












Skeletal anterior open bite may be treated with mini-screws since they provide an absolute anchorage to correct it through maxillary molar intrusion. With an adequate control a bite block was used in this case to help correct the malocclusion.
Case reportA 15 year-old male dolichofacial patient with an Angle class II division 1 malocclusion, a -4.5mm anterior open bite and incompetent lips is hereby presented. Etiology: reduced anterior upper facial height. The treatment goal was to obtain a normal anterior overbite decreasing the posterior maxillary dentoalveolar height. Orthognathic surgery was indicated but the patient refused it. So the treatment consisted in two mini-screws implanted on the palatal side and a modified fixed bite block, activated with elastomeric chains.
ResultsA molar intrusion of 2mm was achieved; the anterior overbite changed to +2mm, a mandibular counterclockwise rotation took place and the facial profile was improved.
ConclusionsThe anterior open bite was corrected with a good control during molar intrusion and without buccal tipping.
La mordida abierta esquelética anterior puede ser tratada con miniimplantes, ya que proveen un anclaje absoluto para corregir mediante la intrusión de los molares maxilares con un adecuado control, en el presente caso se ayudó con un bite block modificado. Se presenta el caso de un paciente de 15 años de edad, dolicofacial, con una maloclusión clase II subdivisión 1, mordida abierta anterior de -4.5mm e incompetencia labial. Etiología: por una altura facial anterior superior disminuida. El objetivo del tratamiento fue conseguir una adecuada sobremordida anterior disminuyendo la altura maxilar dentoalveolar posterior. La cirugía ortognática se le indicó pero fue rechazada. Por lo tanto se realizó una intrusión molar superior con dos miniimplantes colocados en el paladar más un bite block modificado activado con cadenas elásticas.
ResultadosLa intrusión molar superior fue de -2mm, la sobremordida anterior cambió a +2mm, hubo autorotación mandibular y se mejoró el perfil facial.
ConclusionesLa mordida abierta anterior fue corregida con un adecuado control de la intrusión evitando alguna inclinación bucal de los molares.
Open bite is a malocclusion of the vertical plane, due to a lack of anterior contact. It may be of skeletal or dental origin.1 The malocclusion is attributed to a multifactorial etiology since it may be genetic, anatomical and environmental as well as due to the development of pernicious oral habits, The prevalence of anterior open bite is 3.5% (8 to 17 years of age).4 In Mexican population, at early ages, the open bite is related to habits in 96.6% of the cases.5
The open bite patient is characterized by adenoid facies or long face syndrome with lip incompetence caused by incisor proclination and lack of overbite, which when combined with habits cause gingival inflammation.6 The retruded position of the mandible decreases the mentocervical distance and shortens the projection of the chin.2 This mandibular position may also decrease the airways.
To differentiate if it is a skeletal or dental open bite cephalometric analysis are used. A dental open bite is characterized by incisors in infraocclusion, while the premolars and molars are further away from the palatal or mandibular planes, Graber et al. indicates that if their apices are more than 3mm above these planes it may be considered as a supraeruption.7 A larger degree of divergence of the upper and lower occlusal planes indicates the severity of the case.8 Janson et al. reported that the upper and lower molars are more mesially inclined with respect to the occlusal plane, while the apices are accentuated in a distal inclination in relation to the palatal and mandibular plane respectively.9
Among the skeletal cephalometric data, the inclination of the Mandibular Plane will be found increased as well as a downward and rearward inclination of the mandibular ramus, a short mandibular ramus, a more marked antegonial notch and a shortened posterior facial height, which increases the mandibular angle and the anterior facial height.2 If the problem is in the maxilla an increased inclination of the palatal plane will be present due to excess of posterior growth or to poor anterior growth of the maxilla.10 In addition to the vertical analysis of the anterior and posterior facial height, the height of the dentoaveolar processes must be measured as indicated by Sean Biggerstaff et al.11 When a vertical problem is evident in a skeletal open bite, Sassuoni described that the occlusal, palatal and mandibular planes make a closer convergence near the posterior portion of the face.12
Several therapies have been described to correct the skeletal or dental open bite such as functional education of the tongue; extraction of first premolars, second premolars or first molars; high-pull headgear, chin cup, elastics, multi-loop arch wires (MEAW), bite blocks, tongue cribs and functional appliances. In the skeletal open bite orthognathic surgery will always be the standard treatment.8,13–17
In the last decade molar intrusion through the use of mini-implants has been described to correct the skeletal open bite thus causing a decrease in incisor extrusions. It has also been described to provide favorable cosmetic results such as a forward rotation of the mandible and a reduction in anterior facial height. It has even been used as an alternative for patients who have not agreed to orthognathic surgery.18,19
There are different ways to perform molar intrusion with mini-implants, whether placed palatally, labially or in both sides as well as with the help of other appliances.17,18,20–23
In Graber's book it is stated that molar intrusion with mini-implants must be designed to provide threedimensional control of the tooth regarding rotation, inclination, torsion, mesiodistal position and the vertical position molars, in addition to assessing arch form, inclination of the occlusal plane and the frontal occlusal plane. When performed on upper molars, it is very important to consider control over the resistance of the palatal roots.7
In the present case an upper molar intrusion was performed trying to have sufficient control over the first and second molars to achieve adequate results and correct the open bite.
