


The aim of the present study was to assess prevalence of maxillary sinus pneumatization and its relationship to loss of adjacent teeth, in a geriatric Peruvian population treated at a geriatric center recognized for the comprehensive medical care it provides to elderly patients.
Material and methodsA sample of 60 panoramic X-rays were gathered from the dental service of the Military Geriatric Clinic at Chorrillos. Millimeter count of maxillary sinus pneumatization was conducted with a standardized millimeter template.
ResultsFrom a total of 60 X-rays, 51 were selected for the study. Grade 4 pneumatization was observed (50%) in the mesial wall, grade 4 pneumatization was observed in the medial wall (57.1%) and grade 3 pneumatization was observed in the distal wall (64.7%).
ConclusionsBased on results of the present study it could be concluded that there was higher maxillary sinus pneumatization degree when there were at least two teeth adjacent to the edentulous side.
El objetivo de este estudio fue evaluar la prevalencia de neumatización del seno maxilar y la relación con la pérdida de piezas adyacentes, en la población peruana geriátrica de un centro reconocido por la atención médica integral a los pacientes adultos mayores.
Material y métodosSe recogieron como muestras 60 radiografías panorámicas del Servicio de Odontología de la Clínica Geriátrica Militar de Chorrillos. El conteo de milímetros de la neumatización del seno maxilar fue mediante una plantilla milimetrada estandarizada.
ResultadosDe las 60 radiografías se obtuvieron 51 para el estudio. La neumatización fue grado 4 de neumatización (50%) en la pared mesial, grado 4 de neumatización (57.1%) en la pared medial y grado 3 de neumatización en la pared distal (64.7%).
ConclusionesA través de los resultados de este estudio se pudo concluir que la pérdida de piezas dentarias afecta a la neumatización del seno maxilar. Según los resultados de este estudio se encontró el mayor grado de neumatización del seno maxilar cuando había por lo menos dos piezas dentarias adyacentes al lado edéntulo.
Premature tooth loss and lack of prosthetic rehabilitation is one of the greatest current dental problems. Loss of upper posterior teeth causes bone loss due to osteoclastic activity initiated from the maxillary sinus membrane after extraction, when bone mass of the maxillary sinus becomes very limited.1
In order to elevate maxillary sinuses by means of lateral or intra-alveolar techniques with use of biomaterial, it is necessary to always have as a reference point the distance from the ridge to the maxillary sinus obtained in panoramic X-rays and/or tomographies.1,2
According to some authors, vertical distortion observed in panoramic X-rays can be lesser than 30%. There is no existing standard for all panoramic equipment, nevertheless it can be used as an initial diagnosis element.2
Radiographic analyses templates used to calculate implant's optimal length and distributed by different commercial brands, pre-assume a 25% distortion in panoramic X-rays.3 Thus it is proposed to study this anatomical trait before using dental implants as treatment of partial edentulism in a Peruvian geriatric population. Classification of different maxillary sinus floor elevation techniques depends on the residual bone existing between alveolar crest and floor of the sinus, as described by Misch.4
The purpose of the present study was to evaluate prevalence of pneumatization of the maxillary sinus, to assess relationships between maxillary sinus pneumatization and gender, as well as existing relationship with loss of adjacent teeth in a geriatric Peruvian population treated at a center recognized for providing comprehensive medical care to elderly patients.
MATERIAL AND METHODSInitial sample was composed of 60 panoramic X-rays taken at the dental service of the Military Geriatric Clinic of Chorillos, Peru. Using inclusion and exclusion criteria, 9 X-rays were excluded from the present study since they showed loss of alveolar ridge. Inclusion criteria were the following: fully preserved X-rays with optimum development process, belonging to patients of both genders with partial or total edentulism, X-rays from the same imaging center, upper edentulous spaces in the premolar and molar area with 0 to 3 teeth adjacent to the maxillary sinus. Exclusion criteria were the following: X-rays belonging to patients with Sibert II residual ridge defect (horizontal shape).
