






To undertake characterization of patients requesting periodontic specialty care.
Material and methodsThe present was a descriptive study which included all patients registered to receive dental care in a population of the Quinta Region in Chile. Data were grouped according to male and female gender, as well as age range. The following was recorded: presence or absence of tobacco use habit, type II diabetes mellitus (DM), admission to periodontal treatment, treatment desertion and admission to post-treatment periodontal therapy (PTPT). For statistical analysis of frequency differences χ2 test, alpha 0.05, confidence level 95% potency 80% and t student test were used, assessing differences according to age and gender.
Results110 patients requested treatment: 75 female and 35 male. 94% were admitted in the specialty program. Average age was 41 years (SD 15). During the one-year follow-up, 68% of patients remained in treatment, and 19% was admitted in PTPT. Type II DM rate was 4% for females and 31% for males (p<0.001). Patients in age range 14-29 years were more prone to abandon periodontal treatment. With respect to type II DM differences were statistically significant in average age, 39.5 (SD 15.3) years (p=0.002) and average age for desertion 33.2 (SD 17.7) years (p>0.001).
ConclusionsWomen were more inclined to attend periodontal treatment than men, young patients deserted treatment more frequently. Studies on both genders revealed that males exhibited greater rate of type II DM. Additionally, diabetic patients were younger in average age as well as in average age for desertion of periodontal treatment.
Realizar la caracterización de los pacientes que solicitan atención de especialidad en periodoncia.
Material y métodosEstudio descriptivo que incluyó a todos los pacientes inscritos para recibir atención odontológica de una población de la Quinta Región de Chile. Los datos se agruparon de acuerdo con el sexo femenino, masculino y rango de edad. Se registró ausencia o presencia de hábito de tabaco, diabetes mellitus (DM) tipo 2, ingreso a tratamiento periodontal, abandono de tratamiento e ingreso a terapia periodontal de mantenimiento (TPM). Para el análisis estadístico las diferencias en la frecuencia se determinó con χ2, alpha de 0.05, nivel de confianza de 95%, potencia de 80% y t Student evaluando diferencias en la edad, sexo femenino y sexo masculino.
ResultadosSolicitaron atención 110 pacientes, 75 sexo femenino y 35 sexo masculino, ingresaron a la especialidad el 94%. La edad promedio fue de 41 (DE 15) años. Durante el seguimiento por un año, el 68% se mantuvo en tratamiento y el 19% ingresó a TPM. La tasa de DM tipo 2 fue de 4% en mujeres y 31% en hombres (p<0.001). El rango de edad entre 14 a 29 años abandonó más el tratamiento periodontal. En relación con la DM tipo 2 las diferencias fueron estadísticamente significativas en la edad promedio, 39.5 (DE 15.3) años (p=0.002) y edad promedio de abandono, 33.2 (DE 17.7) años (p>0.001).
ConclusionesLas mujeres asisten más a tratamiento periodontal que los hombres y las personas jóvenes abandonan más el tratamiento. Al estudiar ambos sexos, masculino y femenino, los hombres alcanzaron un mayor porcentaje de DM tipo 2. Además el paciente diabético demostró ser más joven en edad promedio y en edad promedio de abandono de tratamiento periodontal
In the pursuit of an ideal periodontal assessment, the professional operator must be aware of the characteristics of those patients he is going to treat, or patients who are going to receive health coverage. It is therefore important that he avails himself to knowledge on patients’ non-modifiable individual determinants such as age and gender, descriptive factors which can exhibit differences in a population.1–4 As a second step, risk factors should be assessed; exposure to risk factor might increase possibilities of contracting disease.3,5 All the aforementioned will finally build up a characterization which might guide towards care that is pertinent to the population's reality.
