




Skeletal class III discrepancy has been a therapeutic challenge due to the fact that its therapeutic management seeks not only the correction of the malocclusion but also the aesthetic component of the patient which is affected according to the severity of the discrepancy. Likewise, anterior crossbites are characteristic of skeletal, dental and even functional class III malocclusions and may prevent sagittal maxillary development in growing patients thus becoming a skeletal anomaly. Hence it is important to intercept this malocclusion as early as possible in order to prevent it from transforming into a true discrepancy. This case report discusses the timely intervention of a pseudo Class III malocclusion with the aim of changing the sagittal and vertical position of the incisors to guide and maintain the growth remnant stable towards a Class I dental occlusion in a 13-year-old patient who had previously received orthopedic treatment without a positive result. The case was handled in the clinics of the post-graduate Program in Orthodontics at the Dental School of the Universidad del Valle, Cali, Colombia.
La discrepancia esquelética de clase III ha sido un reto terapéutico debido a que su manejo busca no sólo la corrección de la maloclusión sino también el componente estético del paciente, que se ve afectado de acuerdo con la severidad de la discrepancia. Así mismo la mordida cruzada anterior característica de las maloclusiones clase III tanto esqueléticas como dentales e incluso funcionales puede impedir el desarrollo sagital del maxilar superior en pacientes en crecimiento y desarrollo, convirtiendo una maloclusión en una real alteración esquelética. De allí lo importante de interceptar esta maloclusión lo más temprano posible, para impedir que se transforme en una verdadera discrepancia. El presente reporte plantea la intervención oportuna de la maloclusión de pseudo clase III con el objetivo de modificar la posición sagital y vertical de los incisivos para guiar y mantener estable el remanente de crecimiento hacia una clase I dental en una paciente de 13 años quien había recibido tratamiento ortopédico sin un resultado positivo. El caso fue manejado en las clínicas del Postgrado de Ortodoncia de la Escuela de Odontología de la Universidad del Valle, Cali, Colombia.
Pseudo class III malocclusion, functional bite or false class III malocclusion is a product of an acquired reflex mandibular advancement due to a discrepancy between centric relation (CR) and centric occlusion (CO). In this anomaly a Class III molar relationship is found in centric occlusion and a Class I in centric relation, i.e. there is mesial mandibular displacement to achieve the greatest number of contacts and muscle relaxation. In growing patients it may give raise to a true skeletal class III, if not corrected in due course.1,2
Premature contacts at incisor level may result in a forward movement of the mandible in pseudo-class III malocclusions in order to disengage the incisors and allow closure with the posterior teeth.3
Early loss of primary molars can also cause mandibular displacement, due to changes in the occlusal guide of poorly aligned teeth or to the lingual inclination of the maxillary incisors. It has been found a statistically significant correlation between the lack of maxillary teeth such as agenesis of the lateral incisors, maxillary hypoplasia, pseudo Class III, and impacted canines.4,5
The characteristics of class III malocclusions have been well documented and described in the literature finding a wide combination of dentoalveolar and skeletal components. Among the skeletal components there are: maxillary hypoplasia, mandibular prognathism and macrognathia or a combination of both. Among the dentoalveolar components one may findproclined maxillary incisors and retroinclined mandibular incisors as a dentoalveolar compensation. With regard to pseudo class III malocclusions many of its features have been misunderstood through the years. Tweed6 classified class III malocclusions into two categories: category A and category B, where category A was defined as a pseudo-class III malocclusion with a conventional mandibular shape. For his part, Moyers7 suggested that pseudo class III malocclusion was a bad positional relationship caused by an acquired reflex.
With this in mind, pseudo class III malocclusion has been defined as a functional anterior crossbite due to a mesial mandibular displacement.
The influence of genetics in the etiology of this dysplasia has been widely reported; studies of craniofacial relationships in twins have supplied useful information concerning the role of genetics in this malocclusion. Thus, Markowitz quoted by Da Silva in 2005 points to the existence of a polygenic transmission not linked to gender that has been proven in a study of 15 pairs of identical twins and seven fraternal twins. Fourteen identical twins exhibited the same Class III malocclusion and in fraternal twins, only a couple presented malocclusion.4
EtiologyDifferent etiologic factors have been suggested by Giancotti et al,8 for pseudo-class III malocclusion:
- 1.
Dental factors:
- a.
Ectopic eruption of maxillary central incisors or canines.
- b.
Premature loss of deciduous molars.
- 2.
Functional factors:
- a.