Millimeter count of maxillary sinus pneumatization was performed with a standardized millimeter template, and was noted in a data collection chart. This chart included the following data: patient’ s number and gender, type of edentulism (partial or total edentulism), amount of millimeters of maxillary sinus ridge on mesial, middle and distal sides, to the residual alveolar ridge, count of number of teeth adjacent to the maxillary sinus. Data were assessed with statistical program SPSS version 3.0. Measurements of pneumatization grade of the three walls of the maxillary sinus were mathematically calculated a second time, following a statistical formula according to distortion grade horizontally exhibited in a panoramic X-ray. According to measurement, X-rays were grouped into four grades: grade 1: distance of alveolar ridge to maxillary sinus wall of 12 to 20mm, grade 2: distance of alveolar ridge to maxillary sinus wall of 8 to 12mm, grade 3 distance of alveolar ridge to maxillary sinus wall of 5 to 8mm, grade 4 distance of alveolar ridge to maxillary sinus wall lesser than 5mm. Graphs and tables were obtained to relate variables in order to achieve results.
RESULTSFor the present research study all samples were analyzed, 51 valid elements were conformed. They were grouped according to the patient's gender; it was found that the number of panoramic X-rays for male patients was greater (56.9%) than that of female gender (Table I).
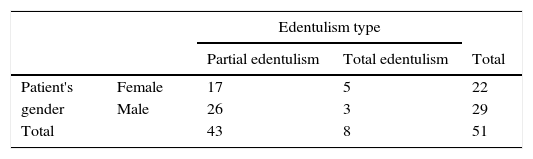
Table II show that the most frequent edentulism type was partial edentulism, most frequently found in males (26 cases out of a total 43).
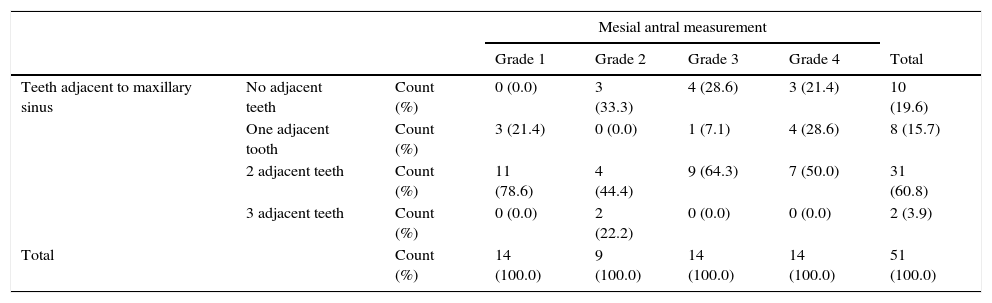
Number of teeth adjacent to edentulous space was grouped according to maxillary sinus pneumatization degree of each studied wall (mesial, medial and distal sides).
Table III shows that grade 4 was the greater pneumatization found in the antral mesial wall (50%) and that these cases exhibited two teeth adjacent to the edentulous side (Table III).
Number of adjacent teeth according to pneumatization grade of maxillary sinus in the mesial antral wall.