It is meaningful to note that among men and women there are behavioral physiopathological differences as well as in dental services use and follow-up.4,6,7 As they advance in age, patients face different challenges; among them we can count susceptibility to periodontal disease (PD).8,9 The current concept is based upon the degree of inflammation and bone destruction of periodontal tissues during old age which will be a reflection of the onset, development and progress of PD along time.10 Periodontal risk factors such as tobacco consumption and diabetes mellitus (DM) will be influential factors.2,3,8,9,11–13
In the Petorca province of Chile's Fifth Region (Quinta Region de Chile) no research had been conducted on periodontal patient characterization, since it had only recently been added to dental specialization. The objective of the present study was to achieve characterization of patients requesting periodontal care, the determination according to age range and gender of the number of patients with type II diabetes mellitus (DM), tobacco use, admission to treatment, treatment desertion, as well as follow-up with post-treatment periodontal therapy (PTPT). With respect to type II DM, the following was assessed: average age, number of admitted patients and treatment desertion, presence of type II DM and tobacco consumption, finally age range and desertion of periodontal treatment.
2MATERIAL AND METHODSThe present was a descriptive study. All patients registered to receive dental treatment at the Hospital San Agustin de La Ligua were included. This hospital counts with inter-consultation for periodontal specialty from primary level onwards.
At the first clinical session, patients were requested to sign an informed consent form. Data were recorded in an excel database computer program. Admission was conducted through PSR basic periodontal examination14 as well as full periodontal chart executed by a periodontics expert (PE).
Cases of periodontitis associated to plaque and initial chronic periodontitis were discarded, since treatment of those was directed to the hospital's primary dental care facility before initiation of this research project, two general dentists were trained in the fields of examination, diagnosis and periodontal treatment requirements so as to ensure that all patients were treated without complications. It is worth mentioning that the present study did not analyze relationships between characterization, diagnosis and periodontal treatment requirements of specialty patients.
Data were grouped according to male and female gender, age range (14-29 years, 30-45 years, 46-61 years 62-77 years). The following information was recorded: admission to periodontal treatment, desertion from periodontal treatment, admission to PTPT during a follow-up year, absence or presence of tobacco consumption, and finally absence or presence of type II DM, according to medical charts. Aforementioned diagnosis was corroborated at the Hospital's Internal Medicine Service according to the following parameters: glucose test in fasting patient,≥126mg/dL, obesity (BMI≥27kg/m2), hypertension (≥140/90mmHg), HDL≤35mg/dL and or triglycerides≥250mg/dL, plus previous examination of glucose intolerance while fasting.15
For statistical analysis, frequency differences were determined with χ2 test, assuming the following: 0.05 alpha, 95% level of confidence, and 80% potency. Additionally, Student t test was used to assess differences in age, male and female genders.
3RESULTS110 patients (75 female, 35 male) requested service at the Periodontics Specialty Department. All patients were seeking specialty treatment which included the following in the periodontal treatment: oral hygiene motivation and instruction, teeth cleansing, root scraping and smoothing. 104 patients (94%) were admitted at the Periodontics Specialty Service, 6 (6%) decided not to participate in the study. Average age was 41 years (SD 15). 21 patients (19%) were admitted to post treatment periodontal therapy (PTPT) (Table I). During follow-up, when it was enquired through the telephone why patients had discontinued treatment, 24 patients expressed that they lacked sufficient time, and that it was more feasible to conduct periodontal treatment at later hours or through a resoluteness program; 8 patients informed that they were only interested in the primary reason for their consultation and 3 patients had left the city.
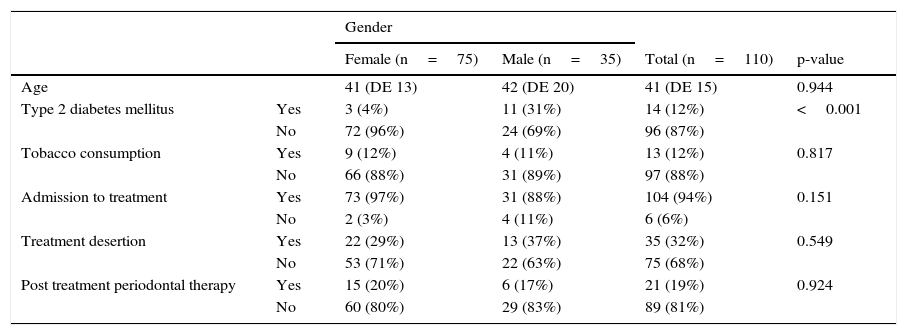
Demographic characteristics of patients. Age average in years and frequency distributed according to gender (female, male) type II diabetes mellitus (type II DM), tobacco consumption, patients admitted to treatment, patients deserting treatment during follow-up year, and patients who were admitted to post treatment periodontal therapy (PTPT).