Abnormal position of the tongue.
- b.
Neuromuscular factors.
- c.
Airway or nasal-respiratory problems.
- 3.
Skeletal factors:
- a.
Slight transverse maxillary discrepancy.
- a.
When in centric relation, the incisors have an edge - edge relationship.
- b.
The mandible is normal in size and length.
- c.
The upper incisors are retroclined and the lower are protruded or in a normal position.
- d.
In centric relation the patient's profile is straight and at rest it is slightly concave.
- e.
Class I molar relationship in centric relation and class III in maximum intercuspation.
The ideal moment to treat patients who have been diagnosed with a pseudo class III malocclusion varies according to the dentition, severity and facial features of the patient, but early treatment in patients with mild to moderate anterior crossbite who exhibit normal characteristics in their skeletal relations is essential to prevent the malocclusion from turning into a well-established skeletal class III anomaly.10
Most treatments begin in early stages of the late deciduous or early mixed dentition and end in the permanent dentition. For Dr. Thilander,11 treatment must be initiated in the deciduous dentition and it should be aimed at treating the origin of the malocclusion or the interference that caused the mandibular displacement. In the case of abnormal teeth inclinations devices that improve dentoalveolar incisor inclination and overbite and overjet relationships should be used.12
Treatment strategiesThere are different alternatives for the therapeutic management of pseudo-class III malocclusions, particularly those focused on an orthopedic approach and dentoalveolar inclination.13 These include: acrylic inclined plane, active expansion plates, plates with Escher or progeny arches, Planas tracks and two by four orthodontic mechanics such as the utility or protrusion archwire.8,14–16