| Mesial antral measurement | |||||||
|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Total | |||
| Teeth adjacent to maxillary sinus | No adjacent teeth | Count (%) | 0 (0.0) | 3 (33.3) | 4 (28.6) | 3 (21.4) | 10 (19.6) |
| One adjacent tooth | Count (%) | 3 (21.4) | 0 (0.0) | 1 (7.1) | 4 (28.6) | 8 (15.7) | |
| 2 adjacent teeth | Count (%) | 11 (78.6) | 4 (44.4) | 9 (64.3) | 7 (50.0) | 31 (60.8) | |
| 3 adjacent teeth | Count (%) | 0 (0.0) | 2 (22.2) | 0 (0.0) | 0 (0.0) | 2 (3.9) | |
| Total | Count (%) | 14 (100.0) | 9 (100.0) | 14 (100.0) | 14 (100.0) | 51 (100.0) | |
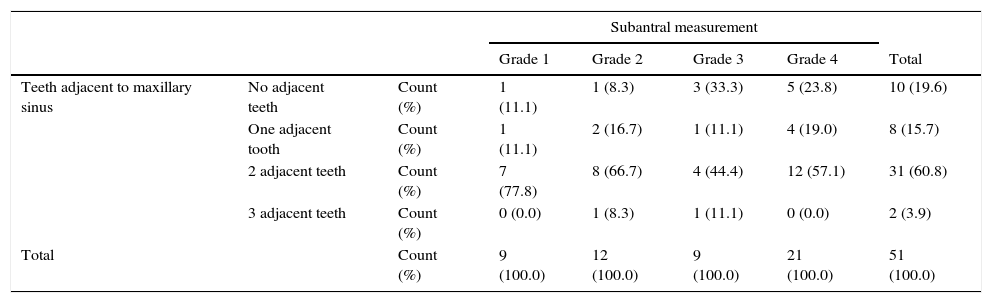
Table IV recorded that patients with greater grade 4 pneumatization frequency in the sub-antral wall (medial side) of the maxillary sinus were those possessing two teeth adjacent to the edentulous space; they reached 57.1% percentage (Table IV).
Number of adjacent teeth according to pneumatization grade of the maxillary sinus in the sub antral wall.
| Subantral measurement | |||||||
|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Total | |||
| Teeth adjacent to maxillary sinus | No adjacent teeth | Count (%) | 1 (11.1) | 1 (8.3) | 3 (33.3) | 5 (23.8) | 10 (19.6) |
| One adjacent tooth | Count (%) | 1 (11.1) | 2 (16.7) | 1 (11.1) | 4 (19.0) | 8 (15.7) | |
| 2 adjacent teeth | Count (%) | 7 (77.8) | 8 (66.7) | 4 (44.4) | 12 (57.1) | 31 (60.8) | |
| 3 adjacent teeth | Count (%) | 0 (0.0) | 1 (8.3) | 1 (11.1) | 0 (0.0) | 2 (3.9) | |
| Total | Count (%) | 9 (100.0) | 12 (100.0) | 9 (100.0) | 21 (100.0) | 51 (100.0) | |
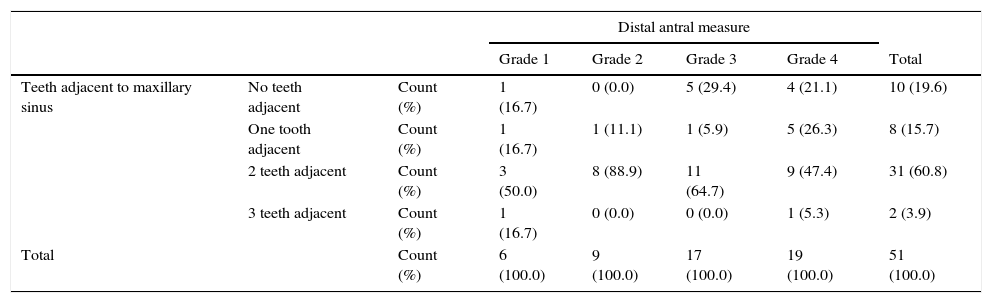
In table V, Patients with grade 3 maxillary sinus distal wall pneumatization were the most frequent; they exhibited two teeth adjacent to the space, representing 64.7% of the total (Table V).