| Gender | |||||
|---|---|---|---|---|---|
| Female (n=75) | Male (n=35) | Total (n=110) | p-value | ||
| Age | 41 (DE 13) | 42 (DE 20) | 41 (DE 15) | 0.944 | |
| Type 2 diabetes mellitus | Yes | 3 (4%) | 11 (31%) | 14 (12%) | <0.001 |
| No | 72 (96%) | 24 (69%) | 96 (87%) | ||
| Tobacco consumption | Yes | 9 (12%) | 4 (11%) | 13 (12%) | 0.817 |
| No | 66 (88%) | 31 (89%) | 97 (88%) | ||
| Admission to treatment | Yes | 73 (97%) | 31 (88%) | 104 (94%) | 0.151 |
| No | 2 (3%) | 4 (11%) | 6 (6%) | ||
| Treatment desertion | Yes | 22 (29%) | 13 (37%) | 35 (32%) | 0.549 |
| No | 53 (71%) | 22 (63%) | 75 (68%) | ||
| Post treatment periodontal therapy | Yes | 15 (20%) | 6 (17%) | 21 (19%) | 0.924 |
| No | 60 (80%) | 29 (83%) | 89 (81%) | ||
Type 2 DM rate was 4% in women and 31% in men (p<.001). The rest of used variables did not exhibit significant differences between male and female gender (Table I).
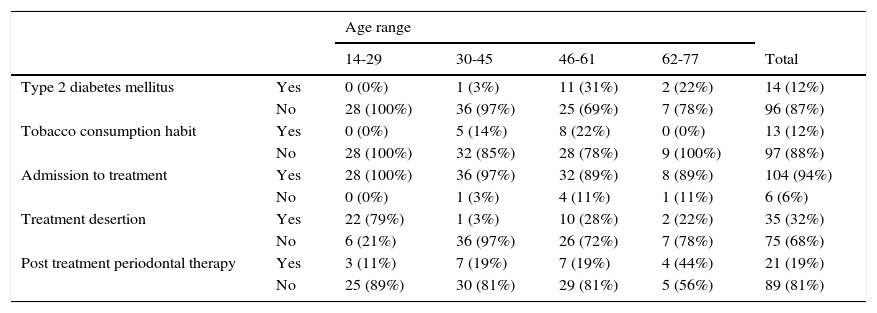
With respect to frequency distributed according to age rank (Table II), the highest concentration of patients registered for treatment was found between ages 30 and 45 years (36 patients), followed by 46 to 61 years (32 patients). There was no difference in age range with respect to type II DM presence, tobacco consumption habit or admission to PTPT. It is important to note that patients in the youngest age range were the ones who abandoned periodontal treatment in higher numbers (79%).
Frequency distributed by age range on type 2 DM, tobacco consumption habit, patients admitted to periodontal treatment, patients who deserted periodontal treatment and patients admitted to post treatment periodontal therapy (PTPT).
