





This is a case report of a 17-year-old male patient, with previous orthodontic treatment, who was admitted to the orthodontics clinic for the correction of a skeletal class III malocclusion (Wits -11mm) due to a combination of maxillary hypoplasia and prognathism that was aggravated by an excessive unilateral laterognathia by excessive unilateral mandibular growth. Dentally the patient presented a class III molar and canine relationship, anterior and bilateral posterior cross bite, and upper and lower crowding, lower midline deviation of 7mm o the right. Treatment goals were: improve the facial profile, establish a molar class I, canine class I, to achieve an adequate anterior guidance (overjet, overbite) and dental arch coordination. The treatment was performed in three phases: A) presurgical orthodontic phase: alignment and leveling, dental decompensation, correction of the curve of Spee, and coordination of the upper and lower arches. B) Surgical phase: 2mm maxillary impaction and advancement of 5mm; 7mm mandibular retroposition with Dal Pont technique and a 4mm advancement genioplasty to improve facial aesthetics. C) Postsurgical phase: detailing and settling of the occlusion, final upper and lower arch correlation. The treatment was finished in a period of two years with a successful outcome.
El presente caso es de un paciente masculino de 17 años de edad con tratamiento previo de ortodoncia, que ingresa a la clínica de ortodoncia para la corrección de una maloclusión clase III esquelética (Wits -11mm), debido a una combinación de hipoplasia maxilar y prognatismo mandibular, además de estar agravada por una laterognasia por un excesivo crecimiento mandibular unilateral; dentalmente presenta clase III molar y canina, mordida cruzada anterior y posterior bilateral, apiñamiento superior e inferior, línea media inferior desviada hacia la derecha 7mm. Los objetivos del tratamiento fueron: mejorar el perfil facial, establecer clase I molar, clase I canina, crear una adecuada guía anterior (overjet, overbite) y coordinación de arcos dentales. El tratamiento se realizó en tres fases: A) Fase prequirúrgica ortodóntica: alineación y nivelación, descompensación dental, corrección de la curva de Spee, coordinación de forma de las arcadas superior e inferior. B) Fase quirúrgica: impactación maxilar de 2mm y avance de 5mm; retroposición mandibular con técnica Dal Pont de 7mm, mentoplastia de avance de 4mm para mejorar la estética facial. C) Fase postquirúrgica: detallado y asentamiento de la oclusión, correlación final de arcos superior e inferior. El tratamiento fue logrado en un periodo de dos años con un resultado exitoso.
According to the WHO, in Mexico dental malocclusions represent a public health problem in 75% of adolescents;1 class III malocclusions represent a 10 per cent of the total number of men and 7% of the total number of women. The incidence of this malocclusion in the white population is of 1-5%, in Asian population, 9 to 19% and in Latino population, it is 5%.2
Skeletal class III malocclusion is characterized by upper incisor proclination and retroclination of the lower incisors to compensate for the sagittal skeletal discrepancy.3 The etiology of skeletal class III is multifactorial involving hereditary factors (race), environmental influences (normal position of the jaw or mouth breathing which stimulates mandibular growth) and pathologies (pituitary tumors such as acromegaly).4
Dentofacial anomalies create a disharmony in the maxilla and the mandible, distorting facial aesthetics and masticatory function. The majority of patients with a severe skeletal class III malocclusion are candidates for orthognathic surgery, which is the procedure of choice and provides the best results by obtaining esthetics and a functional occlusion.5 There are several alternatives to address this problem that depend on the discrepancy of the apical bases; when this discrepancy is mild, the malocclusion may be treated with orthodontic camouflage; in the event that the discrepancy between basal bones is moderate to severe consideration should be given to orthodontic treatment in combination with orthognathic surgery.6 During the orthognathicsurgical treatment the maxillary and mandible are redirected. At the same time, the soft tissues also take a new position in all three planes of space. In general, facial aesthetics is improved after surgery, but these changes are observed mainly due to soft tissue changes.7,8 It should also take be taken into consideration the posterior airway since performing movements in the jaws produces an alteration of the oropharyngeal space: the produce a downward movement of the posterior nasal spine increases the spacing nasopharyngeal and oropharyngeal space decreases, which shows that it is of the utmost importance to make a correct surgical and orthodontic planning –so as not to significantly affect the airways.9
CASE REPORTMale patient, 17 years of age attends the Orthodontics Clinic of the University of Guadalajara; his chief complaint was «I want to correct my mandible». The patient did not present any pathological data, systemic diseases or TMJ problems. (At the time, he had fixed appliances that were placed previously).