Diagnosis and etiologyA male patient of 14 years and 9 months of age attended the Orthodontics Clinic of the Division of Post-Graduate Studies and Research, UNAM, with the following reason for consultation: «My upper teeth are too forward». Regarding pathological data, the patient mentioned being under treatment for rhinitis. Oral habits: Mouth breathing. The facial photographs showed a convex profile, lip incompetence and poor projection of the chin; the smile photograph revealed an anterior open bite (Figure 1). Upon intraoral examination the patient presented a right molar class II malocclusion, bilateral canine class II, bilateral posterior cross bite (-2mm), anterior open bite (-4.5mm) and spaces between the incisors (Figures 2 and 3). In the panoramic radiograph no caries may be observed, there are good root inclinations and third molars are under development. The analysis of the lateral head film identified a skeletal class II due to mandibular retro position (ANB: 6°, Convexity of Ricketts: 5mm), vertical growth: (SN-PM: 41°, Facial Axis: 83°), dental biproclination (1U-SN: 110°, IMPA: 101°). As etiology it was determined that a poor anterior maxillary growth and an increased posterior maxillary height (N-ENA: 52mm palatal plane: -7°) was the cause of the malocclusion (Figure 4). Through the use of CT cone-beam it may be observed that there is no damage to the cortical bone (Figure 5).
Treatment goals




Facial: to improve the profile, decrease lip incompetence and improve incisor exposure during smile. Skeletal: to correct the skeletal open bite, favor a CCW mandibular rotation and control the vertical dimension. Dental: coordinate arches, achieve molar and canine class I, retrocline the incisors, match midlines, and obtain occlusal contact. Functional: to improve respiratory function through open bite closure.
Treatment alternatives- 1.
Orthognathic surgery: LeFort I surgery for maxillary impaction. The patient did not accept this treatment alternative.
- 2.
Extraction of four first premolars: This would allow the correction but could affect the facial profile in the future, as well as increase the vertical dimension.
- 3.
Intrusion of upper molars through the use of miniimplants: molar intrusion has been reported as the most stable option when it comes to performing a camouflage treatment. To achieve this, it was proposed the placement of 2 mini-implants on the palate between the first and second molars, combined with a device similar to a bite block cemented into the upper molars, which would be activated by elastomeric chains, from the mini-implants to the device. This would allow an intrusion without causing undesirable inclination movements.
Fixed appliances: 0.022” × 0.028” slot Edgewise brackets and tubes.
- 1.
Alignment and Leveling Phase: 0.014”, 0.018” and 0.018” × 0.025” NiTi arch wires.
- 2.
Work phase: Placement of 2 mini-implants (1.8 × 9mm) on the palate between the first and second molars; the bite block was cemented with glass ionomer. The bite block was modified by adding two hooks between first and second upper molar palatally, activation was made with closed elastomeric chains, 3 Oz of force on each side in periods of 3 weeks for 3 months. Afterwards, the bite block was removed and a TPA was placed to maintain the intrusion (Figure 6). Space closure was performed with 0.016” × 0.022” SS arch wires with bull loops.
- 3.
Finishing Phase: Upper and lower 0.018” × 0.025” SS arch wires with second and third order bends; bracket repositioning: 0.016”, 0.016 × 0.025” upper and lower NiTi arch wires.
Detailing: Upper and lower 0.017” × 0.025” SS with ideal bends and 60° progressive lingual torque.
- •
Interconsultation with Periodontics: Phase I (hygiene and control) to treat a moderate plaque- related gingivitis; support and education with the brushing technique. Upper and lower gingivoplasty from premolar to premolar.
Settling: 0.017” × 0.025” braided arch wire in the upper arch, 0.017” × 0.025” SS arch wire with ideal bends plus settling elastics (2 weeks). Fixed appliance removal.
- •
- 4.
Retention: upper and lower circumferential retainer. Lower retention from canine to canine with 0.0175 -twisted arch wire.

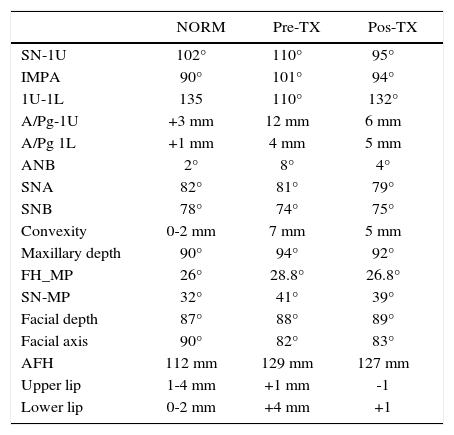
A good alignment and a proper occlusal settlement were achieved. Retraction of the upper and lower incisors was performed thus obtaining a normal overbite and a Class I molar, premolar and canine relationship. A good arch form and an adequate gingival aesthetics were also obtained. Molar intrusion was -2mm, the overbite changed to 2mm thus favoring a mandibular rotation. The facial profile improved, the lip incompetence was eliminated and a better chin projection was obtained. The anterior facial height decreased by 2mm, in addition to a better incisor exposure at smile. Radiographically, an adequate root parallelism may be observed as well as an increase of the airways at pharyngeal level (Figures 7 to 10andTable I).