From anorthodontic management point of view, there are few case reports in the literature for pseudo-class III malocclusion. An accurate clinical, radiographic and functional diagnosis will result in asuitable biomechanical management of the case.17
CLINICAL CASEFemale patient, thirteen years of age, without any relevant data on her medical history, attends the School of Dentistry at the Del Valle University for Orthodontic consultation. Upon questioning for her chief complaint, she replied: «Because I have an inverted overbite».
Upon clinical examination, she did not show any disease that would be a contraindication for orthodontic treatment. As for her dental background, the patient had received in her early years slow maxillary expansion treatments with removable appliances, Planas tracks and progeny arches.
Physical and clinical examination revealed a normal growth and development for her age, a brachyfacial biotype, a decreased lower third, a normal smile line, facial midline coincident with the dental midlines, concave profile, increased nasolabial and flat mentolabial angles. Her lips were incompetent at rest and the lower lip was everted (Figure 1).

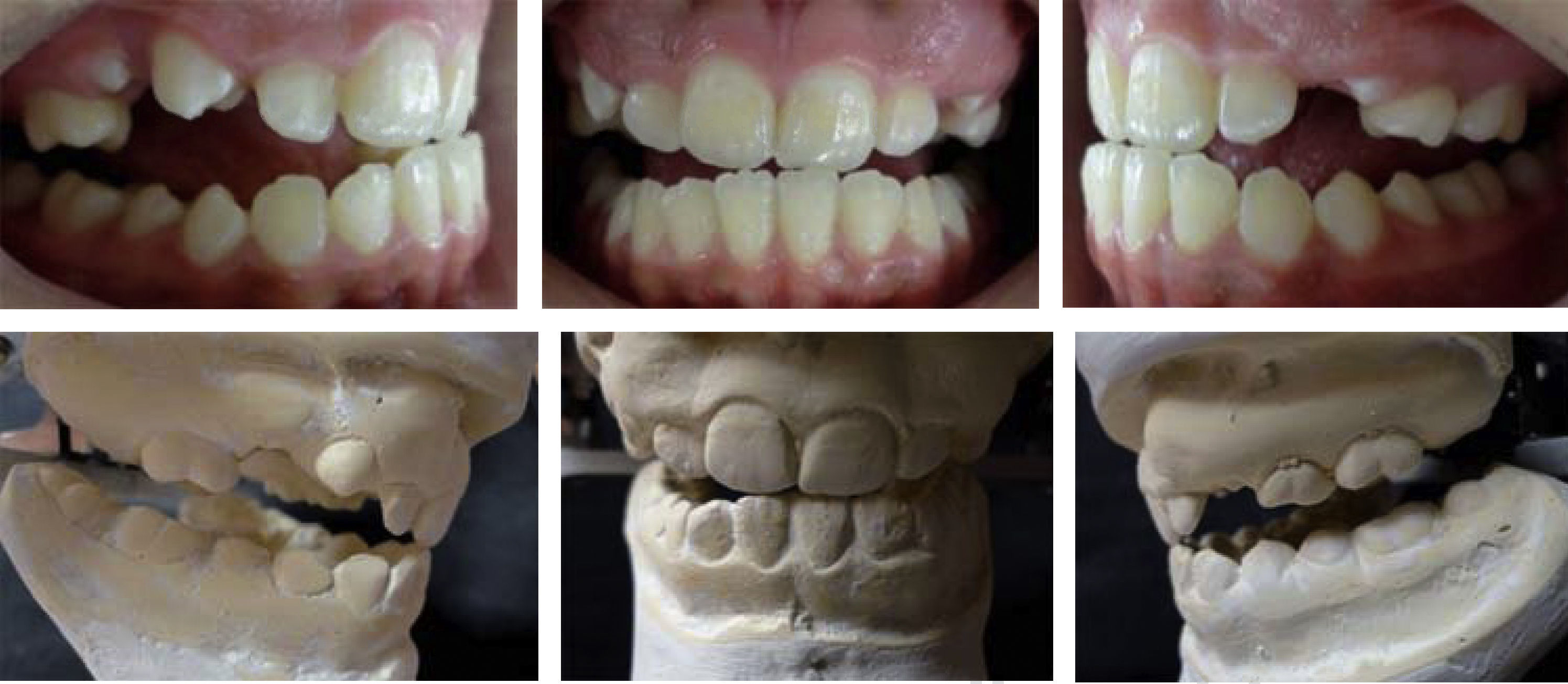
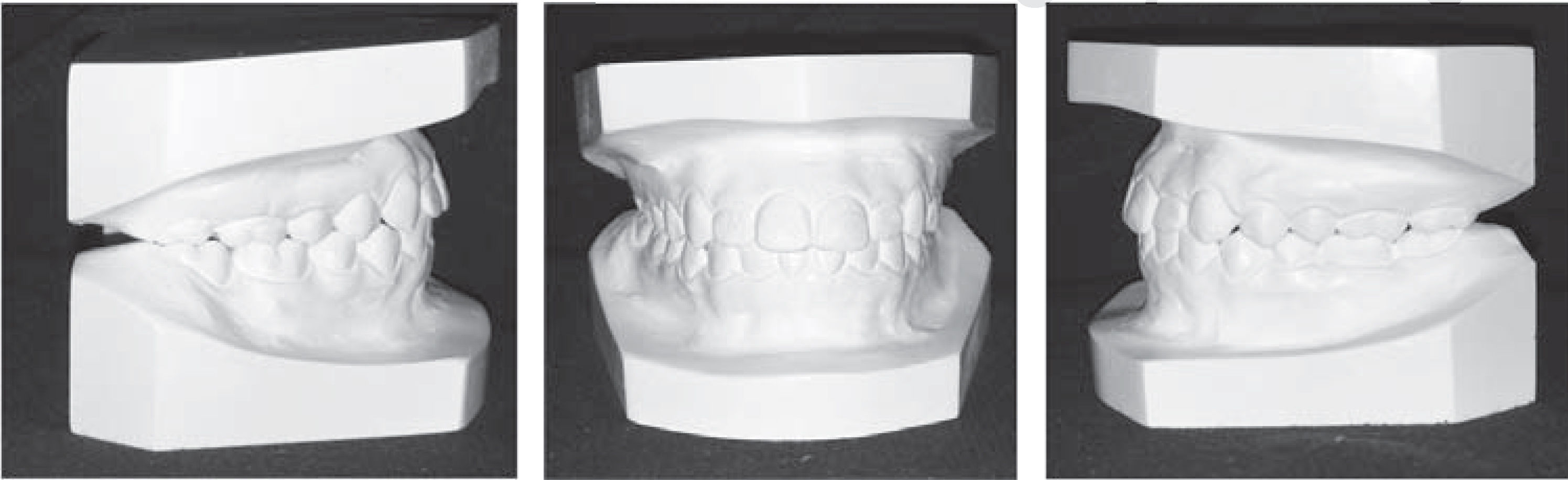
Upon intraoral examination a permanent dentition is observed in the lower arch and an early mixed one in the upper arch. The anterior cross bite had a -4mm overjet and the curve of Spee was pronounced in the lower arch with incisor extrusion. The molar relationship was class III in maximal intercuspation and the crowding was mild on the lower arch and severe in the upper.