Clinical examination:- a)
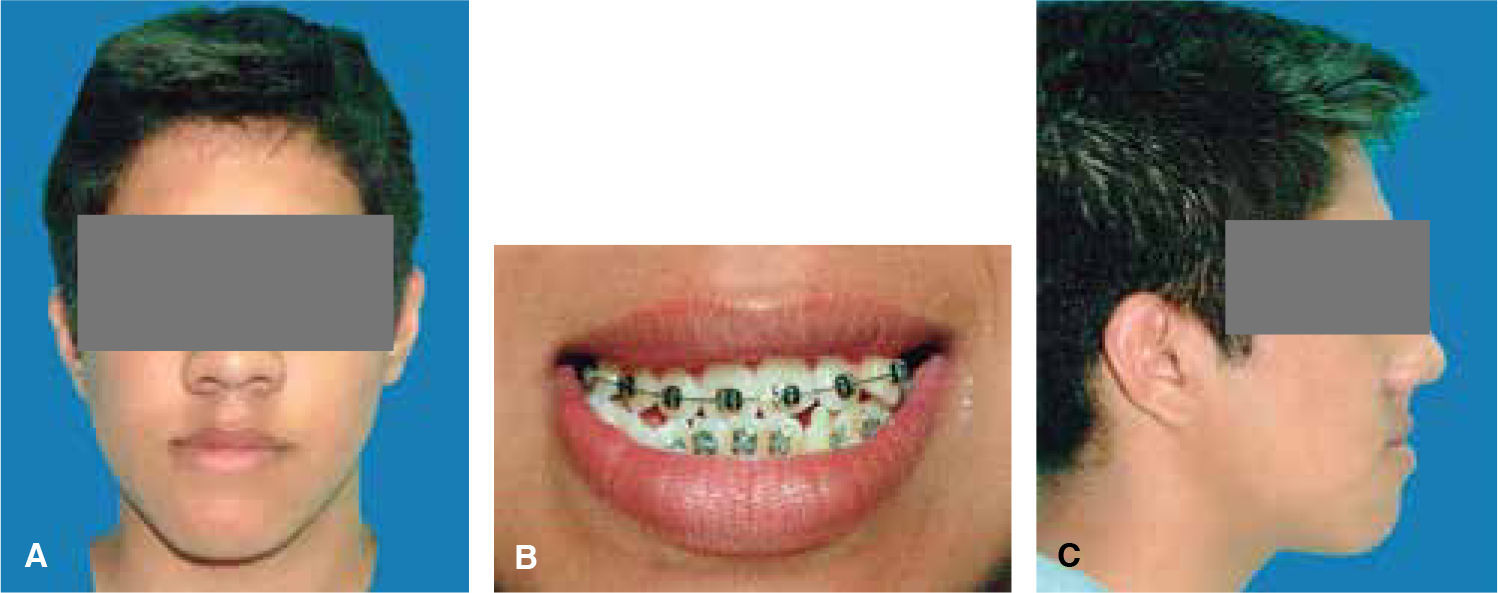
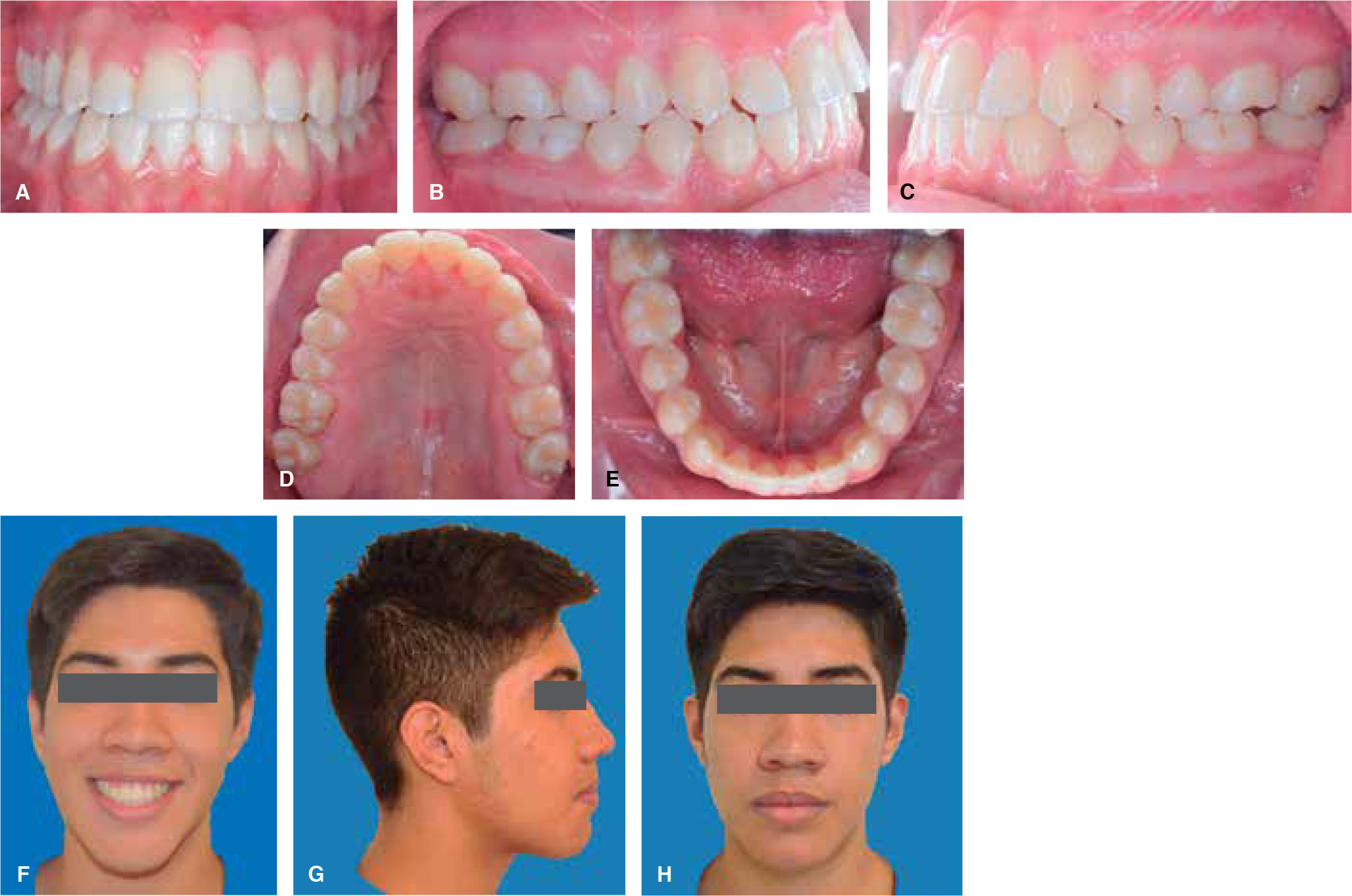
Frontal esthetic analysis: long, oval-shaped face, dolichofacial biotype, low left pupil, deficient paranasal and malar region, increased lower and middle thirds (Figure 1A). The smile photograph revealed the previous fixed appliances, lower dental midline deviated to the right (Figure 1B).
- b)
Profile analysis: concave profile, deficient paranasal region, protrusive lower lip, reduced mentolabial angle, decreased mentocervical distance (Figure 1C).
- c)
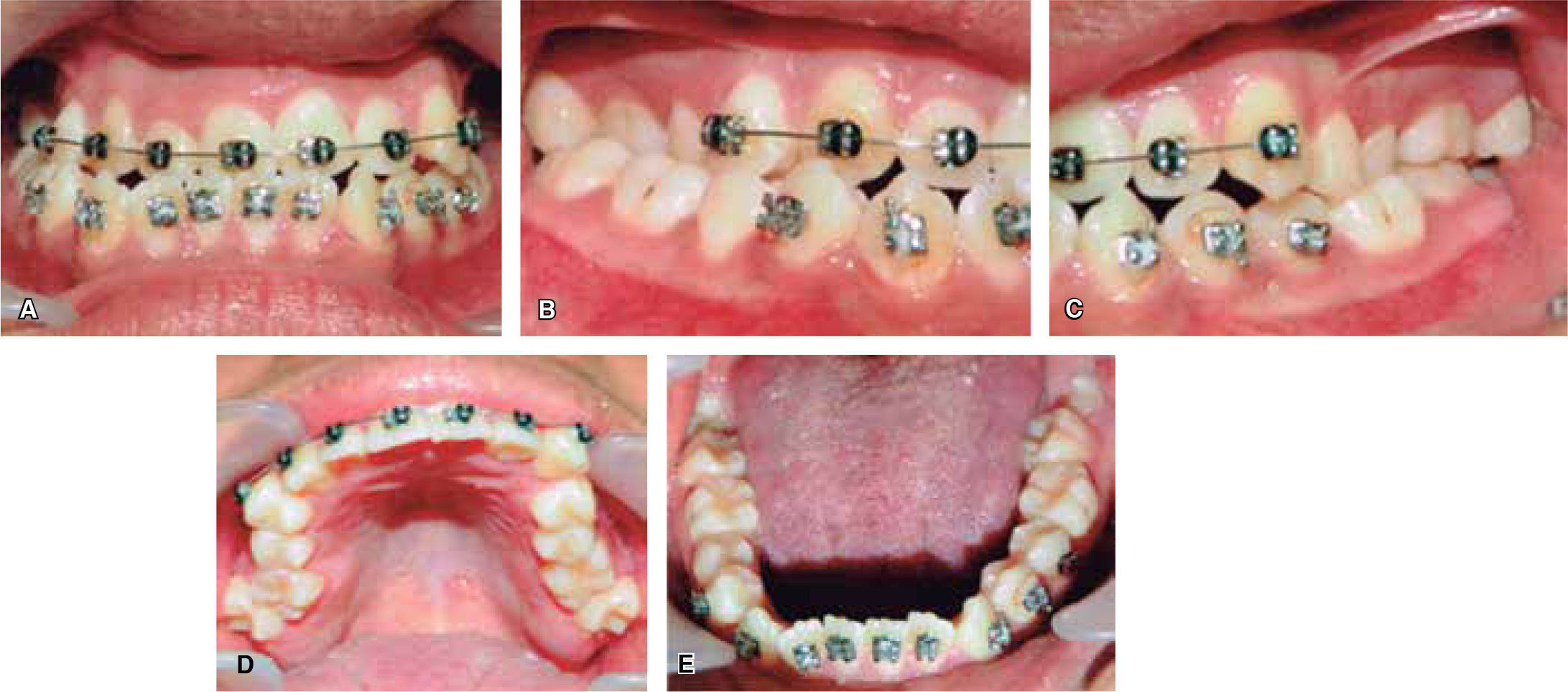
Intraoral analysis: anterior cross bite and bilateral posterior crossbite, lower dental midline 7mm deviated to the right (Figure 2A), molar class III, canine class III (Figures 2B and 2C) irregular and collapsed upper arch form; -8mm arch length discrepancy, ovoid lower arch form, -6mm lower arch discrepancy (Figures 2D and 2E).


Skeletal:
- a)