Cephalometric data.
| NORM | Pre-TX | Pos-TX | |
|---|---|---|---|
| SN-1U | 102° | 110° | 95° |
| IMPA | 90° | 101° | 94° |
| 1U-1L | 135 | 110° | 132° |
| A/Pg-1U | +3 mm | 12 mm | 6 mm |
| A/Pg 1L | +1 mm | 4 mm | 5 mm |
| ANB | 2° | 8° | 4° |
| SNA | 82° | 81° | 79° |
| SNB | 78° | 74° | 75° |
| Convexity | 0-2 mm | 7 mm | 5 mm |
| Maxillary depth | 90° | 94° | 92° |
| FH_MP | 26° | 28.8° | 26.8° |
| SN-MP | 32° | 41° | 39° |
| Facial depth | 87° | 88° | 89° |
| Facial axis | 90° | 82° | 83° |
| AFH | 112 mm | 129 mm | 127 mm |
| Upper lip | 1-4 mm | +1 mm | -1 |
| Lower lip | 0-2 mm | +4 mm | +1 |
In the case hereby presented the goals were to correct an anterior open bite caused by a skeletal problem. According to the analysis of Sean Biggerstaff et al.,11 it was found that the malocclusion was caused due to a growth deficiency of the anterior portion of the maxilla, in contrast to the inclination of the Ricketts palatal plane which showed an excess of maxillary posterior growth. An excess of the posterior portion of the maxilla, at the level of molars causes growth problems in a clockwise direction or a retruded position of the mandible.2
With regard to the mini-implant placement in this case, it was performed as described by Björn et al., who state that for intrusion from the palatal side between the first and second molar, between their palatal roots, 5mm from the marginal crest, there is a space of 4-5mm ideal for mini-implant placement. In this case, a similar placement site was chosen.24
Posterior intrusion with mini-implants to correct an open bite is well described by several authors.1,14–25 Cifter et al using a finite element model for transpalatal (Goshgarian) arch and mini-implants found that there is more intrusion of the buccal roots than the palatal roots.21 When mini-implants are placed only on the palatal side some auxiliary appliance should always be placed to avoid an undesirable lingual crown torque as described by Buschanget and Xun et al.22,23
The applied force in this case was 3 Oz per side by means of elastomeric chains to avoid root resorption. Some cases using NiTi spring coils of 150g per each side have been described.1,22,26 Greater intrusion forces have been presented in cases from Everandi et al with the use of zygomatic mini-plates combining the use of 200g springs.20
The results in this clinical case show that an intrusion of 2mm in the first molar and of 1mm in the second molar are similar to that reported in the studies of Scheffler et al, who determined that for a 2mm intrusion there will be a 4mm overbite.10 Alsafadi et al and Scheffeler et al. indicated that when performing this movement, passive extrusion of the lower molars must be controlled. This may be avoided with the use of miniimplants for intrusion or only as an indirect anchorage and the use of acrylic plates.27 The modified bite block cemented to the first and second molars helped crownroot three-dimensional control during intrusion and prevented lower molar extrusion. Other authors such as Bushang et al. analyzed intrusion performed only with palatal mini-implants using coil springs attached to a palatal expander and the results indicated that the molar intrusion was controlled properly.22
One advantage was that there were interproximal spaces in both the upper and lower arches, which favored the retroclination to consume those spaces (retroclination or retraction of the teeth), thus decreasing the open bite. It also favored lip closure and improved the aesthetics considerably. It should be noted how Daguchi et al. indicated that molar intrusion combined with retraction of the anterior segment, favors significant aesthetic changes due to a CCW mandibular rotation and improves the stability of the case in contrast to performing only incisor and canine extrusion.25,27
Several authors such as Scheffer et al., Härt et al, Kuroda et al, Buschang et al., Xun et al. and Alsafadi et al. stated that the effects of intruding the upper posterior teeth are favorable causing a mandibular rotation of 1° to 4°, hence improving chin projection, decreasing the facial height and the mandibular angle. Similar results were also achieved in the present case but not significantly.18,19,22,23,26,27
CONCLUSIONS- •
Upper molar intrusion mechanics is described as being more stable than extrusion of the anterior teeth for open bite closure.
- •
The use of two mini-implants on the palate combined with a modified bite block provided excellent three- dimensional control avoiding any unwanted upper molar tipping during intrusion.