Functional analysis revealed a history of oral breathing and when manipulating the mandible a discrepancy between centric relation and maximal intercuspation was observed with a sagittal deflection of 3mm and a vertical one of 7mm. With mandibular manipulation the occlusion was edge to edge with posterior infraocclusion and molar class I. In maximal intercuspation the overjet was -4mm with and a 70% overbite with an Angle molar class III (Figure 2).
Study models analysis
In the assessment of the articulated models, it became evident that there was a deflection and a discrepancy between CR and CO. Different analyses were performed such as Moyers18 and Pont19 analysis. Moyers analysis revealed a -13.2mm discrepancy between the required and the available space for teeth to erupt in the upper arch and with Pont analysis, a slight transverse narrowness was found in both arches. The other teeth were in a percentile of large teeth. Bolton analysis was not performed because the rest of the permanent teeth had not yet erupted (Figure 3).
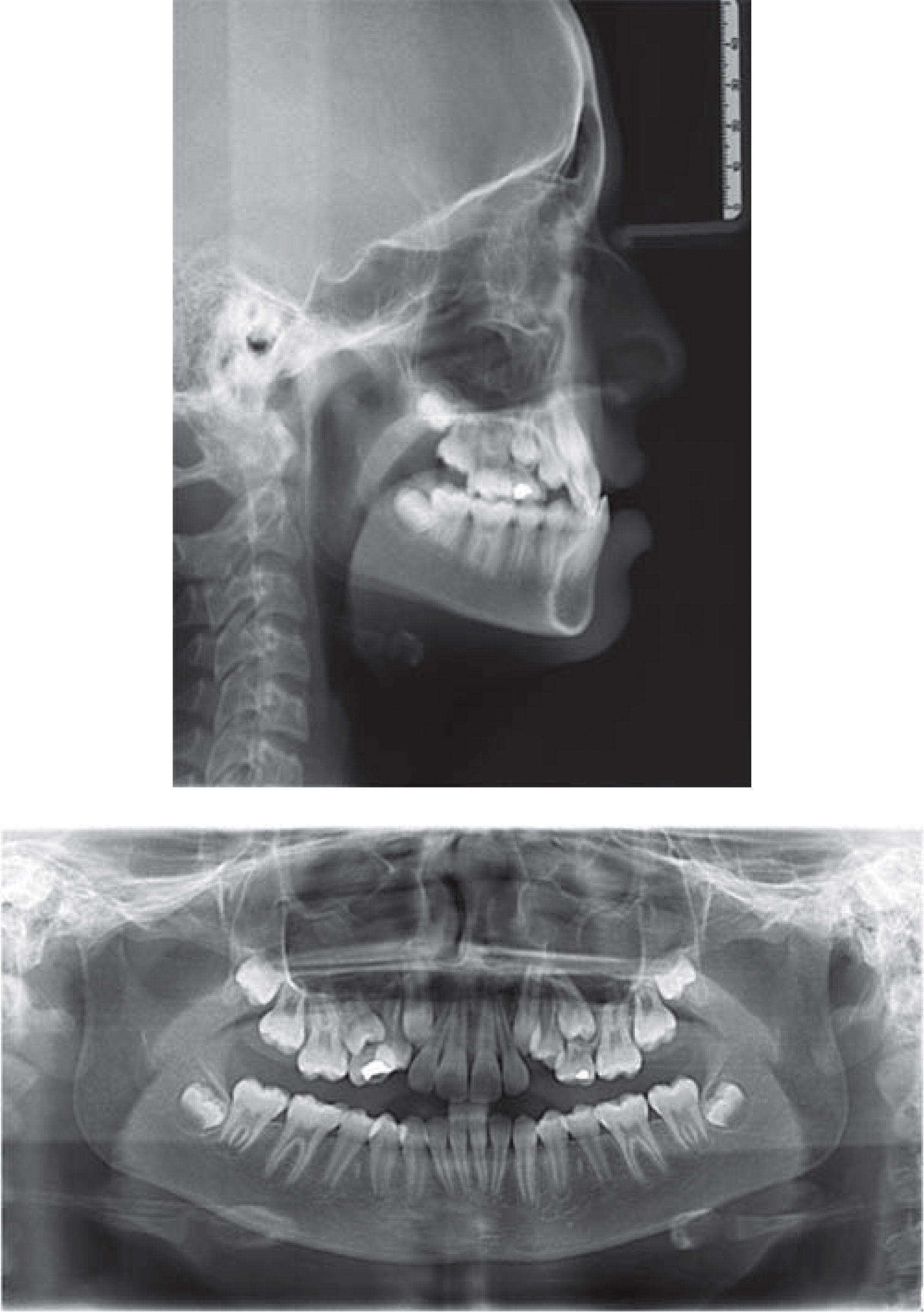
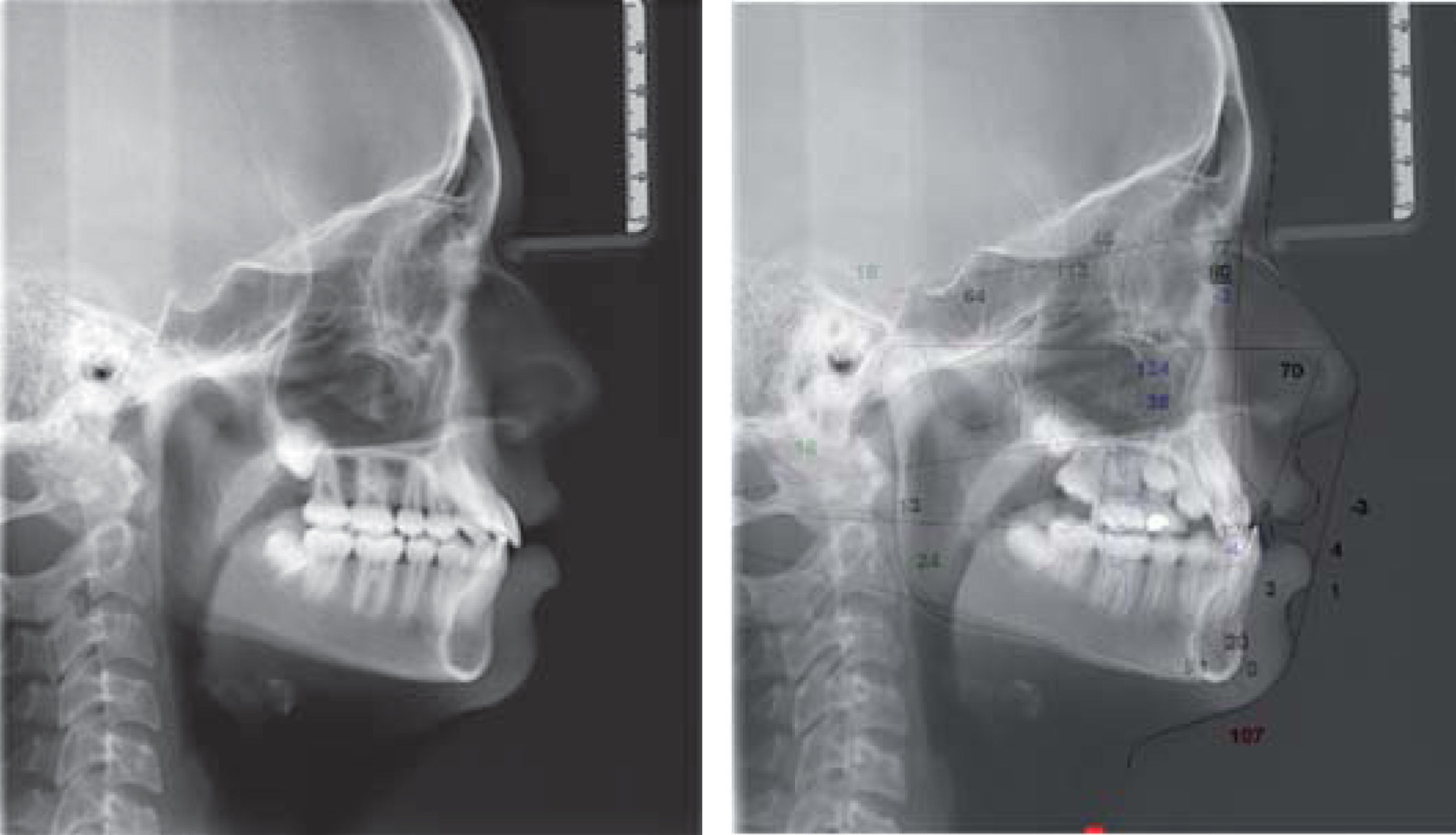
Radiographic analysis
In the panoramic radiograph rounded condyles, short mandibular ramus, normal bony trabeculae, well defined cortical of maxillary sinuses and mixed dentition were observed. The upper left and right canines had no space to erupt and were diagnosed as being in a stage 9 of Nolla. The upper and lower third molars were in stage 6 of Nolla.