Anteroposterior: class III due to maxillary hypoplasia and mandibular prognathism.
- b)
Vertical: dolichofacial pattern.
- c)
Transverse: right mandibular laterognathia.
Facial: concave profile, facial asymmetry.
Dental: molar class III, canine class III, anterior crossbite, bilateral posterior crossbite.
Functional: bilateral clicking in the TMJ.
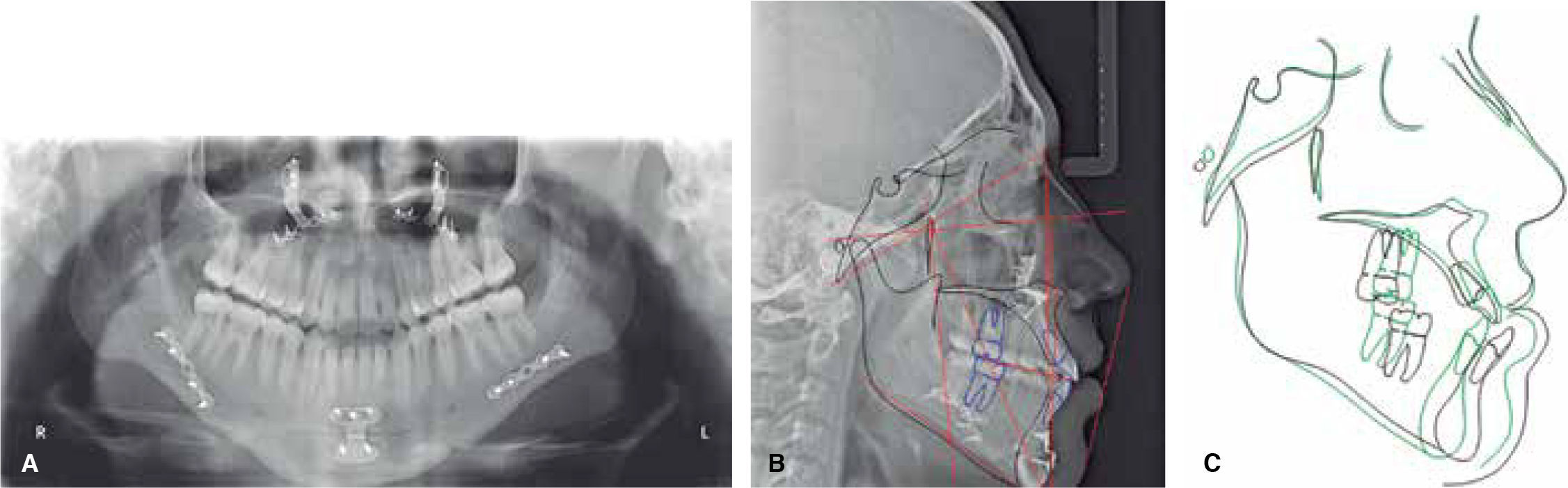
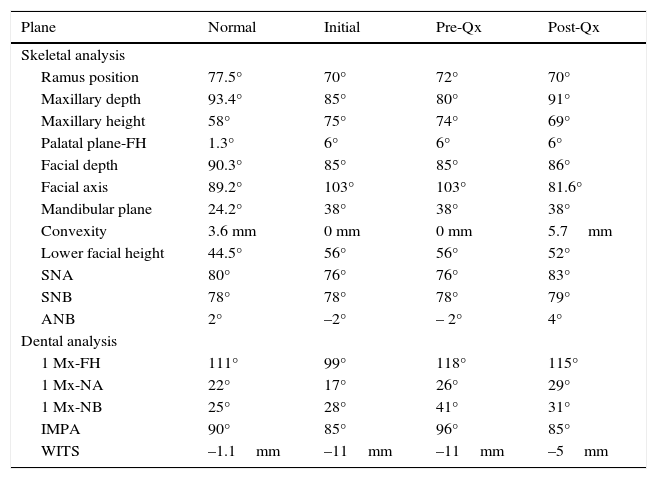
Cephalometric analysisThe initial cephalometric analysis shows a skeletal class III (-2° ANB angle, -11mm WITS) (Figure 3) excessive mandibular growth and a vertical dolichofacial pattern. He presented a lower dental compensation due to lower incisor retroclination (Table I).

Cephalometric values.
| Plane | Normal | Initial | Pre-Qx | Post-Qx |
|---|---|---|---|---|
| Skeletal analysis | ||||
| Ramus position | 77.5° | 70° | 72° | 70° |
| Maxillary depth | 93.4° | 85° | 80° | 91° |
| Maxillary height | 58° | 75° | 74° | 69° |