Number of adjacent teeth according to pneumatization level of the maxillary sinus in the distal/antral wall.
| Distal antral measure | |||||||
|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Total | |||
| Teeth adjacent to maxillary sinus | No teeth adjacent | Count (%) | 1 (16.7) | 0 (0.0) | 5 (29.4) | 4 (21.1) | 10 (19.6) |
| One tooth adjacent | Count (%) | 1 (16.7) | 1 (11.1) | 1 (5.9) | 5 (26.3) | 8 (15.7) | |
| 2 teeth adjacent | Count (%) | 3 (50.0) | 8 (88.9) | 11 (64.7) | 9 (47.4) | 31 (60.8) | |
| 3 teeth adjacent | Count (%) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 1 (5.3) | 2 (3.9) | |
| Total | Count (%) | 6 (100.0) | 9 (100.0) | 17 (100.0) | 19 (100.0) | 51 (100.0) | |
Oral health professionals must establish as first and foremost consideration a global assessment of the patient. Evaluation of general health circumstances must be thoroughly and competently established, bearing in mind that elderly population is afflicted by several age-related conditions. From the diagnostic point of view, oral exploration must be comprehensive and methodized, therefore, it is important to assess amount of bone mass needed for future restorations.5–8 Residual alveolar processes (ridges) exhibit an anatomical structure called maxillary sinus, in order to analyze this anatomical structure as well as bone status, an X-ray study of the jaw (orthopantomography) must be achieved. In the case of implants, a tomography should be accomplished.8–12
Loss of upper teeth causes alveolar process resorption and maxillary sinus pneumatization.12–15 Use of oral implants has allowed solving tooth loss, nevertheless, when there is pneumatization of the maxillary sinus, bone availability decreases, hindering thus the process of implantation.
Diaz mentions that in a Peruvian population aged 17-32 years, 98.46% suffered less than five missing teeth. He also found that in a population aged 49-64 years, 37.78% suffered a loss of 5 to 10 teeth, and from the total of subjects aged 65 to 80 years, 35% suffered loss of 10 to 15 teeth.15
Osorio mentioned in his study on removable partial prosthesis planning that the 45-64 year old group represented 62.35% (n = 366) of total population, the 65 year old and over group represented 28.28% (n = 166). In the sample, average age was 58.06 ± 10.55 years.6 Upper dentures of the sample corresponded in greater percentage to Kennedy's class III, with 227 upper arches which corresponded to 38.60% of the total sample. Kennedy class II classification takes the second place of the greater to lesser percentage classification. Class I follows in this order with 16% of the total sample. This is to say that, in average, 81% of all subjects, when they reach 58 years of age, have lost teeth in the upper jaw, which might show a probability of maxillary sinus pneumatization.16
Tooth loss determines important functional and morphological changes in the cervical/mandibular cranial system. These changes can be observed at oral and extra-oral levels, extra-oral changes depend on location of the lost tooth. Main morphological oral changes are established by the progressive loss of height and thickness of the alveolar process. Resorption pattern of the alveolar process varies according to whether the lost tooth is in upper or lower location, since maxillary resorption pattern is described as centripetal, differing from mandibular resorption pattern which is described as centrifuge.17,18
In the lower jaw, dental arch exhibits different anatomical relationships depending on the tooth, 4 dental groups are recognized: a) with respect to the nasal cavity floor, these are mainly the incisor group, b) with respect to the canine abutment, it might be said through a lateral direction to the lateral wall of the nasal cavity and through a medial direction to the medial and anterior wall of the maxillary sinus, the canine tooth is described in this region, c) with respect to the maxillary sinus, this group comprises premolars and first and second molars, d) with respect to the tuberosity of the jaw, third molars are mainly found in this group. These anatomical relationships might vary according to the pnematization grade of the maxillary sinus; this situation is exacerbated when a tooth is lost, in which case pneumatization toward the sinus’ anterolateral wall as well as to the jaw's tuberosity are described. Thus, alveolar process height is altered due to alveolar resorption as well as pneumatization of the maxillary sinus.19
CONCLUSIONWe might say that, based on results collected in the present study, it could be proposed that tooth loss affects maxillary sinus’ pneumatization. According to results in the present study it was found that greater grade of maxillary sinus pneumatization could be observed when there were at least two teeth adjacent to the edentulous side.