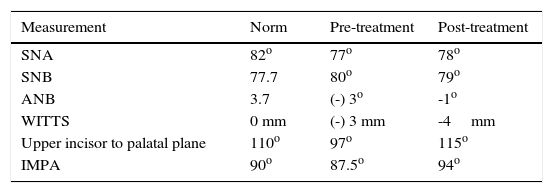
Cephalometric analysis revealed an increased cranial base angle which indicates posterior growth of the cranial base. The maxilla had a mild sagittal retroposition (SNA 77°) and McNamara's perpendicular to point A was at -1mm. The mandible had a normal ramus and a body length and it was properly positioned in the sagittal plane (SNB 80°).Vertically the gonial angle was decreased thus indicating a forward and upward mandibular rotation. Regarding the intermaxillary relationship, the Convexity Angle was -2mm which resulted in a concave profile and sagitally there is a maxillo-mandibular difference of -3mm according to WITS appraisal.20 The lower incisors were almost within normal values (87°) and the upper were severely retroclined (97°). Anterior Facial Height was reduced at the expense of the lower third considering, however, the fact that the radiographic analysis was carried out in maximal intercuspation. The soft tissue analysis shows anincreasedmentolabial fold and an obtuse nasolabial angle (112°) (Figure 4).
Diagnosis
Pseudo-class III intermaxillary sagittal relationship with vertical and sagittal mandibular deflection. Mild maxillary retrusion, brachifacial biotype, concave profile, lower procheilia and retroclined upper incisors.
Treatment goalsTo correct the anterior crossbite in order to allow the normal development of the maxilla, to correct the upper incisorretroclination and retrusion, to make space for upper canine eruption and to achieve a functional and stableocclusion.
Treatment alternativesTreatment of dentoalveolar anomalies of the pseudo class III malocclusion varies according to the orthodontist's preferences and clinical experiences, but primarily it seeks to improve the incisor inclinations that were affected by the intermaxillary vertical relationship which poses the therapeutic challenge to open the bite before correcting the overjet. In this case, the initial diagnosis allowed us to intercept the malocclusion to provide a normal sagittal development of the maxilla in 13-year-old patient thus avoiding a possible orthognathic surgery at the end of her growth period.