| Palatal plane-FH | 1.3° | 6° | 6° | 6° |
| Facial depth | 90.3° | 85° | 85° | 86° |
| Facial axis | 89.2° | 103° | 103° | 81.6° |
| Mandibular plane | 24.2° | 38° | 38° | 38° |
| Convexity | 3.6 mm | 0 mm | 0 mm | 5.7mm |
| Lower facial height | 44.5° | 56° | 56° | 52° |
| SNA | 80° | 76° | 76° | 83° |
| SNB | 78° | 78° | 78° | 79° |
| ANB | 2° | –2° | – 2° | 4° |
| Dental analysis | ||||
| 1 Mx-FH | 111° | 99° | 118° | 115° |
| 1 Mx-NA | 22° | 17° | 26° | 29° |
| 1 Mx-NB | 25° | 28° | 41° | 31° |
| IMPA | 90° | 85° | 96° | 85° |
| WITS | –1.1mm | –11mm | –11mm | –5mm |
According to the assessment of clinical, facial, dental and cephalometric data it was decided that the procedure of choice was a surgical-orthodontic treatment in order to achieve the ideal objectives which were: to improve the profile, to obtain molar and canine class I, anterior guidance (overjet, overbite), and arch coordination. 0.022” x 0.028” slot MBT appliances were used with bands in the first and second molars. The discrepancy analysis was performed and afterwards the airways were assessed, as was the mentocervical distance, which appeared decreased so it was decided not to perform extractions.
The orthodontic treatment-surgical was performed in three phases:
Presurgical phaseMBT appliances were placed and in this way the presurgical objectives were met: dental alignment and leveling, eliminate dental compensations, bring incisors into their basal bone, coordinate dental arches, eliminate the curve of Spee and show the real problem of the patient, which was the skeletal class III and the laterognathia (Figure 4). The MBT archwire sequence was followed: 0.012” 0.014” NiTi archwires, 0,016” NiTi thermal, 0.016” x 0.022”, 0.017 x 0.025” NiTi 0.019 x 0.025” NiTi up to 0.019 x 0.025” stainless steel archwires with crimpable hooks placed between each tooth in order to perform intermaxillary fixation during the orthognathic surgery (Figure 5).


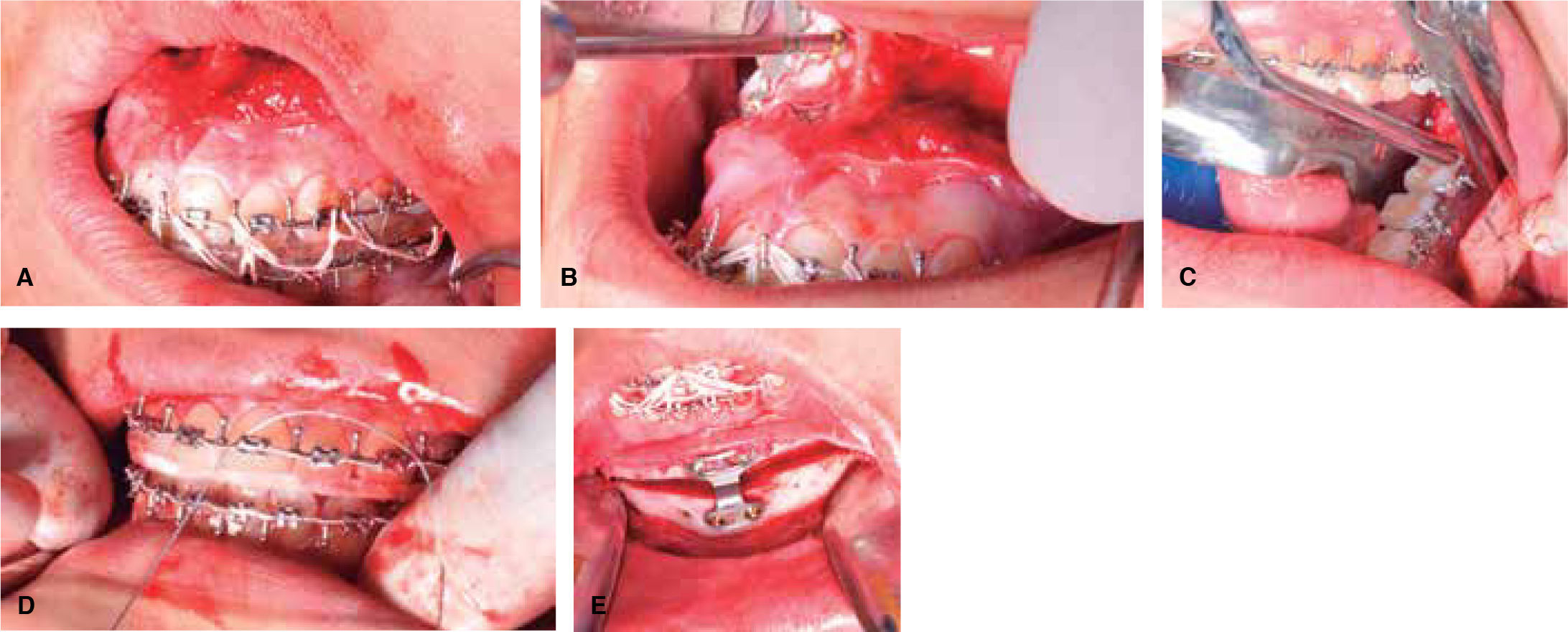
Surgical planning was in charge of the maxillofacial surgeons in collaboration with the orthodontists. Study models were taken in centric relation and mounted in a semi-adjustable articulator in order to perform the surgical prediction, surgery of models and surgical guides.10 A bimaxillary surgery was planned,6 which consisted in a 5mm maxillary advancement to improve the zygomatic deficiency in addition to a 2mm maxillary impaction to reduce the eversion effect generated in the upper lip when the maxillary retroposition is performed. An intermediate surgical guide was used. A mandibular advancement of 4mm with a Dal Pont osteotomy of 7mm was also performed to correct the laterognathia and match the dental midlines with the facial. A final surgical guide was used in order to do this in addition to an advancement mentoplasty of 4mm for better aesthetic and facial results (Figure 6).
