment depends on it. The present case was analyzed with published open bitearticles14,22–24 which suggest specific angles to diagnose it. Molar intrusion cases reported by Lee J,13 Umemori M,20 Sakai Y,8 Park H,19 showed no major changes in the cephalometric data but instead notorious clinical changes. First of all, open bite closure, the consolidation of molar and canine class I, an appropriate overbite and overjet, a more pleasant facial appearance, more relaxed facial muscles, in some cases anadequate labial competence and preservation of the vertical dimension. All these results are similar to those obtained in the patient presented in this article.
Despite all the care that was taken in relation to the force vector’s direction for molar intrusion, the patient presented relapse of the upper second molars cross bite. If this method of molar intrusion is to be used, the placement of a transpalatal arch with torque is suggested after removing the buccal mini- implants in order to avoid the molars returning to their position. Another option is to over-expand the maxillary buccal archwire until treatment is completed. Quiros4 reported a relapse in dolichofacial patients with open bite combined with posterior cross bite. He recommended overcorrection to avoid relapse.
In terms of intrusion stability with mini-implants no long-term data were found in the literature, due to the fact that the implementation of this treatment mechanics is recent. Lin J. et al.15 reported relapses of 30% in the case of dental intrusion of the incisors but not in molars.
Xun, Zeng and Wang23 assessed the effectiveness of mini-implants to correct the open bite in 12 patients between 14 and 27 years of age. All the cases were successfully resolved thus concluding that miniimplants are easy to place and remove, are minimally invasive and require little cooperation from the patient.
ConclusionsOpen bite can be corrected with the use of mini implants for molar intrusion, finally providing a less invasive option compared to orthognathic surgery and the risks that the latter involves. Additionally, it is an option for patients who do not have the economic means to afford an orthodontic-surgical treatment.
The use of the mini-implants as a skeletal anchorage method creates a wider outlook in orthodontic biomechanics because as mentioned above, not only they can be used for molar intrusion, but also to perform movements that require a high magnitude of force without compromising the adjacent teeth with secondary movements.
The success or failure of the anchorage and biomechanics of orthodontic treatment will depend mainly on the specialist, making patient cooperation less important.