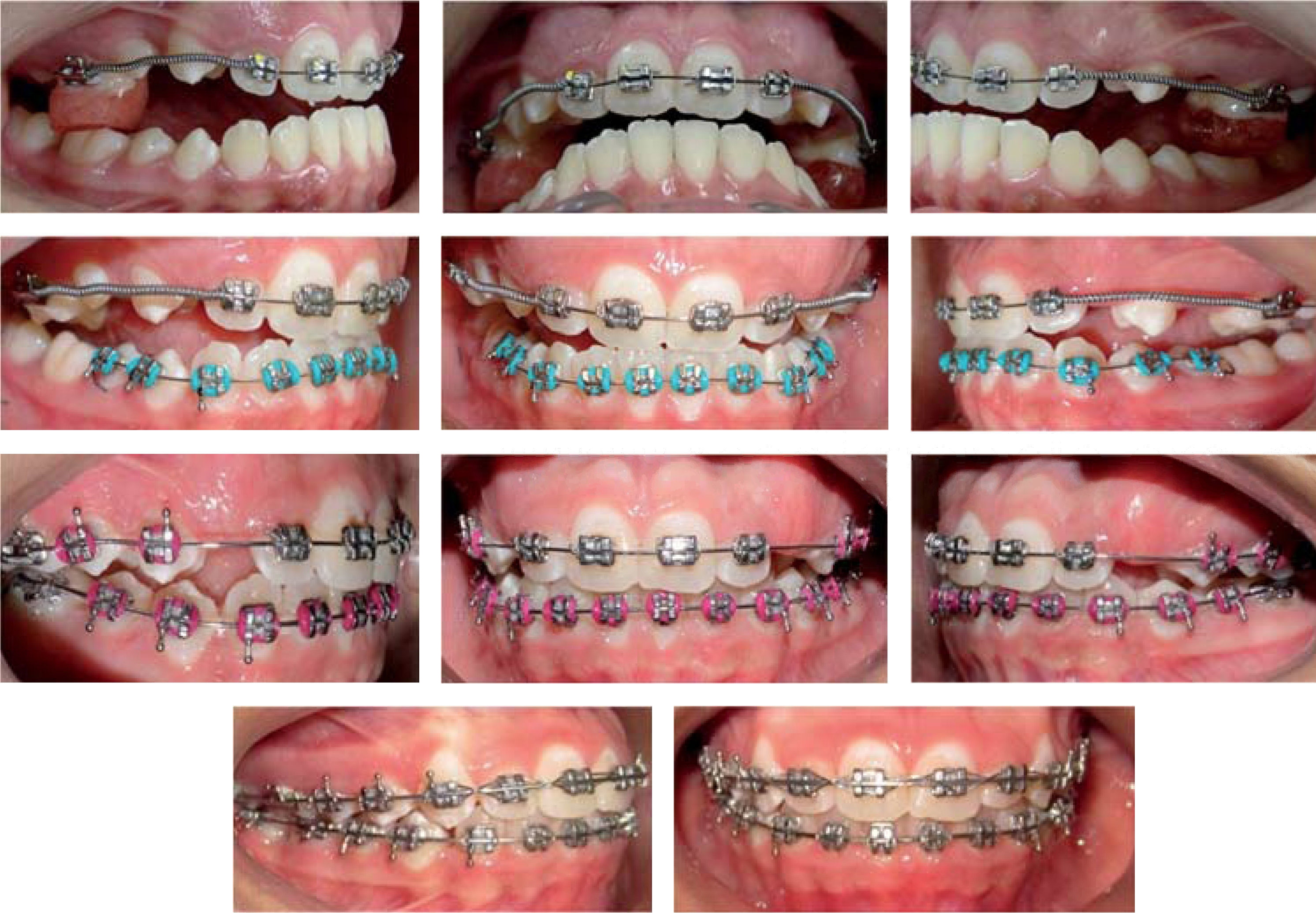
Treatment plan and progressThe first stage of treatment consisted of using a two by four mechanics with bonded tubes on teeth number 16 and 26 and MBT prescription brackets (3M) in the upper incisors. Active coil springs were placed bilaterally from first molar to lateral incisors with 0.018” Australian archwires to open spaces for the eruption of teeth #13 and 23 and also to achieve the protraction and proclination of the upper incisors. In order for the movement to be effective, the overbite needed to be corrected, therefore 7mm acrylic blocks made during the articulator mounting in centric relation were cemented to the first upper molars on each side allowing the bite to and keeping the patient in this position (Figure 5).

After achieving a positive overjet, brackets were placed in the lower arch starting the alignment and leveling phases with 0.014”, 0.018”, 0.017” × 0.025” and 0.019” × 0.025” Nitinol archwires. As the teeth erupted they were gradually incorporated into the mechanics and finally, 0.019” × 0.025” stainless steel archwires were placed in the upper and lower arch. There was no traction mechanics for the canines, the space was generated with orthodontic mechanics only and their eruption occurred spontaneously.
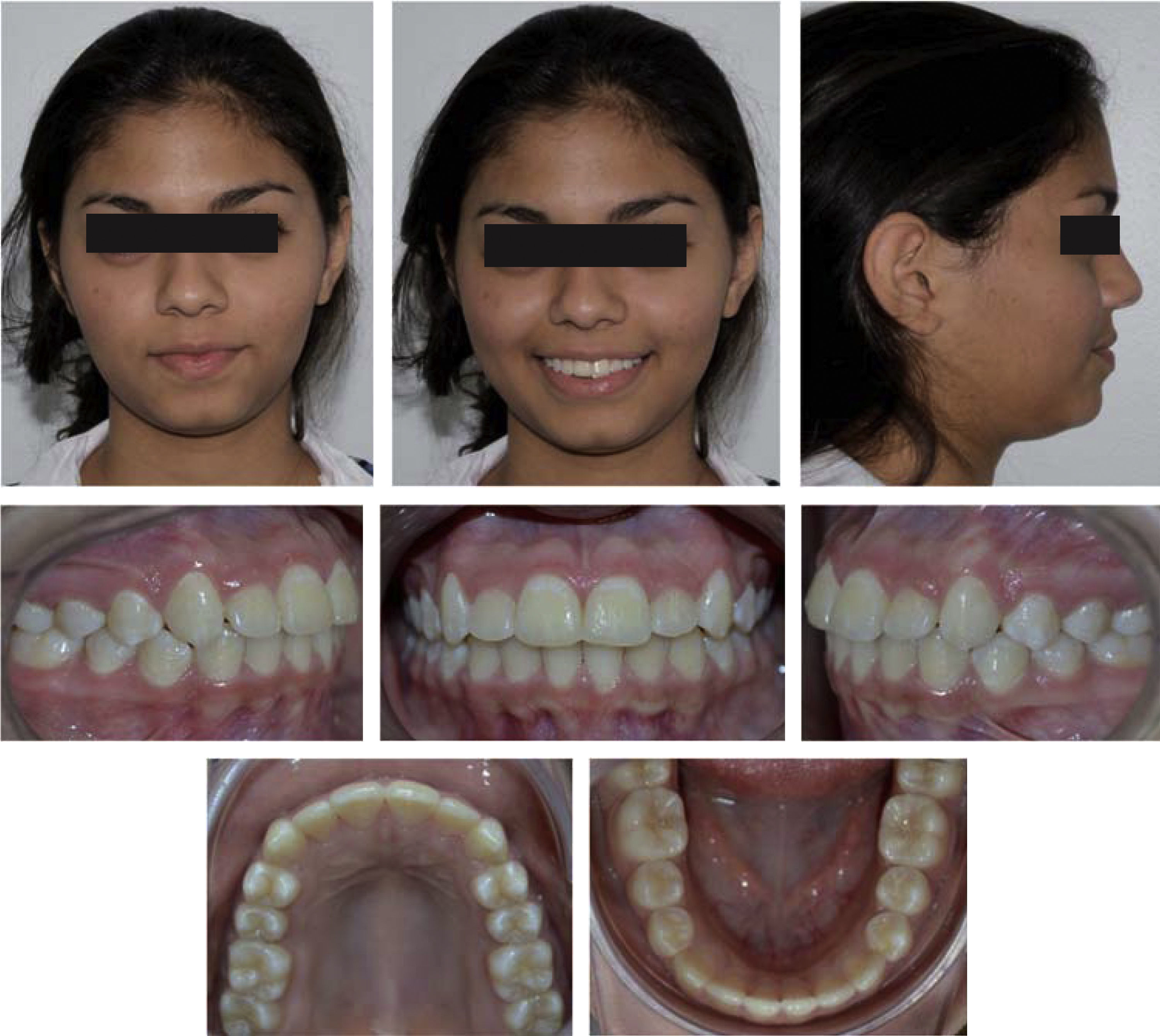
After orthodontic treatment was finished, circumferential removable retainers were placed with acrylic tape from 3 to 3 and Adams hooks at the level of the lower first molars. An assessment of the obtained results was made and the patient was 100% satisfied with the obtained results (Figures 6 to 8).



The patient attended her follow-up visits every 6 months during the first two years after treatment. No significant clinical or radiographic changes were noted and she will be scheduled for an annual control during three years.
DISCUSSIONThis case report shows a satisfying correction of a pseudo-class III malocclusion in a thirteen-year-old patient in whom early diagnosis and the right therapeutic decisions for bite opening helped achieve the treatment goals. The two by four appliance offers the versatility of having mechanical options to correct the pseudo-class III in a predictable manner, due to the fact that the mechanical system can be designed to produce the exact amount of labial dentoalveolar movement of the upper incisors.