Postsurgical phase
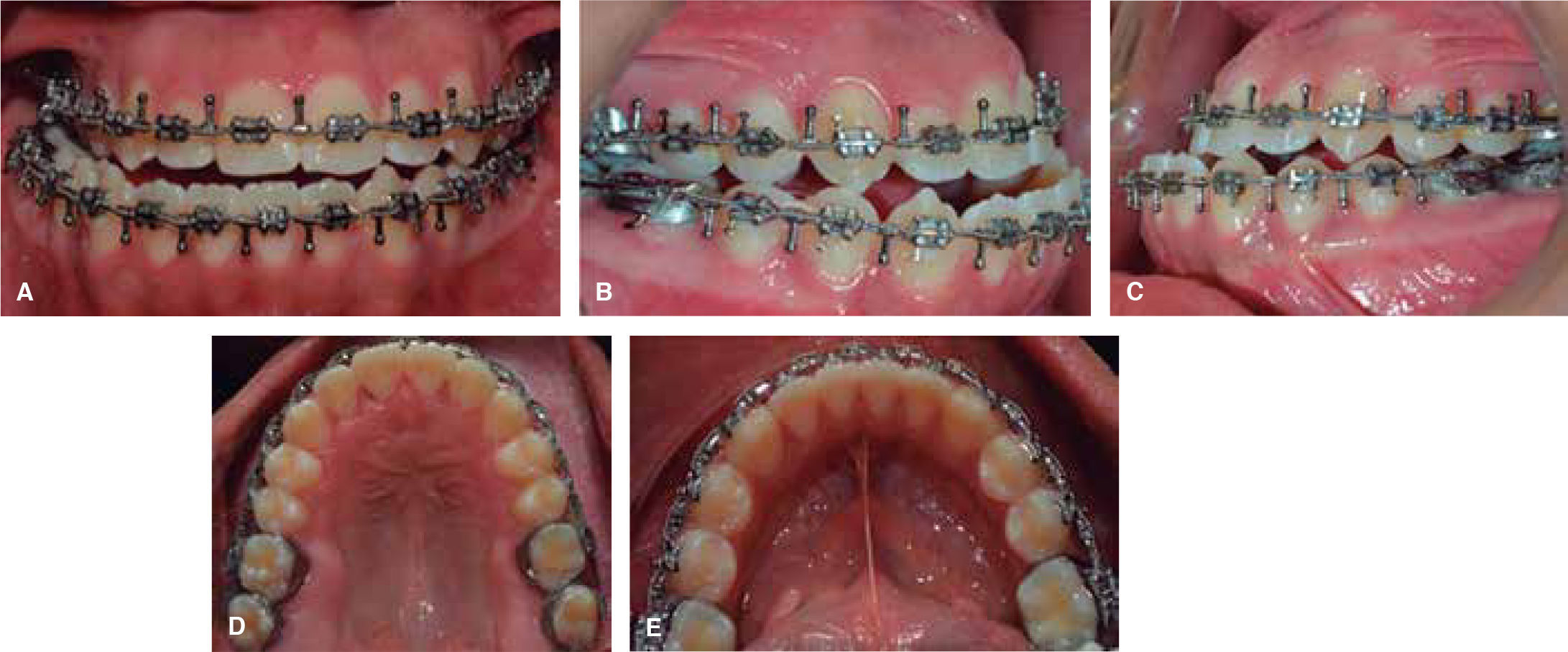
This phase was begun three-weeks after the orthognathic surgery was performed with the aim of taking advantage of the RAP (regional acceleratory phenomenon). 11 0.016” x 0.022” NiTi termal archwires were placed with ¼” 4.5 oz N-shaped settling elastics with a class III vector. For finishing and detailing a 0.019” x 0.022” stainless steel archwire was placed to express the appliance prescription (Figure 7).
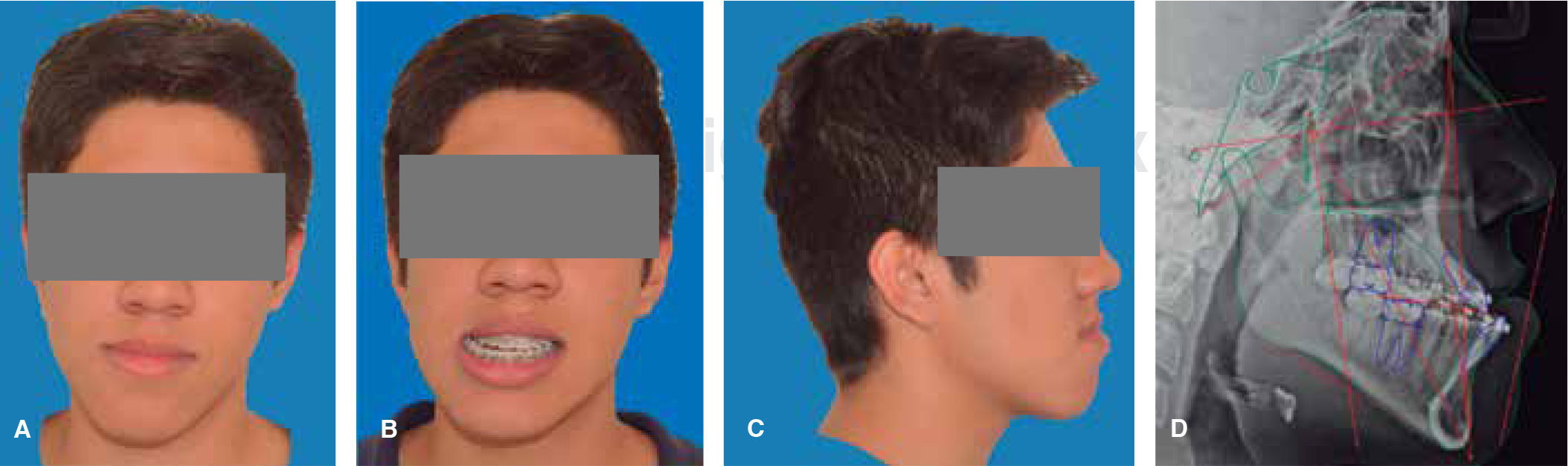
RESULTS
The postsurgical phase was finished six months after the orthognathic surgery because it is the minimum time in which it may be assessed whether there is no relapse after the orthognathic surgery.10 Total treatment time was two years; satisfactory aesthetic and functional results were achieved for the patient; post-treatment photographs show that there a correct facial symmetry was obtained and molar and canine class I was achieved with a good intercuspation and anterior guidance(overjet, overbite). The maxillary and mandibular midlines were coincident with the facial midline. The anterior crossbite and the bilateral posterior crossbite were corrected (Figure 8). An adequate canine and incisor disocclusion guidance was obtained as well as a correct exposure of the maxillary incisors during smile and an excellent facial balance. Upon assessment of the panoramic X-ray an acceptable root parallelism may be observed without the presence of resorptions; there is evidence of the L-plates with 8-millimeter monocortical screws, with good osseointegration. The cephalometric analysis demonstrates the skeletal changes made during: the maxillary impaction and advancement, the mandibular retroposition and the chin advancement to improve facial aesthetics, which is confirmed with the superimposition (Figure 9). For retention and stability of the treatment an upper and lower Hawley retainer was placed to promote occlusal settling (Figure 10).



This skeletal class III malocclusion (ANB angle -2°, Wits - 11mm) was treated with bimaxillary orthognathic surgery with excellent functional and cosmetic results; it was decided not to perform extraction of premolars with the aim of avoiding a decrease in the airway space; it also secured a class I molar and canine relationship with an excellent occlusal settlement. The combination of orthodontics and maxillofacial surgery produces successful results with a high percentage of long-term stability cases and prevents relapse in the future. It is of the utmost importance to start with the postsurgical orthodontics three weeks after the surgical intervention to take advantage of the RAP (regional acceleration phenomenon), hence better intercuspation and midline correction movements may be performed in less time and with better results. Changes in soft tissues after the orthognathic surgery vary individually due to biological differences between patients. These differences include local factors such as (muscle tone, thickness of the soft tissue) and general factors such as age and changes in body weight. It is for this reason that high expectations with the digital surgical prediction should not be made since different aesthetic results may be expected.
CONCLUSIÓNThe success of the treatment of skeletal class III patient depends on a good interdisciplinary relation between the orthodontist and the maxillofacial surgeon in order to establish the preoperative objectives and to plan a correct orthognathic surgery, adapting it to the skeletal and facial needs of the patient. Bimaxillary orthognathic surgery presents greater stability in the long term, besides having better esthetic and functional results.
It is very important to make a correct assessment and an appropriate interdisciplinary diagnosis to be able to implement a correct treatment plan for the patient and try to cover all the objectives, besides obtaining a correct integral health for the patient.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia
Dental Surgeon. Resident of the Orthodontics Specialty, University Center of Health Sciences, University of Guadalajara.
Master in Science. Head of the Orthodontic Specialty University Center of Health Sciences, University of Guadalajara.