| Age range | ||||||
|---|---|---|---|---|---|---|
| 14-29 | 30-45 | 46-61 | 62-77 | Total | ||
| Type 2 diabetes mellitus | Yes | 0 (0%) | 1 (3%) | 11 (31%) | 2 (22%) | 14 (12%) |
| No | 28 (100%) | 36 (97%) | 25 (69%) | 7 (78%) | 96 (87%) | |
| Tobacco consumption habit | Yes | 0 (0%) | 5 (14%) | 8 (22%) | 0 (0%) | 13 (12%) |
| No | 28 (100%) | 32 (85%) | 28 (78%) | 9 (100%) | 97 (88%) | |
| Admission to treatment | Yes | 28 (100%) | 36 (97%) | 32 (89%) | 8 (89%) | 104 (94%) |
| No | 0 (0%) | 1 (3%) | 4 (11%) | 1 (11%) | 6 (6%) | |
| Treatment desertion | Yes | 22 (79%) | 1 (3%) | 10 (28%) | 2 (22%) | 35 (32%) |
| No | 6 (21%) | 36 (97%) | 26 (72%) | 7 (78%) | 75 (68%) | |
| Post treatment periodontal therapy | Yes | 3 (11%) | 7 (19%) | 7 (19%) | 4 (44%) | 21 (19%) |
| No | 25 (89%) | 30 (81%) | 29 (81%) | 5 (56%) | 89 (81%) | |
With respect to type II DM risk factor and treatment desertion, no significant dependence was observed (p>0.05) in the rate of patients with type II DM and treatment desertion (Figure 1). Moreover, no significant dependence was found (p>0.05) in rate of patients with type II DM and tobacco consumption habit (Figure 2).
 in rate of patients with type 2 DM and desertion rate.")
 in rate of type 2 DM patients and tobacco consumption habit.")
Statistically significant differences (p=0.002) were found in average age of patients with type II DM, 39.5 (SD 15.3) years, when compared to patients lacking type II DM which exhibited average age of 54.2 years (SD 6.8) (Figure 3). In results, statistically significant differences were found (p>0.001) in age rank of DM patients and periodontal treatment desertion. Average age of diabetic patient deserting treatment was 33.2 years (SD 17.7) whereas average age of patient lacking type II DM was 45.2 (SD 12.4) years (Figure 4)
 years, whereas diabetes-free patients exhibited 54.2 (SD 6.8) years. Differences were statistically significant (p=0.002).")
 whilst diabetes-free patients exhibited average of 45.2 (SD 12.4) years. Differences were statistically significant (p>0.001).")
Patients requesting periodontal specialty care characterization revealed that in the follow-up year, women attended more frequently periodontal treatment than men (Tables I and II), this evidence is in concordance with other research6,16 which indicated that women visited the dentist office more often,17 this is furthermore consistent with an American Academy of Periodontics report which stated than males exhibited less positive attitude towards dental visits.17
In both genders (Tables I and II) there was no difference with respect to tobacco consumption, attendance to periodontal treatment, treatment desertion, and follow-up during PTPT phase. Nevertheless, there was evidence of higher susceptibility to disease in patients who did smoke; this could be due to systemic effects which impacted on immune response and caused more severe clinical risk of periodontal disease.11,12 Moreover there are different biological circumstances among males and females.4 In this respect our results were relevant since they revealed significant differences in type II DM rate. Even though this research is a novel study never before undertaken, it is important to recognize there were limitations to state that it would be a characterization which would strictly represent patient's systemic or periodontal disease or health circumstances: the degree of tobacco use of periodontal patients must be studied as well as glycemic control. Nevertheless, our research can be considered a starting point for further scientific projects which might involve wider samples and include the whole of the Petorca Province, and, if possible, the Valparaiso Region in Chile.
Another important aspect in the undertaken characterization when compared to other research projects were results obtained in patients’ age ranks (Table II).18–20 Patients aged 30 to 61 years requested greater inclusion in treatment. It is relevant to note that the greater rate of periodontal desertion was observed in younger patients. Therefore, in the Petorca Province of Chile, it would be necessary to further promote dental care at early ages.
Deeper analysis of patients requesting treatment at the Periodontics Specialty and type II DM patients, revealed, when compared to non-diabetic patients, a statistically significant difference in two factors: average age and average age of patient deserting periodontal treatment (Figures 3 and 4). It was interesting to observe that type II DM patients were younger, and deserted treatment at earlier stages. The aforementioned results can be used in future periodontal treatments which might promote multidisciplinary follow-up with medical control, since, according to nation-wide study,21 in Chile, diabetes prevalence results are 7.5%, and this figure is rising. Therefore, it can be deemed necessary to promote early detection of diabetes and periodontitis, and create links among dental and medical professionals in the treatment of diabetic patients. This is particularly necessary when there is evidence sustaining the fact that glycemic control of a patient can impact in more favorable periodontal health circumstances.8,9