Early treatment of the pseudo-class III malocclusion did not only eliminate the discrepancy between the mandibular position in centric relation and in maximum intercuspation21,22 but also increases maxillary arch length, which promotes a Class I eruption of the canines and premolars. This new occlusal relationships favors maxillary growth and prevents the mandibular trap that guides the teeth towards a true skeletal Class III malocclusion.23–25 Therefore, dental correction has a secondary skeletal benefit that contributes to occlusion stability and intermaxillary relationships. Studies such as those of Anderson and Bendeus15,26 show that in patients with anterior crossbite treated with two by four mechanics, point A may grow sagitally up to 4.5mm during growth remnant which indicates that early correction creates a healthy environment for maxillary growth.
Another important advantage of choosing interceptive orthodontic treatment is that it is non-invasive and avoids a possible orthognathic surgery in the future that in addition to its risks, requires the patient to wait until growth has been completed; with aesthetic deterioration as a consequence and the psycho emotional issues that the it entails.
CONCLUSIONDifferent appliance designs and therapeutic managements have been mentioned through time, from orthopedics to intraoral devices for early correction of pseudo-class III malocclusions.27–29 No matter what technique is performed, important treatment points are: 1) to establish a correct diagnosis in order to differentiate it from a real skeletal class III; 2) diagnosis should be as detailed as possible and 3) early intervention has favorable cost-benefit ratios. The stability of the correction may depend on a favorable post-treatment growth.
To Dr. Adriana Herrera, radiologist who from her imagenology centre helped with the cephalometric tracings and superimpositions.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia